
Abstract
Background:
During emergencies, including natural disasters and armed conflict, breastfeeding is critically important. Breastfeeding provides reliable nutrition and protection against infectious diseases, without the need for clean water, feeding implements, electricity, or external supplies.
Key Information:
Protection, promotion, and support of breastfeeding should be an integral part of all emergency preparedness plans. Breastfeeding specialists should be part of plan development. Emergency protocols should include breastfeeding specialists among emergency relief personnel, provide culturally sensitive environments for breastfeeding, and prioritize caregivers of infants in food/water distribution. Emergency relief personnel should be aware that dehydration and missed feedings can impact milk production, but stress alone does not. Emergency support should focus on keeping mothers and infants together and providing private and/or protected spaces for mothers to breastfeed or express milk. Emergency support should also focus on rapidly identifying mothers with breastfeeding difficulties and breastfeeding mothers and infants who are separated, so their needs can be prioritized. Breastfeeding support should be available to all women experiencing difficulties, including those needing reassurance. Nonbreastfed infants should be identified as a priority group requiring support. Relactation, wet-nursing, and donor milk should be considered for nonbreastfed infants. No donations of commercial milk formula (CMF), feeding bottles or teats, or breast pumps should be accepted in emergencies. The distribution of CMF must be highly controlled, provided only when infants cannot be breastfed and accompanied by a comprehensive package of support.
Recommendations:
Protecting, promoting, and supporting breastfeeding should be included in all emergency preparedness planning and in training of personnel.
About ABM Position Statements:
The Academy of Breastfeeding Medicine empowers health professionals to provide safe, inclusive, patient-centered, and evidence-based care. Women and others who are pregnant and lactating identify with a broad spectrum of genders, pronouns, and terms for feeding and parenting. There are two reasons ABM’s use of gender-inclusive language may be transitional or inconsistent across protocols and position statements. First, gender-inclusive language is nuanced and evolving across languages, cultures, and countries. Second, foundational research has not adequately described the experiences of gender-diverse individuals. Therefore, ABM advocates for, and will strive to use, language that is as inclusive and accurate as possible within this framework.
For more explanation, please read ABM Position Statements on Infant Feeding and Lactation-Related Language and Gender and Breastfeeding As a Basic Human Right.
Introduction
During emergencies, such as natural disasters, armed conflicts, famines, and mass displacement, breastfeeding is vital to the health and well-being of infants and their mothers. Breastfeeding saves lives, 1 and this is particularly true in emergency settings. Breastfeeding provides a clean, reliable source of safe nutrition without the need for clean water, feeding implements, electricity, or other external supplies. Breastfeeding helps to prevent infections and malnutrition, both of which can be a significant risk in emergency situations. 2 In addition, breastfeeding reduces the maternal stress response, 3 partly through the release of the hormone oxytocin, 4 which helps increase maternal resilience in the face of traumatic circumstances.5,6 A reduced stress response helps mothers provide sensitive, loving care to their infants, thereby protecting the mental health and development of children. 7 Breastfeeding (even the odor of breast milk 8 ) is known to decrease infants’ stress and pain responses, 9 which is helpful during a crisis. Breastfeeding also protects maternal health during emergencies related to birth spacing and preventing excessive postpartum hemorrhage. 10
In contrast, the emergency milieu increases the risks associated with feeding of commercial milk formula (CMF). Feeding implements (including cups, bottles, and teats) require washing with hot water and detergent and powdered infant formula requires boiled water for reconstitution. These resources are often scarce in emergencies. Infants who are dependent on CMF are vulnerable to food insecurity due to supply chain disruptions that commonly occur in emergencies. They are also deprived of the many ingredients in breast milk that protect against infection, whereas infant formula itself affects the gastrointestinal environment in a way that facilitates infection. 11
Severe weather and natural disasters are becoming increasingly common with climate change. 12 Children are disproportionately impacted by climate change. 13 In addition, in 2022, more than two-thirds of the world’s children were living in countries experiencing conflict, and 1 in 6 children were living less than 50 km from where fighting was taking place. 14 In light of the contribution of breastfeeding to infant health, well-being, and survival, as well as to maternal health, health care professionals as well as emergency relief personnel should act to support breastfeeding mothers in emergency situations and ensure appropriate targeted support for nonbreastfed infants and their caregivers.
The ABM Position Statements Breastfeeding as a Basic Human Right 15 and Informal Breast Milk Sharing for the Term Healthy Infant, 16 and the ABM Protocol #35 Supporting Breastfeeding During Maternal or Child Hospitalization, 17 serve as important adjuncts to this Position Statement. In addition, all ABM protocols that help promote breastfeeding, such as #37 Physiological Infant Care, 18 #2 Guidelines for Birth Hospitalization Discharge, 19 and #14 Breastfeeding Friendly Physician’s Office 20 also serve as important resources.
Recommendations
The Academy of Breastfeeding Medicine makes the following recommendations, based not only on international guidelines but also on our synthesis of available information and on expert opinion.
Protection, promotion, and support of breastfeeding should be enabled at all times
The more women who are breastfeeding before the disaster, the more breastfeeding women there will be able to continue at times of emergency. At an individual level, breastfeeding should be promoted as an emergency preparedness action and women should be encouraged to factor emergencies into their infant feeding decisions. Exclusive expressing of breast milk without a medical reason should be discouraged. Women who exclusively use breast pumps should be referred for help to transition to direct breastfeeding and should know how to hand express. Governments should be encouraged to consider high breastfeeding rates as supporting community resilience to emergencies and view investment in breastfeeding support as emergency preparedness. As a part of this, implementation of the Baby-Friendly Hospital Initiative (BFHI) should be supported.
Emergency plans should include skilled breastfeeding support and breastfeeding specialists
Trained personnel should be available to support and assist breastfeeding mothers with issues that arise as a result of the emergency, including those related to ordinary breastfeeding concerns, issues requiring reassurance, low milk production, relactation, facilitation of wet nursing, assistance of mothers who are separated from their infants, and assistance for those who are exclusively expressing breast milk. Breastfeeding specialists should be trained on how to counsel and assist breastfeeding mothers who request CMF.
