
Abstract
Objective:
To investigate mother’s own milk (MOM) feeding rates in the first year of life after neonatal intensive care unit (NICU) discharge for infants born <37 weeks gestational age and compare rates by race and ethnicity.
Study Design:
This was a retrospective study of preterm infants discharged from the NICU who sought care at a primary care clinic within our academic health system. Infant demographic characteristics and feeding at NICU discharge were extracted from the medical record. Post-discharge feeding history was extracted from health care maintenance (HCM) visit records at 2, 4, 6, 9, and 12 months for infants born between January 2018 and December 2019. Exclusion criteria included having a contraindication to MOM feeding or insufficient feeding documentation.
Results:
Of the 314 infants meeting inclusion criteria, 57% received any MOM and 24% received exclusive MOM at NICU discharge. At the 6-month HCM visit, MOM feeding rates decreased to 25% for any MOM and 12% for exclusive MOM. Statistically significant racial and ethnic differences in MOM feeding rates were observed at all HCM visits, with White infants having the highest and Black infants having the lowest MOM feeding rates.
Conclusions:
MOM feeding rates decreased from NICU discharge to the 12-month HCM visit. Disparities observed during the birth hospitalization persisted after discharge, with Black infants having consistently lower MOM feeding rates compared with Hispanic and White infants. These disparities highlight research opportunities to pinpoint factors contributing to the decline in MOM feedings and develop targeted interventions to address these disparities.
Introduction
The benefits and protective effects of mother’s own milk (MOM; breast milk from the mother) for parents and infants of all gestational ages (GAs) have been well documented.1–5 The American Academy of Pediatrics (AAP) recommends exclusive MOM feedings for the first 6 months of life, with continuation along with complementary foods until two years of age or beyond, a recent increase from the previous recommendation of continuation through 1 year of age. 6 However, only one-quarter of infants in the United States receive exclusive MOM through 6 months of age, despite 83% of infants receiving MOM at the time of discharge from their birth hospitalization. 7
Despite documented benefits of MOM in reducing the incidence of neonatal morbidities, including necrotizing enterocolitis, 2 late-onset sepsis, 1 and bronchopulmonary dysplasia, 8 decreasing hospital readmission rates, 9 and improving neurodevelopmental outcomes for preterm infants (<37 weeks GA), 9 MOM rates may be lower for preterm compared with term infants. For example, U.S. birth certificate data from 2017 indicate that only 71% of extremely preterm infants received any MOM during the birth hospitalization compared with 85% of term infants, 10 and unadjusted data from the 2021 Pregnancy Risk and Monitoring System show lower rates of MOM provision at 12 weeks for preterm compared with term infants. 11 Furthermore, these differences in MOM rates are exacerbated by racial and ethnic disparities, with preterm infants in each racial and ethnic group being less likely to receive MOM compared with their term counterparts.10,12,13 However, other studies have reported similar or higher MOM feeding rates in very low birth weight (VLBW, birth weight <1,500 g) and preterm infants compared with those seen in term infants.14,15 Although disparities in MOM continuation to neonatal intensive care unit (NICU) discharge are well documented in the VLBW and very preterm (<32 weeks GA) populations,14,16 few studies have reported MOM continuation rates after NICU discharge,15,17 despite the recommendation for exclusive MOM feeding for the first 6 months of life. 6 Moreover, data are even more limited on MOM provision rates by socioeconomic status and race and ethnicity after NICU discharge for U.S. preterm infants. 18
Our objective was to evaluate MOM feeding rates during the first year of life among preterm infants born <37 weeks GA and cared for in an urban Level 3 NICU. We hypothesized that MOM feeding rates would be lower for non-Hispanic Black (Black) infants compared with non-Hispanic White (White) and Hispanic infants at each pediatrician visit (2, 4, 6, 9, and 12 months chronologic age). 16 This investigation aims to shed light on whether disparities in MOM provision persist at key milestones, providing insight to inform future interventions, public policies, and public health initiatives aimed at eliminating disparities in MOM provision and increasing MOM feeding rates for preterm infants.
