
Abstract
Introduction:
Breast milk (BM) has numerous well-known, proven health benefits; however, the mechanisms underlying these effects are still not well-defined. Recent studies have shown that BM contains mesenchymal stem cells (MSCs), which might support both the growth and development of infants as well as provide protection from acute and chronic diseases. The effect of different conditions on the cellular components of BM is still unknown. This study focuses on investigating the influence of various storage methods on the properties of BM-derived MSCs.
Methods:
The study involved collecting 15 mL of BM samples from 17 participating mothers within the first week postpartum. MSC isolation was conducted on three sets of 5 mL samples from each participant: freshly obtained samples, refrigerated samples for 72 hours, and samples deep-frozen at −20°C for 1 month. Poststorage, MSCs were assessed for cell count, viability, and expression of specific markers using flow cytometry.
Results:
Analysis revealed a significant decrease in the average count of MSCs in BM poststorage. Freshly collected BM samples showed an average MSC count of 80.588,24 ± 50.0431,96, which significantly reduced to 28.333,33 ± 10.298,57 after 72 hours of refrigeration (p < 0.05). Despite this decrease, there was no notable change in the expression of MSC positive markers. Interestingly, MSCs were undetectable in samples stored in a deep freezer for one month upon microscopic examination.
Conclusion:
The study demonstrates a reduction in the viability of MSCs in BM when refrigerated, yet the surviving cells maintained their characteristic surface markers. However, freezing BM resulted in a complete loss of its MSC content.
Introduction
Breast milk (BM) is often considered a nutritionally rich and biologically active fluid essential for infant development. It contains various micro and macronutrients, pre and probiotics, cell types, immune-modulating molecules, hormones, and other protective elements.1–5 Its composition dynamically adapts to the specific needs of each infant.4,5 While BM’s numerous health benefits are well-documented, the mechanisms through which it confers immediate and long-term advantages, such as enhanced growth, neuromotor development, and protection against acute and chronic illnesses, must be fully understood.1,4
Mesenchymal stem cells (MSCs) are adult multipotent progenitor cells capable of differentiating into various cell types, including neurons, myoblasts, adipocytes, osteoblasts, and chondroblasts. 6 MSCs are particularly valued in regenerative medicine due to their postnatal origin, differentiation capacity, immune-privileged status, and safety for the host. 7 They also possess significant immunomodulatory, anti-inflammatory, and immunosuppressive properties, enabling them to regulate injured tissue microenvironments.8–10 Clinically, MSC-based therapies are being explored for conditions such as Alzheimer’s and Parkinson’s disease.7–11 While MSCs are commonly derived from peripheral blood, bone marrow, adipose tissue, and dental tissues,9–11 recent advancements have identified perinatal tissues, including the umbilical cord, placenta, amniotic fluid, and BM, as promising MSC sources.10–14
BM is known to harbor a heterogeneous mix of cells, including epithelial cells, immune cells, and hematopoietic stem cells, and is particularly rich in MSCs.15,16,39,40 Cregan et al. first reported the discovery of stem cells in BM in 2007. 17 The following research confirmed the presence of multipotent MSCs in BM, identifiable by surface markers such as CD44, CD73, CD90, and CD105.6,9,14 These stem cells are thought to be crucial in benefiting the infant, interacting via cell-to-cell contact (through receptors) and secreted mediators. 18 Such interactions are hypothesized to be key to understanding BM’s unexplained health benefits.19–24
Recent research highlights the adverse impact of preterm birth on progenitor and stem cells across multiple critical tissues and organs, primarily due to the loss of maternal and placental growth factors and exposure to postnatal oxidative stress.21,22 These disruptions increase the risk of morbidities such as bronchopulmonary dysplasia (BPD), intraventricular hemorrhage (IVH), and necrotizing enterocolitis (NEC).25,26 MSCs have shown promise as a therapeutic strategy for these conditions, supported by encouraging animal study results. 27 For instance, BM-derived MSCs (BM-MSCs) differentiated into neurogenic precursor cells have effectively reduced inflammation, apoptosis, ischemia, and necrosis in mice with spinal cord injuries.8,12,25,28 Clinically, intranasal administration of BM-MSCs in preterm infants with IVH significantly reduced complications such as ventricular dilatation and hydrocephalus, decreasing the need for surgical interventions. 26 Moreover, Chang et al. reported that intratracheal administration of umbilical cord-derived MSCs to preterm infants reduced the severity of BPD. Over a 2-year follow-up, infants receiving MSC therapy exhibited fewer BPD-related complications than those without MSC treatment.29,30
In certain situations, mothers may be unable to breastfeed their newborns due to social or medical reasons. In intensive care units, feeding may be delayed or interrupted due to infants’ clinical conditions. For these medically fragile infants, BM is essential.18,19 To ensure its availability, mothers often express and store excess BM for later use, keeping it in refrigerators at +4°C for short-term storage or in deep freezers at −20°C for extended periods. Research has shown that the biological and immunological components of BM can be affected by storage conditions. 31 This study aims to be the first to evaluate how refrigeration and profound freezing impact the count, viability, and immunological properties of BM-MSCs.