Ensure training of emergency relief personnel so that they are able to support breastfeeding dyads within their role
Emergency relief workers should receive basic training and sensitization on the support needs of breastfeeding women in emergencies and on Infant and Young Child Feeding in Emergencies (IYCF-E) policies and procedures. Educational messages should include breastfeeding is the safest and most reliable source of infant nutrition during an emergency. Training should include content on the harm of providing CMF to breastfeeding mothers and where to refer breastfeeding mothers or other caregivers who request formula.
In cases of mother–infant separation, wet-nursing (breastfeeding from another mother) or use of donor milk should be considered
Health screening of wet nurses and milk donors should be informed by available resources (e.g., testing for infectious diseases) and local prevalence of infections of concern. Breast milk donation should be done through local milk banks. Milk banks should be included in emergency planning and have their own emergency plans. Local informal milk sharing may be necessary if use of banked milk is not available.
In cases of mother–infant separation, assure maternal milk production
Mothers who are separated from their infants should be encouraged and supported to hand express their milk. Breast pumps should only be considered for use if abundant hot water for washing is available. Separated mothers may be willing to wet-nurse infants in need of breast milk.
Emergency plans should include provisions that support breastfeeding in shelters and mother–baby areas
Planning should include breastfeeding support in emergency shelters. Emergency shelter protocols should enable staff to rapidly identify the feeding needs of each family with infants and young children, as well as breastfeeding mothers and infants who are separated.
Women should be able to access breastfeeding support on-site or facilitated to access support off-site, including via electronic communication or telephone. Breastfeeding mothers and the other caregivers of infants and young children should receive priority in queuing for food and water distribution. Emergency shelters should include a protected space for mothers to breastfeed their children or express their milk with the amount of privacy the mother requires according to local cultural practice.
Mother–baby areas (MBAs) to facilitate maternal psychological well-being, breastfeeding, and other health support should be set up during emergencies and in their aftermath.
Infants not directly breastfed should be fed using a cup if there is no reliable source of clean water
Use of bottles and teats for feeding infants should be strongly discouraged in circumstances where adequate washing with hot water is not possible. In these situations, cup feeding, including with disposable cups, should be supported. Similarly, use of breast pumps should also be strongly discouraged where adequate washing with hot water is not possible, and instead hand expression should be supported.
Nonbreastfed infants should be considered a vulnerable group and appropriately supported, with use of breastfeeding or donor milk as initial options
CMF should only be provided after an assessment of need by appropriately trained health providers. Breast milk options for feeding nonbreastfed infants should be explored first as follows: relactation, wet-nursing, and donor milk (in that order) and if these are not available, CMF. If a decision is made to provide commercial milk to an infant, it must be accompanied by guidance on safe preparation under the emergency conditions and caregivers must be ensured access to other resources needed to feed with an adequate level of safety. These resources include the following: clean water for reconstitution and washing, an ability to heat water for reconstitution and washing, and adequate feeding implements as well as health monitoring and health care, with a commitment to provide this support for as long as the infant needs it.
The international code for the marketing of breastfeeding substitutes should be followed, and guidance on donations and distribution from the Infant and Young Child Feeding in Emergencies-Operational Guidance should be followed
Donations of CMF, other breast milk substitutes, bottles and teats, commercial complementary foods, and breast pumps should not be sought or accepted, but rather should be publicly discouraged. CMF distribution must be strictly controlled by emergency relief personnel, provided only when an infant cannot be breastfed, and should not be routinely distributed. CMF should not be distributed to exclusively breastfeeding mothers. CMF should be stored and distributed discreetly so as not to discourage breastfeeding mothers. Advertising and sponsorship related to CMF and other breast milk substitutes, bottles and teats, and breast pumps should not be permitted in emergency shelters or in any other aspect of emergency response (e.g., on or inside care packages).
Feeding complementary foods or liquids to infants younger than 6 months should be discouraged and infants younger than 6 months should not be provided with solid food
Complementary feeding of infants 6–23 months should be supported in emergency response. Any complementary foods that are provided should be safe and appropriate, and donations of commercial complementary foods should not be solicited or accepted.
Key Information to Support Recommendations
Background
Natural and human-origin disasters can cause destruction and widespread disruption, including to breastfeeding mothers and their breastfed children and to nonbreastfed infants and their mothers and caregivers, leading to the need for an emergency response.
The Global Strategy for Infant and Young Children Feeding from the World Health Organization and UNICEF recommends exclusive breastfeeding for the first 6 months of life, after which appropriate complementary foods should be introduced with breastfeeding continuing alongside for up to 2 years or beyond. 21 Infants younger than 6 months should not be fed liquids other than breast milk or CMF, including teas, juices, or homemade formulas.21,22
The main internationally recognized core guidance resource for infant and young child feeding is the Infant and Young Child Feeding: Operational Guidance for Program Managers (OG-IFE), which provides detailed guidance on emergency response to meet the feeding needs of infants and young children. 23 In 2010, the World Health Assembly urged all member states to ensure that they had national emergency preparedness plans in line with the OG-IFE. 24 A second influential resource is The Sphere Handbook: Humanitarian Charter and Minimum Standards in Disaster Response (Sphere Handbook), which provides direction on aid provision across the breadth of human needs in disasters. 25 The Sphere Handbook adapts and reflects the OG-IFE, and provides minimum humanitarian standards. The recommendations made in this Position Statement are informed by the OG-IFE and therefore are also aligned with the Sphere Handbook. Additional resources to support IYCF-E response can be found in Table 1. This Position Statement also draws from many resources and presents a compilation and synthesis of information that will be useful for those preparing for emergencies or working in an emergency situation.
Online Resources for Infant and Young Child Feeding in Emergencies
Care should be taken to ensure that resources are suitable for the setting in which they will be used.