Methods
Study sample
This was a retrospective review of electronic medical records (EMR) for preterm infants admitted to a Level 3 NICU of a large, urban academic medical center in Chicago, Illinois, USA, between January 1, 2018, and December 31, 2019. The study sample was limited to infants who were discharged home from the NICU and completed at least one health care maintenance (HCM) visit between birth and 12 months at either of the two general pediatric clinics at the academic health system. These pediatric clinics had similar lactation support available. Infants were excluded from the study if they had a contraindication to MOM feeding or if they were transferred to the general care nursery before discharge from the birth hospitalization. In addition, one subject was excluded due to missing race or ethnicity. The study was reviewed and deemed exempt by the institutional review board at Rush University Medical Center.
MOM feeding duration
Feeding history was retrospectively retrieved from the EMR at NICU discharge and at the 2-, 4-, 6-, 9-, and 12-month HCM visits. Feeding at NICU discharge was determined by nursing documentation of feedings on the day of discharge and the full 24-hour calendar day before discharge.
Feeding history from the HCM visits was extracted from the physician’s note as reported by the parent or guardian at each visit, including whether the infant was receiving MOM, formula, or both. If documentation did not specify whether the infant was receiving MOM or formula, data for that visit were reported as missing. Two MOM feeding variables were created for each time point. The first was a dichotomous variable indicating whether the infant was receiving any MOM. The second was a dichotomous variable for exclusive MOM, coded as “yes” if the infant was receiving MOM and not receiving formula, irrespective of receiving complementary foods. The route of MOM feeding (direct breastfeeding versus bottle) was not collected.
Independent variables
Independent variables included infant sex (male, female), race, ethnicity, insurance at the birth hospitalization (commercial insurance, Medicaid), mode of delivery (cesarean delivery, vaginal delivery), birth GA (extremely preterm <28 0/7 weeks, very preterm 28 0/7–31 6/7 weeks, moderately preterm 32 0/7 to 33 6/7 weeks, late preterm 34 0/7 to 36 6/7 weeks), birth weight (<1,000 g, 1,000–1,499 g, 1,500–2,499 g, >2,500 g), NICU birth hospitalization length of stay (days), and completion of each HCM visit. Infant race and ethnicity were classified based on maternal self-report at the birth hospital admission (non-Hispanic Black [Black], Hispanic, non-Hispanic White [White]). Due to only one infant reported as Asian or another racial group, this infant was included in the White group. In addition, we calculated the number of days between the infant’s 1-year birth date and the 12-month HCM visit date to determine whether there were differences in the timing of visit completion by race and ethnicity.
Statistical analysis
Frequency distributions and medians (interquartile ranges) were used to describe the sample. Chi-squared tests were used to compare MOM feeding rates at each HCM visit by race and ethnicity. Binary logistic regression was used to test the association between race and ethnicity with any MOM and exclusive MOM at the 6-month HCM visit, controlling for infant characteristics (sex, GA, payer, delivery method, birth hospitalization length of stay, and whether all visits to 6 months were completed). Predicted probabilities were computed using the method of recycled predictions, where the probability of receiving MOM was computed for all infants assuming they were Hispanic, using observed values for all other characteristics, and then computing the average predicted probability for all infants assuming they were Black and White, respectively. Goodness of fit was assessed using the Hosmer–Lemeshow test, and predictive accuracy was assessed using the area under the receiver operating characteristic curve. In addition, we used a population averaged multivariable logistic regression model with robust standard errors and unstructured error correlations to test the association between race and ethnicity and receipt of MOM over time, including time-invariant covariates described above.
Secondary analyses were performed to test the association between race and ethnicity and receipt of MOM, conditional on receiving any MOM at NICU discharge, to examine disparities in continued MOM provision post-NICU hospitalization. Excel for Microsoft 365, SAS version 9.4 (Cary, North Carolina), and Stata version 17 (College Station, Texas) were used for data management and analysis.