Methods
Collection of BM samples
Conduct of the Study: This research was carried out from June 1, 2019, to September 1, 2019, at the Neonatal Nursery and Newborn Outpatient Clinics of Marmara University Pendik Training and Research Hospital.
BM samples were collected from 17 mothers within the first week postpartum, including 1 late preterm, 1 early term, and 15 term infants. Each mother provided 15 mL of BM, divided into three portions: 5 mL analyzed fresh, 5 mL refrigerated for 72 hours, and 5 mL frozen at −20°C for 1 month before thawing and analysis (Table 1). Due to limited availability, only 12 BM samples were included in the final statistical analysis. All mothers provided informed written consent, with demographic data detailed in Tables 2 and 3. BM was collected via hand-expression under strict hygienic conditions.
Inclusion and Exclusion Criteria
Characteristics of Mothers and Babies Participating in the Study-I
SGA, small for gestational age; LGA, large for gestational age; AGA, appropriate for gestational age.
Characteristics of Mothers and Babies Participating in the Study-II
BM, breast milk.
Isolation and characterization of MSCs from BM
MSCs were successfully isolated from BM. Initially, 5 mL of BM was mixed with an equal volume of phosphate-buffered saline (PBS) and centrifuged at 2,000 rpm for 10 minutes. The lipid layer was discarded, and the resulting cell pellet was resuspended in Dulbecco’s modified Eagle medium supplemented with antibiotics and antifungals. Cells were incubated at 37°C in a 5% CO2 atmosphere until 80–90% confluence was reached, with medium changes 2–3 times weekly. For subculturing, cells were detached using 0.25% trypsin-EDTA and counted using a hemocytometer, with trypan blue staining for viability assessment. Subsequent characterization in the third passage confirmed the expression of positive MSC markers CD73, CD90, and CD105 and the low expression of the negative hematopoietic marker CD44.
Functional characterization: in adipogenic differentiation, cells were cultured in an adipogenic medium and later fixed with 10% formaldehyde, followed by Oil Red O staining, which revealed lipid droplet formation under the microscope. For osteogenic differentiation, cells were cultured on type I collagen-coated lamellae in an osteogenic medium for 21 days. After fixation, cells were stained with Alizarin Red, indicating calcium deposition. In chondrogenic differentiation, cells were cultured on type I collagen-coated lamellae in a chondrogenic medium for 21 days, fixed, and stained with Alcian Blue, revealing proteoglycan formation and chondrocyte presence under microscopy (Figure 3).
Storage conditions and culture of BM samples
BM samples were subjected to different storage conditions—kept fresh, stored at +4°C for 72 hours, and at −20°C for 1 month—before isolating MSCs using the protocol outlined in “Isolation and Characterization of MSCs from Breast Milk.” Postisolation, the cells were cultured on coverslips in 6-well plates for 72 hours at 37°C in a humidified 5% CO2 atmosphere until they reached the third passage. A 0.25% trypsin-EDTA solution was used for cell detachment, followed by sequential washing with culture medium and PBS. The cells were centrifuged and prepared for subsequent Annexin V and surface marker analysis.
Detection of cell viability and surface markers expressions
Cell viability and surface marker expression were evaluated after the designated culture period. The cells were stained with Annexin V (FITC) (BD Biosciences, USA) for viability assessment. For surface marker analysis, cells were stained with anti-human-CD73, anti-human-CD90, and anti-human-CD105 to identify positive markers and with anti-human-CD44 for negative marker identification. The staining procedure was conducted for 15 minutes at room temperature in a dark environment. Flow cytometry was utilized to analyze the stained cells. The results were quantified and presented as mean fluorescence intensity or percentage (%) of the total cell population.