CMF, commercial milk formula; IFE, infant feeding in emergencies: OG-IFE, Infant and Young Child Feeding in Emergencies-Operational Guidance; IYCF-E, Infant and Young Child Feeding in Emergencies.
Personnel who provide support during an emergency to breastfeeding mothers and other caregivers of infants and young children may include government employees, nongovernmental organizational staff, volunteers, and health care providers. In this document, we refer to them broadly as emergency relief personnel or aid workers.
Population feeding practices and beliefs
Population infant and young child feeding practices before the emergency greatly impact the required emergency response. 23 Populations with a strong breastfeeding culture, high rates of early, exclusive, and continued breastfeeding, and robust community and health system support of breastfeeding will be more resilient in emergencies. In such circumstances, emergency response will be able to focus almost entirely on supporting women to breastfeed with only small numbers of nonbreastfed infants requiring assistance. However, many low- and middle-income countries (LMICs) have high rates of any breastfeeding but may also have high rates of prelacteal feeding and mixed feeding, with breastfed infants also being fed with animal milk, cereals, or CMF. The IYCF-E response in these circumstances is more complex and challenging, with a need to support women not just to continue breastfeeding but to cease mixed feeding and exclusively breastfeed if possible.
In addition, in some high-income countries, a significant proportion of infants may be not breastfed (fully dependent on CMF). An IYCF-E response in communities with a large proportion of infants who are not breastfeeding at all is extremely challenging because of the vulnerability of these infants and the resources required to support their feeding needs. Finally, some countries have mothers who do not directly breastfeed their infants but instead exclusively express their milk with breast pumps and bottle feed their infants. As discussed later, these mothers and infants have particular support needs.
Different countries and communities not only have different feeding practices but broader differences in customs, religious beliefs, and in resources that impact health care availability, infant feeding, and infant mortality in general. They also have differences in emergency planning, emergency response practices, and capacities, including the involvement or not of humanitarian actors. All of these factors should be taken into consideration in supporting infant and young child feeding in emergencies and in applying the recommendations made in this Position Statement.
Breastfeeding in the Context of IYCF-E
Supporting breastfeeding in emergencies
Even though emergencies enhance the importance of breastfeeding, challenges associated with emergency conditions can make it difficult for women to breastfeed. The OG-IFE and Sphere Handbook both emphasize the need for breastfeeding women to receive skilled breastfeeding counseling in emergencies.23,25 Depending on the country and its resources, this support can include a variety of personnel, including nutritionists, medical doctors, International Board-Certified Lactation Consultants, persons with certifications in breastfeeding counseling or education, and volunteer breastfeeding counselors such as La Leche League Leaders. The Emergency Nutrition Network and the IFE Core Group has also published Operational Guidance: Breastfeeding Counseling in Emergencies to assist in the planning and implementation of breastfeeding counseling in emergencies. 26
One of the most common problems those supporting breastfeeding in emergencies will encounter is women who believe that stress has reduced their milk production. This concern is consistently reported irrespective of country or emergency type and can have the result of women introducing other foods and liquids or stopping breastfeeding. During conflict in Ukraine in 2015, stress was the most common reason given by women for ceasing breastfeeding and almost half of mothers who stopped breastfeeding their infants younger than 6 months named the stress of the conflict as the reason. 27 Health workers may also believe that stress adversely impacts breastfeeding as was found among those providing nutritional support to malnourished infants in an internally displaced persons camp in northern Nigeria, 28 thus compromising their ability to assist. Very often women who believe that stress has reduced their milk production base this belief upon observed infant behavior changes such as wanting to feed more frequently, being unsettled during feeds, and waking more often overnight. However, these behavior changes are normal in the context of the disruption of an emergency. 29 Stress results in decreased frequency of pulsatile releases of the hormone oxytocin, thus slowing the release of milk (letdown), which means feeds may take longer. 30 This effect on oxytocin does not affect the overall milk production in the short term, but over the longer term, chronic impairment of letdown might conceivably result in less effective milk removal, thus potentially impairing production. 31 Changes in letdown can contribute to infant fussiness. Stress may also cause women to be less responsive to infant hunger cues, 32 and thus feed them less frequently, which will also result in decreased milk production. In general, issues with actual or perceived decreased milk production are more likely to be the result of decreased feeding frequency and dehydration than directly as a result of stress itself. It is also common for women to believe that lack of food or not having access to particular foods will impact the quantity or quality of their milk. 33 Breastfeeding counseling and psychological and other supports can assist women who lack confidence in their ability to breastfeed to continue to breastfeed. 34
A variety of cultural beliefs can impact breastfeeding practices. Mothers may need to be reassured regarding a belief that negative emotions may impact the quality of their milk, 35 or that supernatural forces affect their breast milk. 36 Women may also have concerns that breastfeeding is dangerous due to experiences, such as being ill with diarrhea or other foodborne illness, 37 or because they are stressed or traumatized. 33 In the vast majority of circumstances, with information and reassurance, women are able to continue breastfeeding.17,38
Dehydration, reduced feeding frequency (due to constant movement, busyness, exhaustion, or lack of privacy), 39 or ordinary breastfeeding problems such as poor positioning and latch 28 may diminish milk production. Mothers can be reassured that milk production can be quickly increased with proper hydration, increased feeding frequency, and improved positioning and attachment. As discussed later, practical supports should be implemented to address the underlying reasons for dehydration or infrequent feeding and to otherwise support breastfeeding women. Mothers who are not exclusively breastfeeding their infants younger than 6 months should be sensitively encouraged to transition their infants to full breastfeeding.23,25 Supplementary feeding until exclusive breastfeeding is achieved is discussed later. Women may also experience breastfeeding difficulties such as mastitis, hyperlactation, or nipple pain and injury and require assistance.