Results
Of the 1,054 charts reviewed, 314 met inclusion criteria. The most common reasons for exclusion from the analysis were follow-up outside of the hospital system’s pediatric clinics and transfer to the general care nursery before discharge from the birth hospitalization. The sample was predominantly Black (50%) or Hispanic (32%), with 61% having Medicaid. Overall, 51% of infants were born late preterm (Table 1). A total of 121 (39%) infants completed all HCM visits with complete feeding data at all time points. Differences in sociodemographic characteristics between infants who completed all HCM and infants who missed at least one HCM visit were evident (Supplementary Table S1). Of infants who missed at least one HCM visit, 57.5% completed the 6-month visit and 44% completed the 12-month visit (Supplementary Table S2). At NICU discharge, 57% received any MOM and 24% received exclusive MOM. At the 6-month HCM visit, MOM feeding rates decreased to 25% for receiving any MOM and 12% for receiving exclusive MOM (Table 2).
Description of the Sample, N = 314
NICU, neonatal intensive care unit.
Any and Exclusive Breast Milk at NICU Discharge and Each HCM Visit
HCM, health care maintenance; MOM, mother’s own milk.
Any and exclusive MOM feeding rates were highest for White infants, followed by Hispanic and Black infants at every HCM visit (Supplementary Table S3). Notable differences were observed at NICU discharge, with 84% of White infants receiving any MOM compared with 62% of Hispanic infants and 44% of Black infants, with decreased rates among all infants at the 2-month HCM visit, most pronounced in Black infants.
After adjusting for infant characteristics, there was no difference in the likelihood of receiving any MOM at the 6-month HCM visit between Hispanic and Black infants (Table 3). White infants were thrice as likely to receive any MOM compared with Black infants (odds ratio = 3.07, 95% confidence interval [CI], 1.22–7.72), translating into predicted probabilities of any MOM at the 6-month HCM visit of 19.1%, 23.9%, and 36.6% for Black, Hispanic, and White infants, respectively. However, by limiting the analysis to those receiving MOM at NICU discharge, racial and ethnic differences in MOM rates at 6 months were no longer statistically significant (Supplementary Table S4). Differences in exclusive MOM at the 6-month HCM visit were not significant, with predicted probabilities of 6.8%, 15.5%, and 15.6%, respectively. In addition, significant differences in MOM feedings were found between infants with commercial versus Medicaid coverage, with 42.1% probability of any MOM for infants with commercial insurance compared with 11.6% of infants with Medicaid.
Logistic Regression Results for MOM at the 6-Month HCM Visit, N = 232
Models control for infant sex, gestational age at birth categories, delivery method, birth hospitalization length of stay, and whether all visits to 6 months or 12 months were completed.
Area under the receiver operating characteristic curve: Any MOM at 6 months, 0.81; exclusive breast milk at 6 months model, 0.80.
95% CI, 95% confidence interval.
In the repeated measures analysis of any MOM feeding through 12 months for the entire cohort (N = 314), White infants were significantly more likely than Black infants to receive any MOM at each time point. Differences in the rates for Hispanic versus White infants, as well as Black versus Hispanic infants, were significant at only the 2-month and 4-month visits. In addition, adjusted rates of any MOM among infants with commercial insurance were significantly higher than rates for infants with Medicaid at each time point (Table 4). For all three groups, MOM rates decreased between NICU discharge and the 12-month visit, with MOM rates for White infants consistently higher than for Hispanic and Black infants (Fig. 1). In addition, infants with commercial insurance were significantly more likely to receive MOM at every time point compared with infants with Medicaid. In our secondary analysis limited to infants who completed all routine HCM visits (N = 121), MOM feeding trajectories between NICU discharge and the 12-month HCM visit were similar to the results for all infants, showing White infants having the highest rates of MOM feedings at every time point, followed by Hispanic and Black infants, respectively (Supplementary Table S5). However, differences between White and Black infants were only significant at the 2-, 4-, and 9-month HCM visits.