Statistical analysis
Statistical evaluations were conducted using SPSS software, version 17.0. Descriptive statistics were presented in terms of mean, standard deviation, and median values. The Wilcoxon test was applied to assess variations for variables not following a normal distribution (nonparametric). The Spearman correlation test was utilized to analyze the relationships between measurement data. A p value of less than 0.05 was deemed indicative of statistical significance.
Results
The study determined the average count of MSCs isolated from 17 fresh BM samples. The count for freshly obtained samples was 80.588,24 ± 50.431,96 cells/mL, while for the 12 samples stored at +4°C for 72 hours, the count was 28.333,33 ± 10.298,57 cells/mL, as detailed in Tables 4 and 5.
Mean and Median Values of MSC Counts, Viability and Markers in Fresh Breast Milk
MSC, mesenchymal stem cell.
Comparison of MSC Values from Fresh and Refrigerated Breast Milk for 72 Hours with Wilcoxon Test
BM, breast milk; MSC, mesenchymal stem cell.
The comparative analysis of cell count, viability, and expression of positive markers (CD73, CD90, and CD105) was conducted between 7 fresh and 12 stored BM-MSC samples using the Wilcoxon statistical method. A significant reduction in the number of viable cells was observed in the stored samples compared with the fresh samples (p < 0.05), as detailed in Table 5.
Furthermore, no viable cells were detected in the BM samples stored at −20°C and subsequently thawed. In contrast, the expression levels of positive MSC markers remained unchanged in the samples stored at +4°C (Figs. 1–2).
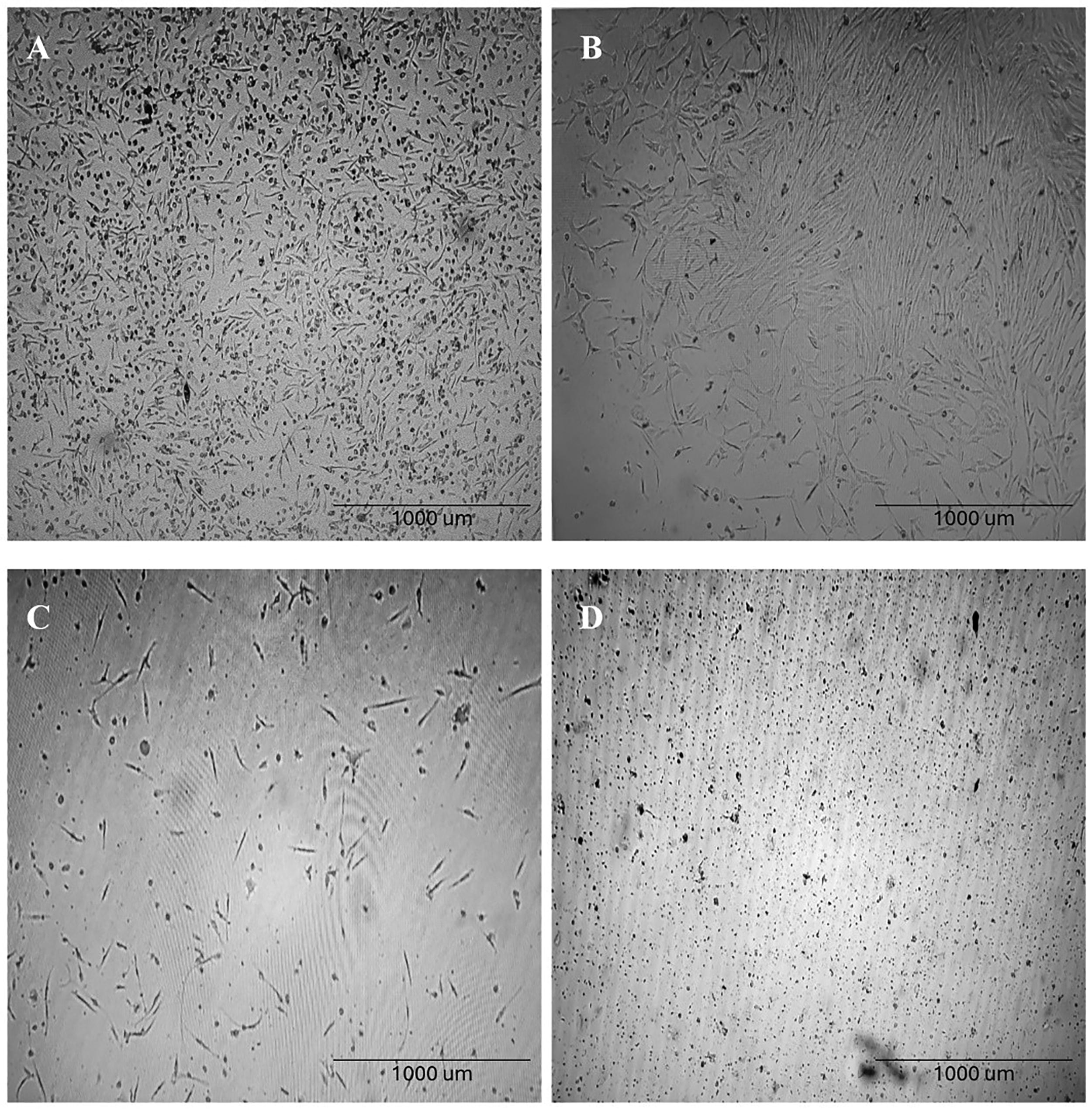
Morphological images of breast milk-derived stem cell cultures:
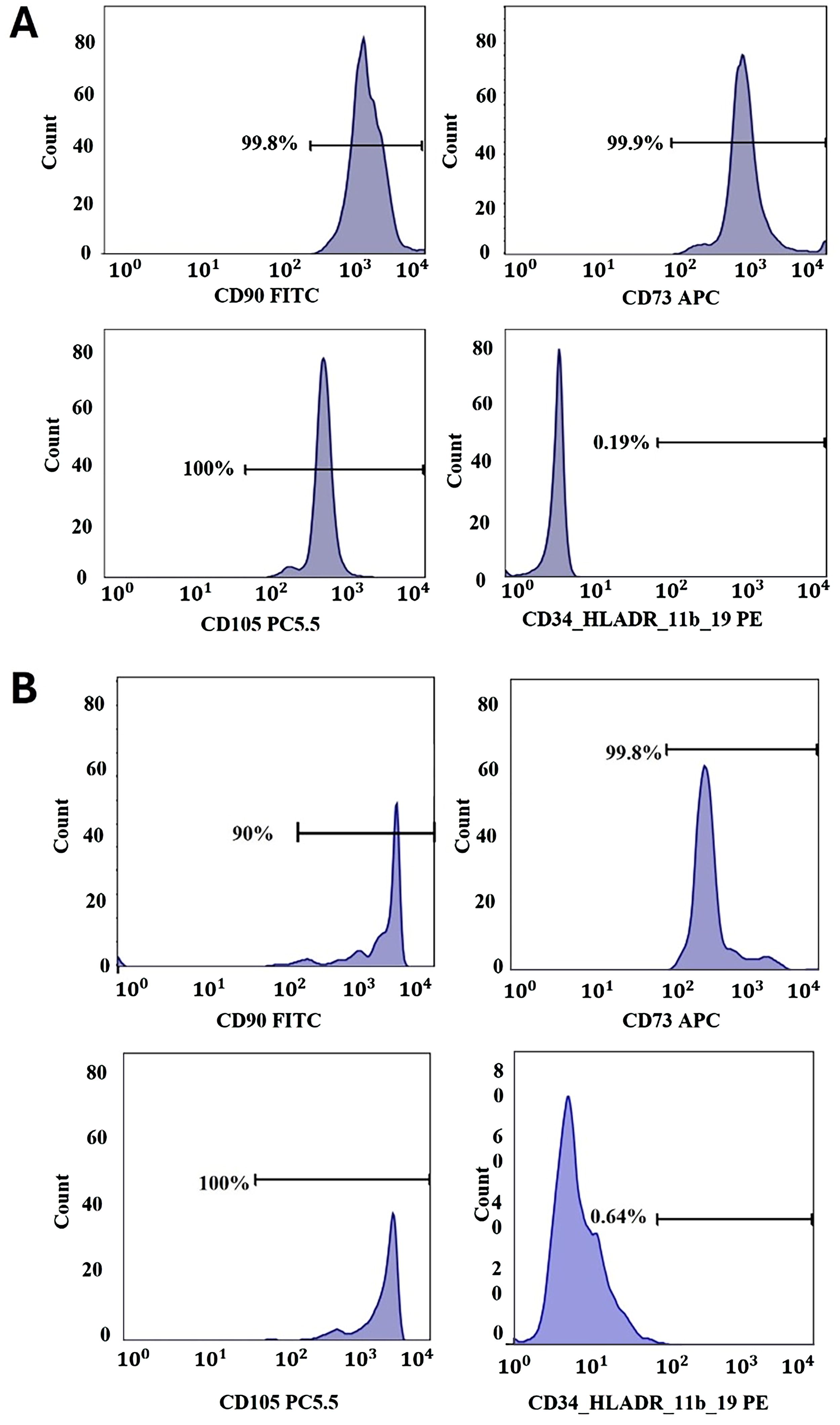
Gate strategy of MSCs isolated from fresh BM-MSCs.