In some cases, health care workers and other aid workers have provided breastfeeding women with poor information, advice, or support such as telling them to stop breastfeeding if they have a minor illness, if their infant cries, and in some cases, they simply encouraged mothers to give their infant CMF. 39 Some women, weakened by the stress of the emergency, have felt coerced into giving CMF, even by medical staff. 40 This underlies the importance of ensuring that health staff and others are oriented to key breastfeeding information and IYCF-E principles and know the referral pathways for breastfeeding women experiencing difficulties. 41
Assisting breastfeeding mothers in special circumstances
Mothers mix-feeding infants younger than 6 months should be sensitively encouraged to transition their infants to exclusive breastfeeding if possible.23,25 These mothers should be encouraged to breastfeed their infants frequently to increase milk production and infant breast milk intake. 42 Skilled breastfeeding support will likely be necessary. Infants will require some supplementation with donated milk, wet-nursing, or CMF until mothers can exclusively breastfeed.
It is vital that breastfeeding mothers who are separated from their infants begin to express their milk frequently or, if appropriate, wet-nurse other infants to maintain their own milk production. Milk expression (or wet-nursing) should begin as soon as possible after separation from their infant. If they express their milk, this milk may be available to nearby infants for informal milk sharing, if that is appropriate given the circumstances. Skilled breastfeeding and emotional support would be very helpful to these mothers.
Mothers who exclusively express milk to feed their infants have particular challenges during an emergency. They may have been accustomed to using breast pumps to express their milk and bottles to feed their infants, both of which require abundant hot water for effective washing. They may also need a power source if they use an electric pump. Their infant may or may not have experience with direct breastfeeding and may thus be unfamiliar with how to breastfeed effectively or be reluctant to do so. In addition, such mothers may depend on caches of their milk stored in a refrigerator or freezer, which may be compromised in a power outage, and they also may not have access to their stores of milk if they are evacuated from their homes. In recognition of the difficulty of washing breast pumps effectively, the OG-IFE states that use of breast pumps “should only be considered if their use is vital and where they can be cleaned, as in a clinical setting.” (page 13) 23 Mothers who have been exclusively expressing should be encouraged to transition their infants to direct breastfeeding if possible and provided with skilled support to do so. If they are unable or unwilling to make this transition, women who are exclusively expressing should be taught how to hand express and cup feed their infants. Cup feeding is discussed in a later subsection in relation to CMF feeding.
In circumstances in which either the breastfeeding mother or the infant or young child is hospitalized with injuries, keeping mothers and infants together and supporting breastfeeding can be crucial to their recovery, and emergency protocols should address this possible scenario. Breastfeeding can help stabilize the vital signs of mothers and infants. 17 For mothers, the presence of her infant can help her recovery and provide her with a stronger will to recover. 17 Refer to ABM Protocol #35, Supporting Breastfeeding During Maternal or Child Hospitalization. 17
It is important to ensure safety and support to families who have vulnerabilities related to domestic violence, disability or medical conditions, religious or cultural needs, marginalization or other special needs.
Relactation, wet-nursing, and donor milk for nonbreastfed infants
For infants younger than 6 months who are not breastfed, the OG-IFE calls for relactation, wet-nursing, or donor milk, in that order. Only if all these options are not acceptable or feasible is support for CMF feeding for infants younger than 6 months old appropriate. 23 The IFE Core Group has produced an infographic summary on how to support nonbreastfed infants in emergencies to guide policy development and individual action. 43
Relactation is a process in which a woman who has given birth and stopped breastfeeding this infant or breastfed a previous infant is stimulated to restart lactation. (All women initially lactate after birth, although not all breastfeed.) Induced lactation refers to a process in which a woman who has never given birth is stimulated to lactate. 44 Relactation may be undertaken by the mother of the infant, or if she is not available, relactation or induced lactation may be undertaken by a family member such as an aunt or grandmother, who may volunteer to wet-nurse the infant. Women who are strongly motivated to relactate will be more likely to be successful than those who are less strongly motivated. 45 Women are also more likely to be successful in relactation if those supporting them are confident in relactation as a process. 46 Guidance for health providers on supporting relactation is available from the World Health Organization in its publication Relactation. 44 A systematic review of relactation, which included a humanitarian setting, found that the start of milk secretion varied from 2 to 15 days, mixed feeding was achieved between 2 and 18 days, and exclusive breastfeeding could be achieved from 3 to 30 days. 47 Mothers who had most recently stopped breastfeeding and who were not using bottles had greater success, and mothers do better with more intensive support, particularly in the first 10 days. 47 Equipment for supplementation while suckling at the breast, including supply tubing (also called a breastfeeding supplementer or supplemental breastfeeding system), may be used where hot water for washing is available such as in a clinic setting. 48 Women who have recently stopped breastfeeding any child younger than 6 months should be counseled to consider relactation, although relactation can be tried for infants and children who are older as well. 49 Skilled breastfeeding support is very important for these mothers,23,47 although relactation in emergencies has been successfully supported by health workers with limited experience. 50
After relactation, wet-nursing is the next feeding option to consider in emergencies, both for infants who are not breastfed and for separated mothers and infants. Wet-nursing, the practice of family and community members breastfeeding an infant that is not their own, has long been a part of infant feeding in many societies through much of human history. It can be considered if it is acceptable to the mother and the family of the infant and a suitable wet nurse can be identified.2,23,51 It is important to note that while wet-nursing may not be culturally acceptable in some settings, emergencies can change perceptions. 52 Recent experiences during the Ukraine war saw wet-nursing serving as a lifeline for infants trapped under siege, where sometimes individual mothers fed multiple infants. 53 It is therefore important not to prejudge whether an infant’s family will consider wet-nursing. 52 Close relatives (such as sisters, aunts, and grandmothers) or friends are more likely to be acceptable as a wet nurse than someone unknown to the family. 52 However, wet-nursing by strangers, including emergency responders (who may undertake this role on a short-term basis), also occurs during emergencies. 54 The legal and regulatory framework for wet-nursing and donor milk use, particularly in emergencies, may vary from country to country or may be absent. 51
Wet-nursing can also help a mother maintain her milk production if she is separated from her own infant. Prospective wet nurses should undergo HIV counseling and rapid testing if it is feasible, and if it is not feasible, they should undergo an HIV risk assessment. 23 Wet nurses should be appropriately supported in this important work, which may include provision of resources, but care should be taken to ensure that women are not coerced by family members or otherwise to wet-nurse. 52 Refer to OG-IFE and the Operational Guidance: Breastfeeding Counseling in Emergencies for more information regarding HIV.23,26
Donor milk should ideally come from milk banks, where it is pasteurized and where donors have been screened. Some countries have robust milk banking systems, which makes this a possibility. For example, banked milk has been provided to emergency shelters for use to feed nonbreastfed infants in some emergencies in the Philippines. 55 However, not every country has such capacity. Donor milk from milk banks requires a cold chain, logistical support, and a strong management system.23,51 Power outages and transportation issues may pose significant logistical challenges to using banked milk, even where it exists. In addition to infrastructure challenges during a disaster, excessive attention to donated milk risks diverting attention away from breastfeeding support. 51 International donations of banked donor milk should not be made. 23 When donor milk is in short supply, it should be prioritized for low birthweight infants, premature, and sick infants. 23 Milk banks should develop emergency preparedness plans, which include how to stockpile supplies for an emergency, developing criteria and logistics for distribution of milk during an emergency, and how to solicit milk and monetary donations during an emergency.
