
Abstract
Introduction:
Donor human milk (DHM) is the next best option when mothers’ milk is unavailable. The study objective was to examine mothers’ knowledge and attitudes regarding DHM.
Materials and Methods:
A prospective, descriptive, online study using mixed methods. Regression analysis was used to control for confounding variables and content analysis for the qualitative component.
Results:
Eighty mothers from the Palestinian Territories and Israel participated. Mothers’ mean objective knowledge score was 3.4/6, and self-evaluation knowledge score was 2.4/5, with religion significant for both scores (p < 0.001 and p = 0.002), respectively. Compared with Muslim mothers, Christian and Jewish mothers were more likely to prefer DHM to formula: (adjusted odds ratio [95% confidence interval], 4.9 [1.5–16.6], and 17.5 [4.3–71.4]), donate HM (human milk) to a friend or relative (7.8 [2.0–30.3]) and 60 [9.9–362.3]) or donate HM to a human milk bank (5.4 [1.3–23.3] and 11.2 [2.6–47.5]). Muslim and Christian mothers were more likely to state that DHM was permissible only under certain circumstances. Regression analysis revealed that only religion was significant for mothers’ response that DHM was permissible (p < 0.001). Qualitative analysis revealed that differences in mothers’ knowledge and attitudes were related to milk kinship.
Conclusions:
In this first study of mothers’ knowledge and attitudes of DHM in the Palestinian Territories and Israel, results revealed low knowledge and negative attitudes regarding DHM correlated with the mother’s culture. Future programs should include culturally competent initiatives regarding the benefits of DHM.
Introduction
Exclusive breastfeeding is recommended for all infants in the first 6 months of life as it provides optimal nutrition and protective effects to decrease morbidity and mortality, such as decreased rates of infections such as respiratory infections, severe diarrhea, otitis media, and childhood obesity. 1 If mother’s own milk (MOM) is unavailable, donor human milk (DHM) is the next best option. DHM can be obtained via informal milk sharing from a relative or friend or via formal milk sharing, where human milk is obtained from a human milk bank (HMB). 2 Although DHM is recognized as an evidence-based practice, the family’s culture influences decisions on DHM. 3
There are few HMBs in the Middle East. Due to religious considerations, the first HMB in Turkey was closed during the pilot stage. 4 Iran opened its first HMB in 2016 and is reported to have 11 HMBs.5,6 The Ministry of Health in Israel’s first official HMB began operations in 2020. 7 The Ministry of Health in the Palestinian Territories has not launched a HMB.
There is a dearth of research on mothers’ knowledge and attitudes regarding DHM, and it has not been investigated in Israel and the Palestinian Territories. The aim of the study was to examine mothers’ knowledge and attitudes regarding the use of DHM.
Materials and Methods
A prospective, descriptive study using mixed methods of qualitative and quantitative research, including snowball sampling, was conducted on mothers from July 2021 to September 2021. Inclusion criteria were Jewish and Arab mothers with access to social media, aged 18 years or older, who can read and write Arabic, English, or Hebrew. Exclusion criteria were women who are not parents to at least one child. Areas were defined as part of the Palestinian Territories or Israel by current jurisdiction. A power analysis was performed. Hebrew University’s Ethical Board approved the study (#03062021).
The Donor Breast Milk Questionnaire, which contained 42 questions, was used to examine mothers’ knowledge and attitudes toward DHM and collect demographic information. The questionnaire was adapted from two previous questionnaires for studies conducted on mothers in the United States and Israel by the primary researchers of the present study (A.N. and L.M.N.). Questions that evaluated mothers’ attitudes concerning DHM were adapted from a study in New York. The demographic questions were adapted from a study in Israel that evaluated breastfeeding of early-term infants. 8 The present questionnaire included objective knowledge questions, self-evaluation knowledge questions, attitude questions, and open questions on DHM. The questionnaire was translated from English into Hebrew and Arabic via the Brislin method with backward–forward translations for each language to the original English. 9 The researchers were given permission to use the Donor Breast Milk Questionnaire, including its adaptation with open and closed questions and translation for the present study. After the questionnaire was adapted for the present study, it received expert validity from a committee of physicians, nurse–midwives, nurses, and lactation consultants with expertise in Women’s Health, Neonatology, Research, and Lactation. For the present study, the Cronbach’s alphas in all three languages were 0.73 for the knowledge questions and 0.85 for the knowledge self-assessment questions.