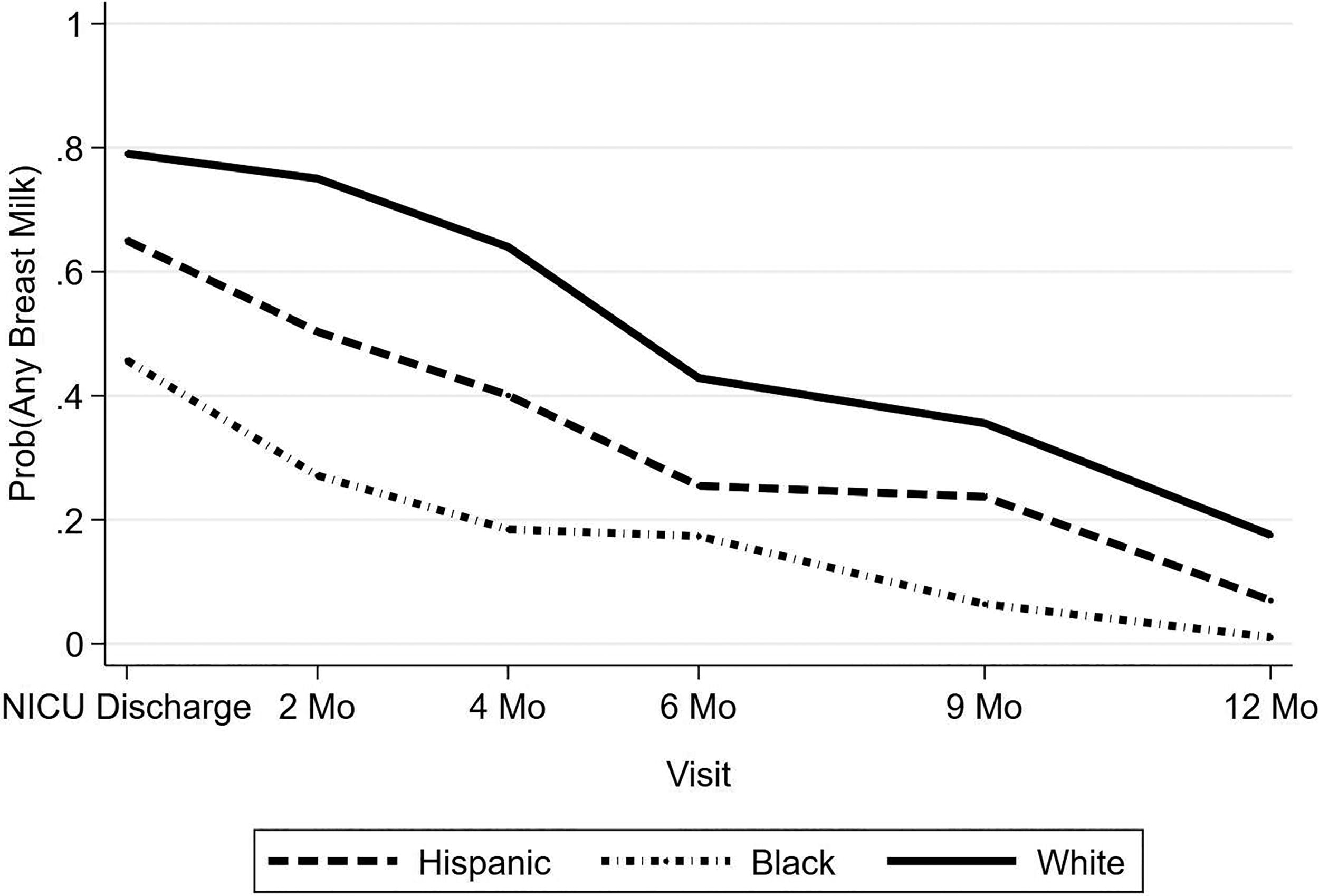
Predicted probability of any MOM at NICU discharge and each HCM visit through 12 months. The predicted probability was calculated using the method of recycled predictions. HCM, health care maintenance; MOM, mother’s own milk; NICU, neonatal intensive care unit.