Milk may be shared directly from one mother to another mother or caregiver during emergencies. The OG-IFE notes that there is little experience with informal milk sharing in this setting. 23 However, a recent report from Ukraine described the sharing of expressed breast milk during conflict. 53 ABM has a Position Statement on Informal Milk Sharing (2017), but it is not specific for disaster situations, and it calls for prospective recipients to screen the donor for use of medications compatible with breastfeeding, tobacco products, use of substances that are not compatible with breastfeeding (such as cocaine), and infections such as HIV, and HTLV-1 (in endemic areas). 16 This guidance contrasts with the OG-IFE, which only recommends testing or screening for HIV23 and screening for HIV would be the most important consideration for informal milk sharing in an emergency situation.
The issue of milk kinship should be considered with wet-nursing or milk sharing among Muslim families. 56 Although it is sometimes believed that Islamic milk kinship precludes wet-nursing or milk sharing, this is not the case. In fact, there is a strong history of wet-nursing in Muslim cultures and identification and documentation of the donor or wet nurse will often be enough to address any concerns related to milk kinship. 52 Involvement of trusted religious leaders can also facilitate the acceptance of wet-nursing. 52
The capacity of wet-nursing and milk sharing to support the health and well-being of nonbreastfed infants points to the contribution of high breastfeeding rates to community resilience in disasters. Government investment in supporting breastfeeding should be considered an essential emergency preparedness activity as having more breastfeeding women in a community can be lifesaving for all infants (breastfed and nonbreastfed). 53 All emergency plans and policies should include breastfeeding support.
Minimizing the risk of artificial feeding with CMF
Infants younger than 6 months for whom breastfeeding or the provision of breast milk is not possible should be supported in CMF feeding. Nonbreastfed infants who are older than 6 months can be fed with animal milk, CMF (only up to 12 months), plus appropriate complementary solid foods. 57 CMF is not recommended for children older than 12 months. 57 Note that feeding with animal milk might increase the risk of iron deficiency, 57 so ensuring iron-rich complementary foods is of increased importance for such infants and supplementation with iron may be necessary if these milks are used. A decision to provide CMF to infants who cannot be breastfed entails a significant commitment. It is much more costly to support CMF feeding than breastfeeding, especially in a humanitarian crisis. 58 Organizations that distribute CMF in emergencies are required to provide it for as long as the child needs and to ensure that all resources necessary to feed CMF with an acceptable level of safety are available to the caregiver.23,25 These resources include clean water for reconstitution and washing, an ability to heat water for reconstitution and washing, and feeding implements, as well as individualized education and health monitoring and health care. CMF should not be distributed without individual assessment of need by a suitably qualified person.23,25 Emergencies bring elevated rates of infant morbidity and mortality, particularly for infants who are not breastfed or not exclusively breastfed,59–61 which is the primary reason why supply of CMF should be tightly controlled and must be accompanied by a comprehensive package of support.
Temporary provision of CMF is indicated for those infants younger than 6 months whose mothers (or caregivers) are relactating, who are transitioning from mixed feeding to exclusive breastfeeding, those enduring short-term maternal separation, or awaiting donor milk or wet-nursing. 23 Longer term CMF is appropriate for infants until 6 months who were dependent on CMF pre-emergency, whose mothers cannot or are unwilling to relactate for whatever reason, or for whom donor milk or wet-nursing is not an option, for whatever reason. Other indications, as outlined in the OG-IFE, include orphaned infants, infants whose mothers are absent long term, infants of mothers with recognized medical conditions in which breastfeeding is contraindicated, a very ill mother unable to breastfeed, an infant rejected by the mother, and a sexual assault survivor not wishing to breastfeed. 23 Maternal desire to formula feed without one of these reasons is not an indication for CMF provision, and CMF provision should be avoided absent one of the above reasons.
The OG-IFE, Sphere Handbook and the WHO International Code of Marketing of Breast-Milk Substitutes (the Code) specify that CMF for infants who cannot be breastfed must be purchased rather than donated, as experience has shown that donated CMF is often improperly distributed.23,25,62,63 For example, after the Yogyakarta, Indonesia earthquake in 2006, three-quarters of households with an infant 0–5 months received donated infant formula 59 despite high levels of breastfeeding before the emergency. (See subsection Donations of CMF and other infant feeding products for more information on donations of CMF.)