Procedure
After receiving ethical approval, the questionnaire was posted on social media, which included Facebook, WhatsApp, Instagram, and Messenger, with a cover letter that contained an explanation of the study: the purpose of the study, eligibility for the study, and that participation in the study was voluntary and anonymous. The cover letter also stated, “Please feel free to forward the link for this study to family and friends that you think would be interested in participating in this survey.” For the social media sites, one of the researchers asked and received permission from the website’s coordinator to join mothers’ groups and to post the cover letter and link to the survey. The researcher’s names, titles, and affiliations were provided, and contact information for the researchers (A.N. and M.K.) was included. A link to the study site was provided. Participants who clicked on the link were directed to the study that contained the cover letter and questionnaire. Consent was implied by participation in the study. After the questionnaire was filled out, the data were saved in the researchers’ university’s secure system. No personal data were obtained, and there was no possibility of tracking computer information identity. A pilot study was performed on the data obtained from the first 10% of the participants in the study. No revisions were necessary; therefore, the study continued to collect data.
Data analysis
All data were transformed into an Excel file and analyzed with SPSS 29. Descriptive statistics, Chi-square, ANOVA, t test, and regression analyses were used. The researchers used content analysis for the qualitative data to identify phrases, words, ideas, and concepts. The text was coded to evaluate frequent expressions to develop categories and themes based on the authors’ consensus. Triangulation of the qualitative and quantitative data allowed convergence and corroboration of the data. The study’s trustworthiness was determined using semistructured open questions to ensure credibility.
Results
Eighty mothers participated in the study. The mothers’ mean age was 33.2 (standard deviation [SD] 8.2), and the mean number of children was 2.2 (SD 1.0). A majority of the mothers reported having an academic degree. Mothers living in the Palestinian Territories reported their religion to be Islam and Christian, and from Israel Islam, Christian, and Jewish. Demographic information can be found in Table 1.
Demographic Information (N = 80)
Knowledge
Mothers were asked what the better option for feeding the infant was when there was insufficient MOM. Forty-three (54%) mothers selected formula as the better option, and 36 (46%) responded DHM (Table 2). Thirty-one (39%) mothers had not heard about the availability of DHM, while 49 (61%) had. When asked if DHM has more benefits than disadvantages, 27 (34%) responded no or don’t know, while 53 (46%) said it had more advantages. Thirty-nine (49%) of mothers responded that DHM from a friend or relative transmits infection. For the question regarding whether DHM from a national milk bank is safe and trustworthy, 29 (36%) responded that it is safe and trustworthy, 17 (21%) responded “no,” and 34 (43%) responded “don’t know.” Sixty-one (76%) responded that DHM contains more nutrients than formula, with 6 (8%) and 13 (16%) responding “no” and didn’t know, respectively. Twenty-nine (36%) thought HMB donation to a national milk bank was safe and trustworthy, 16 (20%) did not, and 35 (44%) did not know. Thirty-nine (49%) thought that HM donated from a relative or friend may transfer infection to their baby, 19 (24%) did not, and 22 (28%) did not know. Fifty-five (69%) thought that DHM provides some benefit regarding immunity/resistance to infections, 3 (4%) did not, and 22 (28%) did not know. Sixteen thought DHM may increase the risk of infants having an allergy; 31 (39%) did not, and 33 (41%) did not know. Fifty-three (66%) responded that DHM has more benefits than advantages, 4 (5%) did not, and 23 (29%) did not know.
Mother’s Knowledge of DHM
DHM, donor human milk; HM, human milk; HMB, human milk bank; MOM, mother’s own milk.