Repeated Measures Results for Any MOM at NICU Discharge and HCM Visits, N = 314
Results from population averaged repeated measures logistic regression model, controlling for infant sex, gestational age at birth, delivery method, birth hospitalization length of stay, visit, interaction term for visit and race/ethnicity, and whether all visits to 12 months were completed. N = 1,424 completed visits with feeding data.
Black White rates significantly different.
Black Hispanic rates significantly different.
Hispanic White rates significantly different.
Commercial-medicaid rates significantly different.
Discussion
Despite the known health benefits of MOM for the infant and mother,1,3–5,8 rates of MOM provision decline after birth hospitalization in the United States. National data from 2021 show that 88% of mothers initiate MOM provision overall, and 68% of these mothers continued to provide MOM at 3 months, 11 whereas only 55% of infants receive any MOM at 6 months of age. 19 Preterm infants are a vulnerable population even after NICU discharge and are at increased risk for readmission in the first year of life, 20 and MOM feedings have been associated with decreased risk of readmissions. 9 Our data demonstrate a steep decline in MOM provision rates by the 6-month HCM visit, with only 25% of infants receiving any MOM and 12% receiving exclusive MOM, far below the AAP recommendations for MOM feedings. 6
Our 6-month MOM provision rate was similar to findings of the study by Ellis et al. of infants (86% born preterm) discharged from the NICU and seen at high-risk follow-up clinics between 2015 and 2017. 15 They found that MOM feeding rates decreased sharply, from 73% at discharge to 30% by 6 months of age. 15 Using more recent national data for infants of all GAs, Wilson et al. reported similar rates of MOM initiation and continuation at 3 months after birth for term compared with extremely and moderately preterm infants. However, they found a large difference in rates for late preterm compared with term infants, with 84% versus 88% of mothers of late preterm and term infants initiating MOM, respectively, and only 65% versus 71% continuing to provide MOM at 3 months after birth. 11 These findings are concerning as late preterm infants account for the largest proportion of preterm infants, 21 but have received fewer quality improvement interventions to increase MOM. Although they are generally healthier and more mature than their younger preterm counterparts, late preterm infants are at significantly heightened risk for neonatal morbidity and feeding issues compared with term infants.9,22,23
Even though MOM provision rates for preterm infants have improved over time in the United States,14,24 racial disparities persist.25,26 We found a disparity in MOM provision at NICU discharge for preterm infants that persisted over the first 12 months, with fewer Black preterm infants receiving any MOM compared with White preterm infants at all HCM visits. These results are consistent with disparities reported for term infants. 12 Given these racial disparities and an overall decline in MOM provision during the early post-NICU period, it is crucial to better understand why mothers discontinue MOM provision. Some barriers to MOM provision occur during the birth hospitalization, including a shortage of lactation specialists,16,27 and are compounded by racial disparities, including unequal access to services, implicit bias, and racial discrimination. 28 In addition, mothers of preterm infants face unique challenges, such as mother–infant separation, pump-dependency while their infant is in the NICU,18,29 and high-risk status of the former preterm infant after NICU discharge, often associated with parental concerns regarding oral intake and adequate weight gain and frequent medical appointments after discharge.
Decisions to provide MOM occur in the context of individual perceptions and cultural norms surrounding breast milk. Breastfeeding intention is positively associated with Hispanic ethnicity and recent immigration. 30 Aspects of African American history such as slavery and forced wet-nursing may negatively impact the provision of MOM in the African American community. 31 In addition, newer cultural influences, such as information from online sources and social media, play a role in shaping mothers’ perspectives on providing MOM. 32 Future studies should assess the impact of family, friends, and social media on the duration of MOM provision for preterm infants after NICU discharge.