Any CMF provided by emergency relief personnel to caregivers should be purchased rather than donated.23,25 In humanitarian contexts, UNICEF is the agency through which CMF should be procured, and it has a procurement guide for this process. 64 There are a number of factors to consider when purchasing CMF for use in an emergency. For a variety of reasons, infant formula (commonly called “stage 1”) should be purchased for use in any CMF program, including for feeding of infants 6–12 months. 65
Liquid ready-to-use infant formula (RUIF) has the advantage of not requiring reconstitution and is sterile, but it is also expensive, bulky, and heavy and so can be difficult to store and transport. Because it is sterile, RUIF may be erroneously perceived as not having any risks associated with its use, which may lead to overuse. RUIF is also not available in all locations, may only be available in large volumes (e.g., 450 mL sizes), and may not be acceptable to caregivers unaccustomed to this form of CMF. Where RUIF is used, it should be purchased in small serving sizes with caregivers educated on the need to discard excess milk following feedings. 65 Powdered infant formula (PIF) requires clean water for reconstitution and it is also recommended that hot water be used for reconstitution to kill pathogens that may be present in the powder. 66 The WHO recommends water (including bottled water) be brought to a rolling boil and allowed to cool to no less than 70°C/130 °F (waiting 5 minutes, e.g., but the WHO specifies no more than 30 minutes), before PIF is added. 66 After mixing water with PIF, the reconstituted CMF should be quickly cooled by running it under cold water or putting into ice, and it should be checked to make sure it is cooled to a temperature safe for consumption. 66 However, this can be extremely difficult to do in emergencies. Concentrated liquid formula is not recommended for use in emergencies due to potential errors in dilution. 23 CMF should be labeled with instructions in the language understood by those using it. As previously noted, when infant formula is provided, individualized education on use should also be given. For further information on infant formula procurement in emergencies, see Gribble and Fernandes (2018) 65 and the OG-IFE guidelines. 23
Figure 1 illustrates the feeding options in order of priority for infants younger than 6 months during emergencies.
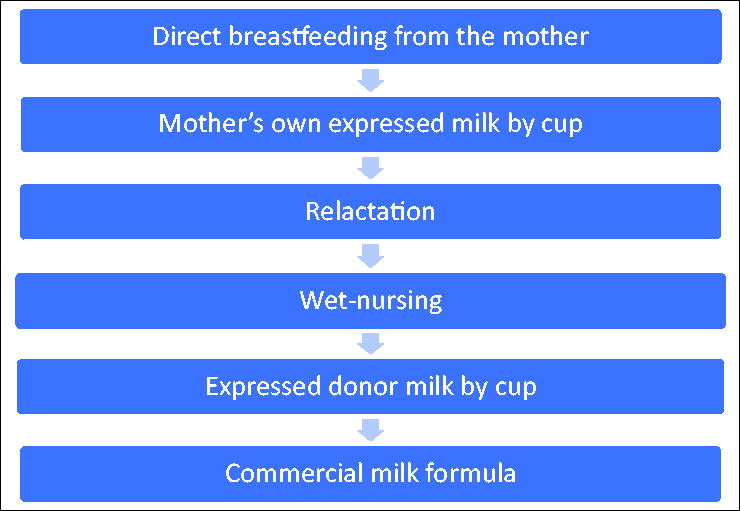
Feeding options in order of priority for infants younger than 6 months in emergencies. Note: In instances in which any of these resources conflict with the Infant Feeding in Emergencies: Operational Guidance (OG-IFE), the OG-IFE guidance should be followed.
Cup feeding
Caregivers of infants who are being fed expressed breast milk or CMF should be encouraged to use cups rather than bottles and teats to feed their infants in any circumstance where liberal hot water for washing is unavailable. 23 This is because cups can be properly cleaned more easily and thoroughly than bottles and teats. Even newborn infants can feed with a cup, and guidance is available on how to support caregivers with cup feeding. 67 Small cups where fingers can easily reach to the bottom when cleaning (and without a spout) are best. Small disposable plastic or paper cups avoid the need for washing and can also be used. Cups with lids might be necessary for caregivers who are traveling. If caregivers are unwilling to use cups, risk mitigation strategies should be put in place where possible, for example, sterilization facilities on-site (in addition to washing sites) and provision of instructions on how to sterilize at home. 23
Donations of CMF and other infant feeding products
Donation and inappropriate distribution of CMF and other breast milk substitutes are a pervasive problem globally, and extensive evidence shows that donations increase use of CMF by breastfeeding mothers in emergencies and undermine appropriate support for nonbreastfed infants.35,41,53,59,65,68–71 Donations of CMF are commonly far in excess of that required, in the wrong place, of the wrong type, and close to or past expiry. 65 Donations are difficult for emergency relief workers to manage and are often distributed indiscriminately, including to breastfeeding women. For a variety of reasons, the presence and distribution of donations commonly result in women terminating exclusive or any breastfeeding.59,68–70 After the Yogyakarta earthquake in Indonesia in 2006, nonscreened distributions of CMF saw infants (0–5 months) whose households were provided with donated CMF being 60% more likely to have been fed CMF in the previous 24 hours and more than twice as likely to have had diarrhea in the last week than infants whose households had not received donated CMF. 59 Donations also undermine the well-being of infants who cannot be breastfed as distribution is rarely accompanied by the supplies and support needed for use with an acceptable level of safety. 65
Donations may be made by well-meaning members of the public, governments, nongovernmental organizations, or businesses (encouraged by media reporting),65,72 or made by CMF manufacturers as a way of promoting their products. 73 Donations made in emergencies by the CMF industry are a part of a pattern of exploitative marketing to undermine breastfeeding and encourage the unnecessary and harmful use of their products.74,75 Donation of CMF and other breast milk substitutes in emergencies is in breach of the Code. 63 The OG-IFE and the Sphere Handbook expressly prohibit accepting and soliciting donations of CMF and urge action to prevent donations.23,25 A scoping review of high- and middle-income countries found that violation of the Code was widespread and problematic, including acceptance of CMF donations and lack of knowledge of the Code by aid workers who often were unwilling to follow OG-IFE protocol. 39
Any donations of CMF that are made should be collected and disposed of; options for disposal include feeding to animals, or mixing with a cereal to be used as a complementary food. 23 However, it should be recognized that throwing out or destroying donated CMF is often difficult to do, even in high-income countries. For example, donations of expired CMF made after the 2011 Christchurch earthquake remained in health facilities for months. 76 Prevention of donations through policy and prompt media communications are therefore critically important. If breastfeeding women have already received donated CMF or other milk, they should be advised to use it only to prepare food for children older than 6 months or to drink it themselves.