DHM objective knowledge scores were assessed from 1 (lowest possible) to 6 (highest possible). The median objective knowledge score was 3.4 (SD 1.2). Correlations were sought for demographic information and objective knowledge and are found in Table 3. No difference in knowledge was found for educational level (3.4 [SD 1.2], p = 0.379). There was a difference in religion. The mean knowledge score was 2.6 (SD 0.92) for mothers who were Muslim, 3.1 (SD 1.1) for Christian, and 4.2 (SD 1.1) for Jewish mothers (F[2,72] = 15.406, p = 0.000). For religiosity, there was only a difference between those mothers who reported to be Religious Traditional (2.6 [SD 1.06]) and Secular/Nonreligious (4.3[SD = 1.00]) (F[5,70] = 5.203, p = 0.000). Knowledge scores by marital status were 3.3 (SD 1.3) for married and 4.8 (SD 0.5) for single (p = 0.015). There was no difference in knowledge for income (p = 0.407). There was a difference in knowledge scores between those mothers who were health care professionals and those who were not. For health care professionals, the mean score was 3.9 (SD 1.4), and for nonhealth professionals, 3.2 (SD 1.1, p = 0.002). Regression analysis revealed that only religion significantly affected objective knowledge scores (p < 0.001) (Table 4).
Unadjusted DHM Objective Knowledge Scores and Demographic Information
Not significant: age, academic degree, income, religiosity, breastfed as an infant, breastfed an infant, duration breastfeeding youngest child, had infant admitted to NICU.
t test analysis.
DHM, donor human milk.
Adjusted a DHM Objective and Self-Evaluation Knowledge Scores and Demographic Information
Logistic regression analysis.
DHM, donor human milk.
Mothers were also asked to self-evaluate their knowledge of DHM. Using a Likert scale, self-evaluation scores ranged from a minimum of 1 (not knowledgeable) to a maximum of 5 (very knowledgeable). The mean self-evaluation knowledge score was 2.4 (SD 1.3). Correlations were sought for demographic information and self-evaluation knowledge and are found in Table 5. There was no difference in level of education (2.4 [SD 1.2]), p = 0.170. There was a difference for mothers’ religion: Islam (2.2 [SD 1.0]), Christian (2.0 [SD 1.2]), and Jewish (3.1 [SD 1.3]), p = 0.001. Post hoc tests for mothers rating their knowledge found a difference between Jewish and Christian mothers (p = 0.002) and Jewish and Muslim mothers (p = 0.021). There was no difference in the level of religiosity with a mean score of 2.44 (F[5,70] = 1.904, p = 0.105). There was no difference in income with a mean score of 2.44 (F[2,73]=0.806, p = 0.451). Health care professionals rated their knowledge higher with a mean score of 3.16 (SD = 1.89) than nonhealth care professionals 2.17 (SD = 1.12), p = 0.002. Regression analysis revealed that religion (p = 0.002) and health care professional (p = 0.016) significantly affected self-evaluation knowledge scores (Table 4).
Unadjusted DHM Self-Evaluation Knowledge Scores and Demographic Information
Not significant: age, marriage, academic degree, income, level of religiosity, breastfed as an infant, breastfed an infant, duration breastfeeding youngest child, had infant admitted to NICU.
t test analysis.
DHM, donor human milk; SD, standard deviation.
Attitudes
DHM attitudes were evaluated by asking about using or donating DHM. Mothers were asked what source of DHM they would select to use: 26 (33%) would choose a relative/friend, 23 (29%) an HMB, and 7 (9%) milk from an internet source. Mothers were asked what option they would choose if MOM were not available. Forty (50%) responded that they would select formula. There was no difference in whether mothers had an infant admitted to the NICU (p = 0.66). Mothers were asked about their attitudes regarding donating and receiving DHM. When asked if they would donate their MOM to an HMB, 30 (38%) would, 26 (33%) would not, and 22 (28%) were not sure if they would. Forty-four (56%) would donate to a friend or relative, 14 (18%) would not, and 20 (25%) were not sure if they would. Mothers were asked if they had any relatives or friends who donated their MOM; 55 (70%) did not, and 25 (30%) did. Forty-eight (60%) of mothers stated that HM from another person (other than the mother) was permissible, 4 (5%) that it was not permissible, and 28 (35%) that it was permissible only under certain circumstances.