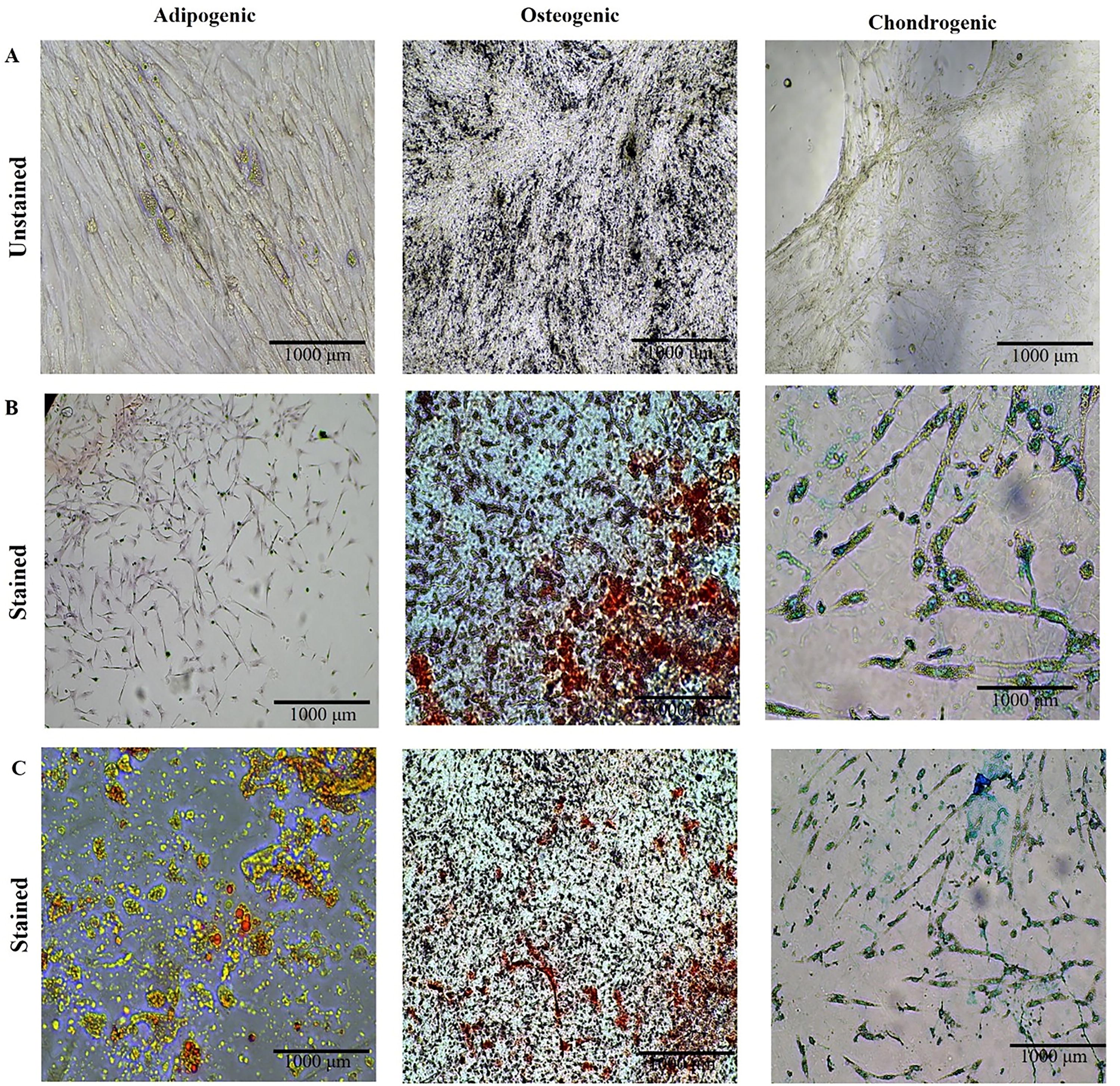
BM-MSC characteristic differentiation analysis as adipogenic, osteogenic, and chondrogenic.