Donations of commercial complementary foods should not be solicited, accepted, or distributed. 23 Problems underlying guidance to reject donations of commercial complementary foods include the following: nutritional poverty, labeling in breach of the Code (including suitability for infants younger than 6 months), commercial exploitation of emergencies, displacement of local foods, excessive and discontinuous supply, and time-resourcing requirements to manage donations. 77
Donations of any form of breast milk substitutes (e.g., baby teas and juices and toddler milks), bottles and teats, and breast pumps should not be accepted. 23 The IFE Core Group has produced an infographic to guide preventing and managing inappropriate donations. 78
Purchasing and distributing CMF so that breastfeeding is protected
Where CMF is purchased, distribution is more carefully managed as it must be budgeted and accounted for. This has been shown in nonemergency settings in hospitals. 79
Ensuring that CMF is distributed only in cases of genuine need in line with the OG-IFE is challenging, particularly where breastfeeding women have requested CMF, which is a common situation. Maternal requests for CMF are often related to the previously described belief that stress reduces milk production or other concerns related to breastfeeding inability. Additional underlying issues may be related to normalization of CMF feeding within the culture creating an expectation to formula feed, an aspiration to formula feed, or simply that CMF is a high-value product. The impact of pre-emergency exploitative marketing of CMF should also be appreciated such as the case of the Syrian refugee mother described by Palmquist and Gribble who was concerned that not feeding CMF would be detrimental to her infant’s immune system. 80 Research on experiences regarding CMF distribution during the European Refugee Crisis of 2015-16 identified that good practice in distribution of CMF was facilitated by the following: the presence of breastfeeding support, presence of properly implemented CMF programs, understanding maternal choice to formula feed should be considered within the risk context of the emergency, consideration of CMF as more similar to a medicine than a food in emergencies, and positive personal breastfeeding experiences of emergency relief personnel. 41
Any CMF should be kept out of public view, and distributed discreetly so as not to discourage breastfeeding mothers. 23 Using a system to identify those caregivers/mothers who truly need this product can be helpful. In the Za’atari refugee camp in Jordan, a system of prescription was developed that ensured that CMF was distributed only to those needing it and accompanied by appropriate support. 81 Among the benefits of this system was that the selling of excess CMF in the camp ceased. In addition, consideration should be given to providing breastfeeding women with something of a similar value to goods provided to CMF caregivers (e.g., additional food rations, a breastfeeding shawl, or a cooking pot) so as not to discourage breastfeeding. 65
Given the importance of preventing donations of CMF and the exploitation of emergencies by CMF manufacturers, all health care professionals should be familiar with the Code and support national efforts to implement the Code and the subsequent World Health Assembly resolutions.39,63 Practical advice on how to accomplish this can be found in the World Health Organization’s Guidance on Ending the Inappropriate Promotion of Foods for Infants and Young Children. 82
Complementary Feeding in Emergencies
Complementary foods (solids) should not be fed or provided to infants younger than 6 months, as this may contribute to making infants vulnerable to infectious disease and malnutrition. 57 Complementary foods for infants older than 6 months should be of the appropriate amount, consistency, variety, and nutritional quality. 57 They should also be acceptable to caregivers.
Supporting Breastfeeding Mothers and Caregivers of Infants in Emergency Shelters
In many contexts, emergency shelters are set up to provide temporary refuge and resources to emergency-affected populations. Such venues may be in existing buildings or may be in temporary structures such as portable buildings or tents. Depending on the emergency, the longevity of such shelters may be as short as several hours or days or weeks to months. Some people may use emergency shelters to access resources but not sleep there. Emergency shelters are an important venue for provision of breastfeeding and infant feeding support.
Those caring for infants should be identified upon entering shelters to determine their immediate and medium-term needs. This may be facilitated through a registration process. Those who may require immediate assistance include the following: women experiencing difficulties breastfeeding, breastfeeding infants and mothers who are separated from one another, women who are exclusively dependent on breast pumps for providing breast milk for their infants, infants younger than 6 months who are not currently breastfed, mothers with infants younger than 6 months who mix feed (i.e., partially dependent on CMF), and orphaned infants and young children. A recent comprehensive review of ICYF-E by Bilgin and Karabayir has a helpful intake form that can be used in the registration process. 83
Ideally, health providers with skills in IYCF-E, including those trained in breastfeeding support, should be available on-site to assist mothers and caregivers with infant and young child feeding-related needs. Otherwise, off-site support, including via telephone, should be made available. Lack of privacy in emergencies has often been identified as a barrier to breastfeeding and can reduce feeding frequency resulting in reduced milk production.39,69,72 Therefore, venues of evacuation or shelter should have private spaces in which women can breastfeed their children, with the amount of privacy that the mother requires according to local cultural practice.
It should be ensured that caregivers of CMF-dependent infants, or those providing CMF temporarily while relactating or otherwise awaiting resumption of breastfeeding, have a clean space within shelters to prepare feeds, and, if possible, to wash feeding implements. Emergency relief personnel should be proactive in ensuring that CMF is not prepared or feeding implements washed in the bathroom/toilet facilities to minimize the risk of fecal–oral contamination of infant food. Where appropriate facilities for washing, including hot water, are not available, single-use feeding implements should be available.