Previous studies have shown that returning to work also impacts MOM provision, with returning to work, lack of paid leave, and short postpartum leave associated with earlier breastfeeding cessation. 33 Women may not disclose their breastfeeding status at their place of employment for fear of judgment or criticism, particularly when a workplace is viewed as not supportive. 34 Even in a supportive work environment, mothers may face barriers, such as lack of a convenient private space to pump MOM and a location to store MOM, 35 despite legal protections. 36 Furthermore, we also noted a significant income disparity, with lower MOM rates in infants born to mothers with Medicaid. Providing MOM while returning to work may be especially challenging for low-income mothers, given less flexibility in their jobs, and breastfeeding is viewed as limiting and less convenient. 37 Concerns over financial burdens are not unsubstantiated; breastfeeding greater than 6 months is associated with lower earnings through 5 years after birth. 38 Although often not considered, women also spend disproportionately more time on unpaid household work and childcare 39 and are more likely to take time off from work than men. This unpaid work extends to the period after NICU discharge when mothers are caring for their preterm infants. Although data on the complex relationship between MOM provision, paid work, and unpaid work are limited in the preterm population, 40 we theorize that MOM provision may be particularly difficult for low-income mothers.
Limitations
This study has several limitations. First, our study was limited to infants born at a single academic medical center located in a large metropolitan area. Due to a relatively large geographic catchment area, not all infants had a pediatrician within our hospital system, and therefore, we were not able to collect feeding data for all infants. In addition, among infants who had at least one HCM visit within our hospital system, many did not complete all visits, with only 44% completing the 12-month HCM visit. Further research is needed to determine whether these infants received follow-up care from pediatricians outside our hospital system or missed visits entirely and whether MOM provision differed for these infants. Infants of multiple births were included in the study, and while they comprised a very small portion of the study population, they were not differentiated from singleton births in the data analysis. In addition, infants born during the COVID-19 pandemic were intentionally excluded to avoid any confounding effects directly caused by the global pandemic, and therefore, our data reflect prepandemic MOM feeding rates. Due to the retrospective nature of the study, we were unable to collect data regarding reasons for discontinuation of MOM provision, which could have contributed to our understanding of drivers of racial disparities.
Conclusion
Our results extend prior findings by examining outcomes for a broader range of preterm infants admitted to our NICU, demonstrating that MOM provision declines over the first 12 months. Disparities in MOM feedings seen at NICU discharge continued through the first year of life for preterm infants, with a sharp decline during the 2- to 4-month period for Black and Hispanic infants, and the highest rates of MOM provision were observed in White infants at all HCM visits. Awareness of the timing of this decline is especially important for pediatricians to provide additional support for breastfeeding parents, specifically at NICU discharge and the 2-month visit. These disparities underscore the need for more research to identify factors contributing to the rapid decline in MOM provision and to develop strategies for supporting continued MOM provision among former preterm infants through two years of age.
Footnotes
Authors’ Contributions
N.L. helped design the study and collect data, coordinated and supervised data collection, analyzed data, drafted the initial article, and reviewed and revised the article. T.J.J. helped design the study and collect data, performed and interpreted data analysis, and reviewed and revised the article. A.L.P. contributed to the study design and methodology and reviewed and revised the article. M.D. collected data and contributed to the initial article. C.F. collected data and contributed to the initial article. K.D. collected data and contributed to the initial article. P.P.M. contributed to study design and reviewed and revised the article. S.K. conceptualized and designed the study, supervised data collection, and reviewed and revised the article. All authors approved the final article as submitted and agree to be accountable for all aspects of the work.
Data Sharing Statement
Data utilized for this study are available upon request to the corresponding author, contingent upon appropriate scientific query, data sharing agreement, and institutional review board approval.
Disclosure Statement
All authors report no disclosures of potential conflicts of interest.
Funding Information
Research reported in this publication was partially supported by internal funding from the RUSH Medical College Deans Professional Development Assistance Program awarded to Charlie Fischer. The study sponsor had no role in the following: (1) study design; (2) the collection, analysis, and interpretation of data; (3) the writing of the report; and (4) the decision to submit the article for publication.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.