The correlation between multiple factors such as gravida, parity, the postpartum day of BM collection, maternal age, gestational week of the baby, birth weight (in grams), and the count, viability, and marker expression of MSCs in both fresh and 72-hour refrigerated (+4°C) BM samples was evaluated using the Spearman correlation analysis test (Fig. 4, Table 6). An inverse correlation was found between the number and viability rate of fresh BM-MSCs and parity. This indicates that with an increase in parity, there is a decrease in the number of MSCs and their viability in fresh BM. The correlations for the other examined variables did not show statistical significance (p > 0.05) (Fig. 4).
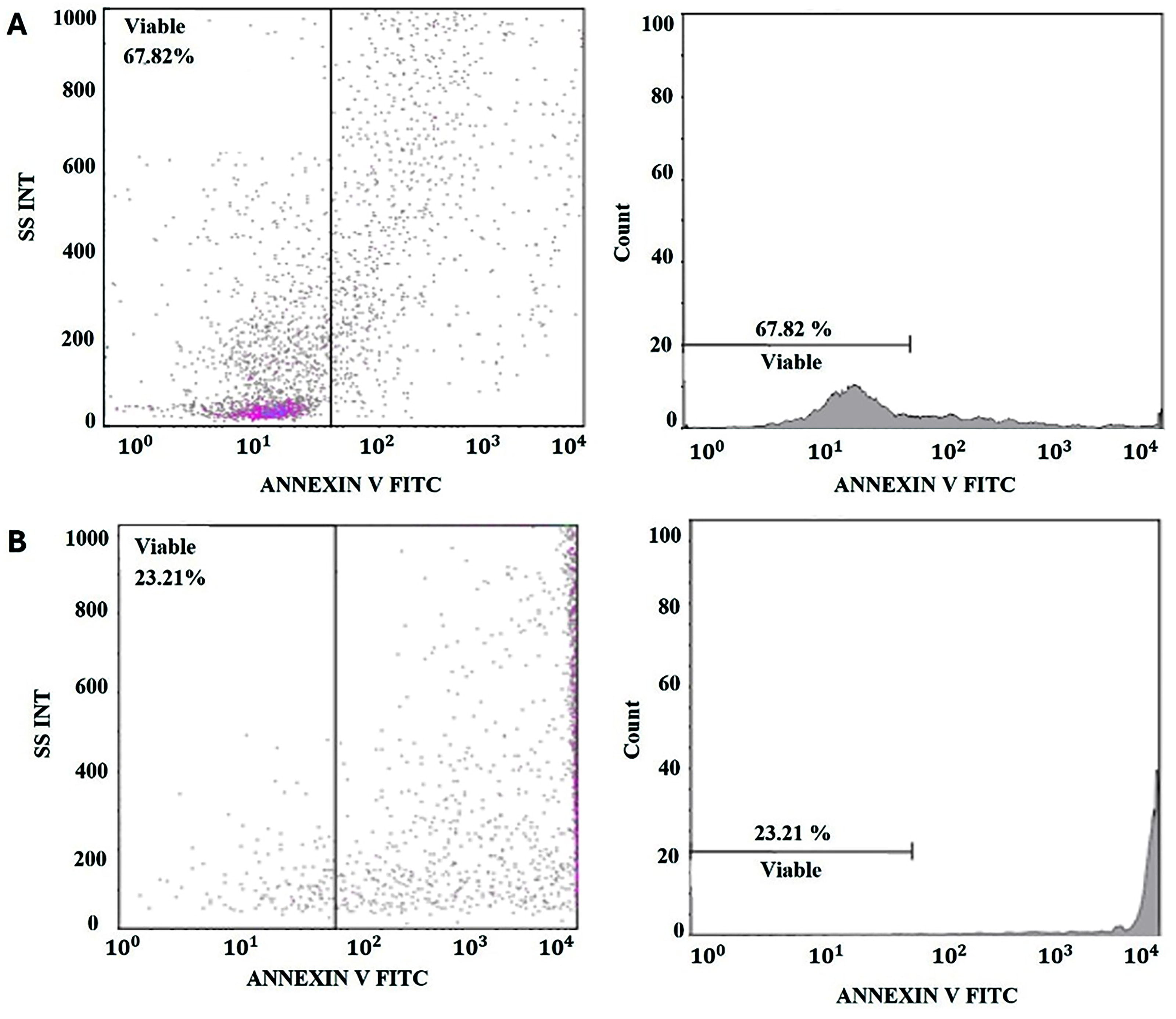
Comparative analysis of viability between fresh BM-derived MSCs using Annexin V staining and BM-MSCs which were stored for 72 hours at +4°C.