Mother’s religion was correlated with attitudes toward DHM use. Compared with Muslim mothers, Christian and Jewish mothers (adjusted odds ratio [95%confidence interval]) were more likely to prefer DHM to formula: (4.9 [1.5–16.6] and 17.5 [4.3–71.4]), donate HM to a friend or relative (7.8 [2.0–30.3] and 60 [9.9–362.3]), or donate HM to an HMB (5.4 [1.3–23.3]) and 11.2 [2.6–47.5]), respectively. Mother’s religion and HMB safety and trustworthiness were also correlated and found that 11 (46%) Muslim mothers, 4 (17%) Christian mothers, and no Jewish mothers responded that HMBs were not safe or trustworthy (p < 0.001). In addition, 30% of Jewish, 46% of Muslim, and 54% of Christian mothers responded that they didn’t know whether HMBs were safe and trustworthy.
Mothers who were Muslim (79%) or Christian (21%) were more likely to respond that DHM was permissible only under certain circumstances than Jewish mothers (4%) (p < 0.001; Fig. 1). The question was further analyzed to determine the difference in their level of religiosity. Those who reported being Secular/Nonreligious were more likely to respond (94%) that DHM was permissible, 14% of Religious Traditional that it was not permissible, and 6 (6.7%) of those who reported being Very Religious responded that it was only permissible under certain conditions (p = 0.026). Regression analysis revealed that only religion, but not the level of religiosity, significantly affected whether mothers responded that DHM was permissible (p < 0.001).
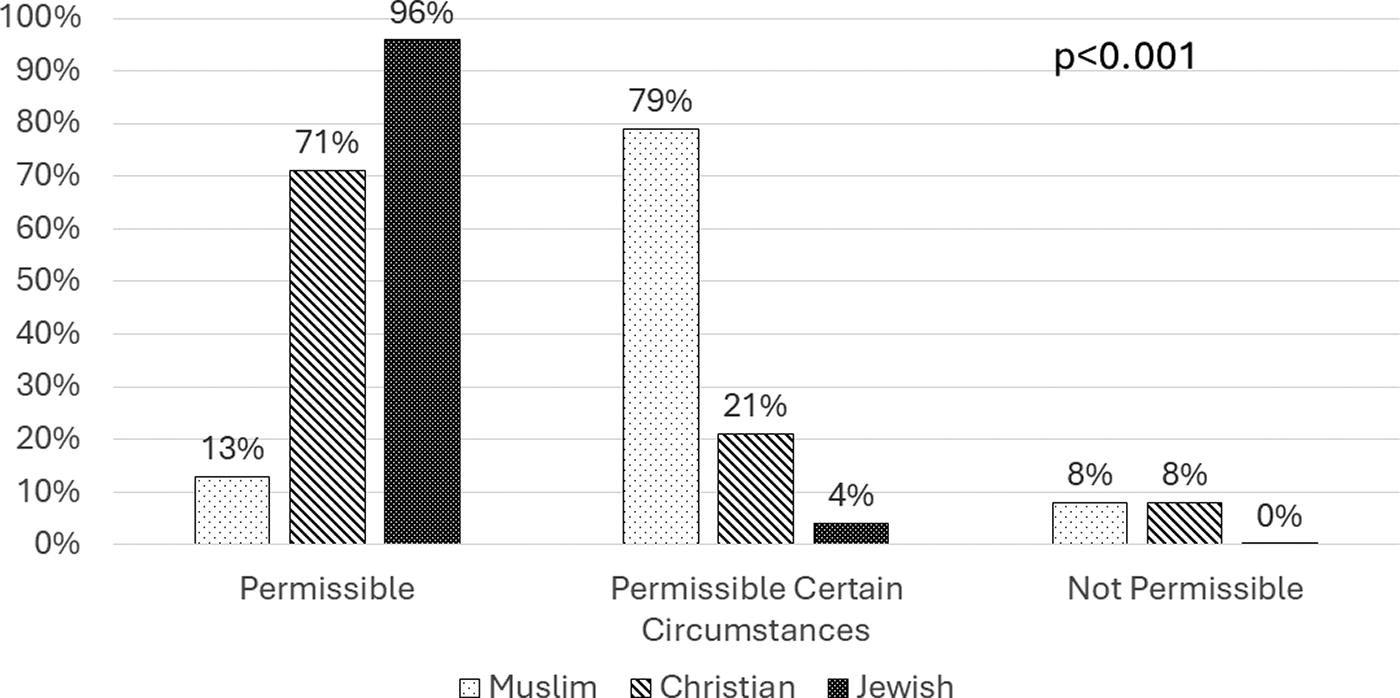
Permissibility of donor milk by maternal religion.