Spearman Correlation Test
BM, breast milk; MSC, mesenchymal stem cell.
Discussion
The Academy of Breastfeeding Medicine has set forth guidelines for storing expressed BM for up to 4 hours at room temperature (16–29°C), up to 4 days in a refrigerator (4○C), and as long as 6 months in a freezer (≤−4°C). 31 These guidelines primarily consider factors such as bacterial growth and the degradation of milk components, including immune cells, lipids, and antioxidants. However, they do not address how cold storage affects the viability of the milk’s microbiome. Storing human milk according to these recommended conditions has been shown to change the profile of viable bacteria, which may significantly affect the colonization of the infant’s gut and overall infant health.3,15 This aspect is crucial as the gut microbiota plays a significant role in NEC pathophysiology. Recent studies have also highlighted that daily probiotic supplementation in premature infants can decrease the risk of NEC. 15
Research has demonstrated that the level of antioxidants in BM decreases gradually throughout the first 14 days of storage, whether in the refrigerator or freezer. Significantly, on the 21st day, there is a notable decrease in antioxidant levels. 16 Refrigerating BM reduces the quantity and activity of macrophages and leukocytes, although lymphocytes, secretory IgA, cytokine, and growth factor levels remain unchanged. However, storing BM at −20°C in a deep freezer leads to a notable decrease in both the quantity and effectiveness of lactoferrin.32–34 Conversely, the concentrations of several cytokines and immunoglobulins in bone marrow have been seen to remain constant for a period of 3–6 months when subjected to freezing.35,36
A research study was conducted to examine the extended preservation of BM. Samples were stored at −20°C for 6 months. The primary objective was to observe the monthly fluctuations in macronutrient content. The results of this study revealed that although the protein and carbohydrate levels in BM were generally constant, there was a significant reduction in the fat content and the overall energy value of the milk. 35
Currently, MSCs derived from the umbilical cord are being utilized in the clinical treatment of neonatal disorders that have a high incidence of illness and death, such as BPD, IVH, and NEC. Encouraging outcomes have been achieved.1,3,26 Nevertheless, there is a lack of clinical research in the existing literature demonstrating the administration of BM-MSCs by the systemic route. Furthermore, there is a lack of research in the existing body of literature directly comparing BM-MSCs with MSCs derived from other sources. Conducting further research to compare the functional and regenerative abilities of BM-MSCs with MSCs derived from alternative sources could have significant ramifications for regenerative medicine. One considerable benefit of BM is that while BM-MSCs can develop into different cell types, they do not give rise to tumors or lead to teratoma production.5,37,38 The numerous and varied varieties of stem cells present in BM offer additional benefits due to their noninvasive nature and easy accessibility.6,18,21,22
In our study group, there was one small for gestational age (SGA) baby and one large for gestational age (LGA) baby. A total of 17 moms and babies participated in the study. One woman had a diagnostic of both gestational diabetes mellitus (GDM) and gestational hypertension (GHT), while two mothers had a diagnosis of GDM. The impact of the mother and baby’s demographic features on BM-MSCs remains a significant area of research. However, because to insufficient sample sizes of SGA, LGA, GDM, and GHT in our study, statistical analysis could not be conducted.
The stem cell characteristics of BM may be influenced by factors such as the lactation stage and the quantity of BM collected. The quantity and arrangement of cells in the BM differ according on the breastfeeding stage. Colostrum refers to the initial milk produced by the mother, which is characterized by having the highest concentration of immunological and cellular components during the breastfeeding phase. As BM develops, its quantity increases while its cellular composition diminishes. Nevertheless, it still retains stem cells and all other types of cells. The research did not provide specific information regarding the quantity of collected BM and the lactation stage. The time interval for collecting milk samples ranges significantly from day 1 to week 177.6,24
In addition, the amount of BM collected varies between 15 and 55 mL, and the average of BM-MSCs collected was 2–2.5 × 106 per mL. However, in our study, we showed that the average number was 0.8 × 105 per mL. Due to the high nutritional value of colostrum for infants, our study found that both the fresh and preserved samples yielded just 5 mL of collected milk. This discrepancy was attributed to the comparatively diminished quantity of BM obtained in our investigation, in contrast to the findings reported in existing literature.
Studies have not found a significant effect of maternal age, parity number, birth weight, or gender of the baby on the number of MSCs in BM and their immunological characteristics [18]. Unlike other studies, our study had a negative correlation between parity and the number and viability of MSCs in fresh BM. In our analysis with Spearman’s correlation test, we found that the rate of MSC viability in fresh BM decreased as parity increased, and we found a decrease in the number of MSCs in fresh BM as the parity number increased, but it was not significant (p > 0.05) (Table 6). In another study, as the parity number increased, a decrease in the protein content of BM and an increase in the lipid ratio were observed, and irregular and statistically insignificant changes were observed in the amount of secretory IgA. There are a limited number of studies in the literature on how parity affects BM content. More studies are needed to interpret this relationship correctly.
Existing research has primarily focused on how various storage conditions and physical factors impact BM components. Yet, no investigation has been conducted into how storage conditions influence the viability and immunological properties of stem cells within BM.
Our study aimed to explore the count, viability, and expression of positive surface markers of BM-MSCs under different storage scenarios. We isolated MSCs from fresh samples and samples stored at 4°C for 72 hours and at −20°C for 1 month. The results showed that while 80,000 MSCs were obtained from fresh BM, around 28,000 cells were isolated from those stored in the refrigerator for 72 hours. This represented a statistically significant reduction in the number and viability of MSCs in refrigerated samples compared with fresh ones. Notably, there was no significant alteration in the expression of positive MSC markers. Moreover, in samples stored at −20°C for a month, no viable MSCs were detected.
More comprehensive studies are needed to focus specifically on how storage conditions affect the live components in BM. Current research is insufficient to determine the optimal methods and duration for storing BM to preserve and utilize its cellular content to the greatest extent.
However, there is a lot of incomplete information about how the BM-MSCs are affected by infantile and maternal characteristics, at which lactation stage they should be collected, with which protocols to isolate, and how they are affected by physical storage conditions. 28
Conclusion
The study revealed that storing BM-MSCs in the refrigerator led to a decrease in their viability. However, the surface markers of the surviving cells were still intact. On the other hand, freezing BM resulted in the loss of its MSC content. Our study is significant since it is the inaugural investigation in the scientific literature to demonstrate the impact of storage conditions on BM-MSCs. The study demonstrates that fresh BM has a significantly higher quantity of MSCs compared with preserved milk. It is crucial to administer fresh BM for enteral feeding, buccal, and nasal applications, particularly for premature infants in neonatal intensive care units. This ensures that they receive the highest possible levels of immunological components and BM-MSCs. Ultimately, it is imperative that all newborns are nourished exclusively with unpreserved BM to the greatest extent feasible, and it is crucial to promote early initiation of breastfeeding for both the mother and the infant.
This study aimed to examine the influence of storage conditions on the viability and immunological characteristics of BM-MSCs in order to assess the preservation of the cellular component in BM.
Footnotes
Authors’ Contributions
E.Ç. conceptualized and designed the study, collected data, drafted the initial article, and critically reviewed and revised the article. D.D. contributed data and critically reviewed and revised the article. S.G.K. assisted with statistical analysis and critically reviewed and revised the article. E.N.B., E.Ö.G., M.G., R.K., T.A., S.S.K., and E.O. conceptualized and designed the study, collected data, and critically reviewed and revised the article.
Data Availability Statement
All data generated or analyzed during this study are included in this article and its supplementary materials. For further inquiries, please contact the corresponding author.
Statement of Ethics
This study protocol was reviewed and approved by the Human Research Ethics Committee of the University of Marmara (approval number 09.2018.723).
Disclosure Statement
The authors have no conflicts of interest to declare.
Funding Information
This study is supported by the Scientific Research Projects Association (Project Code: SAG-C-TUP-130219-0046). The funder had no role in this study’s design, data collection, analysis, or reporting.