Qualitative analysis
Open questions revealed an added perspective on why mothers prefer DHM or formula. Categories included: giving DHM will create a milk kinship, it is better to receive milk from a friend or relative than a HMB, and that formula is available, affordable, nutritious, and safe. Categories for those preferring DHM were closest to MOM, nutritious, healthier option, prevents infection, and natural. The themes were milk kinship, formula is the best second choice if MOM’s milk is unavailable, and for those who would use DHM, it is the second best choice after MOM. Themes, categories, and selected mothers' comments are found in Table 6.
Themes, Categories, and Selected Mothers’ Comments
Discussion
To our knowledge, the present study was the first to examine knowledge and attitudes toward DHM among mothers in the Palestinian Territories and Israel. The questionnaire was available in English, Arabic, and Hebrew and was conducted via social media, giving access to different populations. The study utilized mixed qualitative and quantitative research methods that allowed a deeper understanding of cultural differences. Mothers who participated in the study were Muslim, Jewish, and Christian. The present study evaluated mothers’ knowledge regarding DHM, both formal (from a HMB) and informal milk sharing (from a relative or friend), and the process of collecting and storing DHM.
Mothers’ knowledge of DHM was low, and their attitudes were negative about using DHM. Most of the mothers heard about the availability of DHM. However, more than half preferred formula over DHM as a first option. This is similar to findings from previous studies, such as Elmsworth et al., that examined mothers’ experiences, knowledge, and attitudes toward using DHM and donating their human milk, with an overwhelming majority (89%) preferring to give their infants formula rather than DHM and only if left with DHM as the only option would choose a relative/friend as the donor rather than a HMB. 10 Pal et al. (2020) examined a multicultural population of mothers in New York City and found that more than half preferred formula over DHM. 11 This may have been related to the mother’s low knowledge of DHM. Mothers in that study whose infants had been hospitalized in the NICU were more amenable to using DHM from a HMB than a relative/friend.
In the present study, the adjusted analysis revealed that mothers who were health care professionals had higher self-evaluation knowledge scores, but not objective knowledge scores, than other mothers (Table 4). It suggests that health care professionals may think that they know more than they do. This has implications as they are the ones that patients and families, neighbors, and friends seek for health information, emphasizing the need to provide health care professionals with evidence-based information.
The present study, however, did not find a correlation between mothers whose infants were admitted into the NICU, but rather that mothers’ religion was the significant factor concerning knowledge and attitudes toward DHM. Mean objective and self-evaluation knowledge scores were lower for mothers who were Muslim than for Christian and Jewish mothers on both the unadjusted and adjusted analyses. Compared with mothers who were Muslim, Christian and Jewish mothers were more likely to prefer DHM to formula, donate HM to a friend or relative, or donate HM to a HMB. Muslim mothers were more likely to state that DHM was permissible only under certain circumstances than Christian and Jewish mothers. Regression analysis revealed that only religion was significant for whether mothers responded that DHM was permissible (p < 0.001). Of note, multiple factors, including education, socioeconomic status, or language, were not significant. There was no difference between mothers who were Arab living in the Palestinian Territories or Israel.
The mixed methods design of the study allowed the researchers to gain a more in-depth understanding that mothers’ knowledge and attitudes were due to milk kinship, which was found in the quantitative and qualitative analyses. The source for milk kinship is from a passage in the Quran (Surah An-Nisa 4:23) that notes people who are forbidden to marry each other (mahram), such as brothers and sisters and fathers and daughters. 12 In the passage, “milk mothers” and “milk sisters” are forbidden in marriage and refer to those infants that suckled at the breast of a woman who is not the biological mother due to the establishment of a “milk kinship.”
Milk kinship originates from a quote in the Quran. Therefore, its origin is as a religious practice. However, our study demonstrated that milk kinship is a significant concern when deciding on the permissibility of DHM for Muslim mothers, regardless of their level of religiosity, education, or whether they live in a predominantly non-Muslim country. There was no difference for the level of religiosity or for Arab mothers residing in Israel or the Palestinian Territories. Additionally, the study found that 21% of Christian mothers responded that DHM was only permissible under certain circumstances. We suggest that milk kinship may also be a cultural practice for those among, near, or immigrated from a Muslim-populated area due to acculturation.
For many years, no HMB was opened or sanctioned in Muslim countries due to concerns about milk kinship. In 2016, Iran opened the first HMB; since then, 11 HMBs have been established and sanctioned.5,6 A study of knowledge and attitudes of DHM of Iranian mothers revealed low knowledge but positive attitudes about the use of DHM. 13 A study in Turkey found that both native and non-native Turkish women were hesitant to use DHM due to religious concerns. 14 These concerns were a factor in Turkey ending its pilot program. 4
Using Islamic principles that MOM is beneficial, UNICEF has promoted the use of MOM in the Palestinian Territories; however, a HMB has yet to be established. 15 In Malaysia, due to the concerns of premature infants not receiving HM, Malaysia officially opened the first Sharia-compliant Milk Bank Model in 2022.16,17 Being Sharia-compliant includes consent to establish a milk kinship by the husband and wife donating and receiving.
In Israel, the HMB is relatively new, as it began providing DHM to hospitals in 2020. 7 In 2022, the Israel Human Milk Bank conducted a professional conference that included a session with religious leaders discussing the religious ramifications of allowing premature infants to receive DHM in light of its potential to save lives. 18 Religious leaders related the Jewish, Muslim, Greek Catholic Church, and Druze permissibility of using DHM. However, the President of the Supreme Sharia Court of Appeals in Israel discussed the dilemma of using DHM due to the issue of creating a milk kinship.
Health care professionals should advocate for the use of DHM when MOM is not available while understanding the religious basis for the reluctance toward DHM among Muslim families. Health care professionals should engage Muslim families in shared decision-making when assisting them with infant feeding decisions. 19
Limitations
This study utilized snowball sampling and an online survey made available to mothers via social media. Snowball sampling is a technique where existing study participants recruit others, such as their relatives, friends, and acquaintances. The benefit of snowball sampling is that it allows researchers to access a sample that is difficult to reach. However, using social media for snowball sampling may introduce sampling bias toward those who are active online and potentially make it difficult to generalize to the general population. Therefore, mothers who had no access to social media were not able to participate. The study used a convenience sample for one group. Another limitation was that most mothers were highly educated and had an academic degree; therefore, generalizability may only apply to some populations.
Conclusions
To our knowledge, this study was the first to examine Israeli and Palestinian mothers’ knowledge and attitudes regarding DHM. The results revealed low knowledge and negative attitudes regarding DHM and HMBs. Knowledge and attitudes were correlated with the mother’s religion and culture. The study revealed that milk kinship is a significant concern when deciding on the permissibility of DHM for Muslim mothers, regardless of their level of religiosity, education, or whether they live in a predominantly non-Muslim country. In addition, the study suggests that Christian mothers who live among, near, or immigrated from a Muslim-populated area may also have concerns when deciding on DHM as a cultural practice.
Health care professionals should engage families concerned about DHM due to religious and/or cultural practices in shared decision-making when assisting them with infant feeding decisions. Future programs should include culturally competent initiatives regarding the benefits of DHM.
Footnotes
Acknowledgment
The authors thank Mrs. Shada Macol RN, MA and Mrs. Nadia Korabe RN, MA, LC for their assistance with this study.
Authors’ Contributions
Conceptualization: A.N. and L.M.N.; Methodology: A.N. and L.M.N.; Software: A.N. and M.K.K.; Validation: A.N., L.M.N., M.K.K., and S.E.F.; Formal analysis: A.N., L.M.N., and M.K.K.; Investigation: A.N. and M.K.K.; Resources: A.N, L.M.N., M.K.K., and S.E.F.; Data curation: A.N., L.M.N., and M.K.K.; Writing—original draft preparation: A.N., M.K.K., and L.M.N.; Writing—review and editing: A.N. and L.M.N.; Visualization: A.N. and L.M.N.; Supervision: A.N. and L.M.N.; Project administration: A.N. All the authors have participated in the concept and design, analysis, and interpretation of data, and in the drafting or revising of the article. All authors have read and agreed to the published version of the article.
Disclosure Statement
The authors have nothing to disclose.
Funding Information
There was no funding for this study.