Caregivers of all infants should be prioritized for access to resources, including food and water, so they do not need to stand in long queues for hydration and food. 29 Prioritization may be assisted by providing mothers and caregivers, for example, with a card, note, or lanyard to present to staff. 29 Ensuring women have easy access to toilet facilities will reduce the possibility they will restrict fluid intake and become dehydrated and risk reducing milk production. Providing a separate, supported space in emergency shelters for families with infants and young children can help in providing targeted assistance and safety. 29
Supporting Mothers, Caregivers, and Children via MBAs
MBAs, also called “Baby Friendly Spaces” and “Baby Tents,” have supported the well-being of pregnant women and new mothers and assisted them in caring for their infants and young children during and after emergencies since the Balkan crisis of the late 1990s. 84 MBAs are a safe, comfortable, and welcoming space for mothers and other caregivers of infants and young children to rest, connect with one another, access health care and referral to services, and receive psychological support, help in caring for their children (including feeding), and other supports that can help them and their families. 85 MBAs can be set up within community buildings such as schools or religious or health institutions or in temporary buildings, tents, or caravans and have been deployed in a large number of countries and different emergency types, including earthquakes, hurricanes/cyclones, floods, and war and in refugee camps. Ideally, MBA staff should have expertise in infant and young child feeding and provision of psychological support.
Research conducted by Action Contre la Faim in refugee camps in Cameroon saw women who attended MBAs experiencing less suffering and difficulties with breastfeeding and improved well-being, social support, and interaction with their infants. 34 Support for relactation and wet-nursing can be provided via MBAs. MBAs can be used for controlled distribution of CMF, including instruction in preparation and cleaning of feeding materials. 35 However, care needs to be taken to ensure that this support does not undermine breastfeeding. This may mean that CMF-focused support is provided at separate times from breastfeeding support. 23 MBAs may provide support for only a few days, as occurred in a New Zealand hospital ward after the 2011 Christchurch earthquake, 86 or for many months to a year or more. In an emergency that lasts long-term and with particular food insecurities, MBAs can assist in giving attention to the nutritional status of breastfeeding mothers and to young children, and importantly, ensuring adequate attention to micronutrients. 87 Some mothers may not have the mobility to access an MBA, so it may be important to have skilled breastfeeding supporters available who can travel to mothers who require help. Remote breastfeeding support during a disaster can prove valuable. 53
Emergency Preparedness Training Curriculum Regarding Breastfeeding
It is essential that emergency relief personnel working with pregnant women, new mothers, and other caregivers of infants and young children be trained to understand the vital role of breastfeeding in emergencies. They should learn the basics of lactation physiology and the WHO recommendations for infant and young child feeding. Aid workers should know the preferred order of feeding options for nonbreastfed infants. They must know that donations of CMF and other breast milk substitutes should not be solicited or accepted and about appropriate and discreet storage and distribution of CMF. Aid workers should be trained to recognize which infants have appropriate needs for CMF, and which mothers should be referred for skilled breastfeeding support (if they do not have these skills themselves). They should be educated about cup feeding and avoidance of feeding bottles and teats. They should know about proper preparation of CMF.
Training of emergency relief personnel working directly with mothers should include how to handle frequently encountered breastfeeding issues, such as mothers reporting stress affecting their milk. Gribble and Palmquist have suggested that emergency relief workers be taught appropriate counseling skills so that they know how to respond to maternal requests for CMF. 41 They suggest aid workers be encouraged to understand the ethical framework underpinning CMF provision requirements in the OG-IFE so that they are better able to respond appropriately to maternal requests. 41 Personnel should be trained to counsel women based on evidence, free from bias from their own personal experiences with CMF. 41 Those working in an IYCF-E role may benefit from debriefing of their own infant feeding experiences and on reflective practice. 41 They should be trained to never advise mothers to stop breastfeeding without a compelling evidence-based medical reason, and that mild maternal illnesses are not a reason to stop breastfeeding.
Emergency relief personnel need to be aware of local cultural beliefs around breastfeeding and be prepared to counsel mothers with accurate information. 28 Finally, emergency relief workers should receive training on the International Code of Marketing of Breast Milk Substitutes (the Code), why CMF donations should not be accepted in an emergency, and how untargeted distribution of CMF undermines breastfeeding and infant and maternal health.
The Role of Medical Doctors in Protection, Promotion, and Support of Breastfeeding During Emergencies
During routine care, doctors should promote breastfeeding to all women as the standard of infant nutrition and provide the support needed for women to breastfeed in line with international recommendations, and to help them reach their breastfeeding goals. 88 Doctors should emphasize breastfeeding as part of emergency preparedness in locations where emergencies are seasonal, and as part of their usual anticipatory guidance, doctors should advise mothers to continue breastfeeding until after the risk period ends.
Doctors should also work to implement and support the BFHI. High precrisis implementation of the BFHI in Ukraine greatly helped the resiliency and response of mothers and providers during that armed conflict. 53 Conversely, poor hospital practices, such as unnecessary separation of mothers and infants, can undermine the establishment of breastfeeding when it is most needed.
Medical doctors should also encourage direct breastfeeding and discourage the practice of exclusively using breast pumps for feeding when it is not medically necessary. This is especially important for those using electric pumps, given the rising occurrence and duration of power outages in some locations. 89 Doctors should encourage women who are dependent on breast pumps to seek professional help to transition to direct breastfeeding and encourage all women to learn how to hand express even when no emergency exists. Doctors should particularly advise all mothers who exclusively use breast pumps to learn hand expression for times when access to electricity or sanitation is not possible.
Encouragement and support of breastfeeding include enhancing women’s confidence in their ability to breastfeed as this has been correlated with breastfeeding success. Conversely, lack of self-efficacy makes it less likely for women to breastfeed during an emergency. 70 This underlines the importance of doctors having not just clinical knowledge but also breastfeeding counseling skills.
Preexisting cultural beliefs may limit uptake of breastfeeding even before the emergency. 28 It may help for doctors to work with other community leaders to understand the underlying issues, and work collaboratively to take into account beliefs and barriers that limit breastfeeding. 33
During emergencies, doctors should ensure that women who give birth are supported with standards of care that support breastfeeding. Specifically, women and newborns should experience skin-to-skin care in the first hour of life, early initiation of breastfeeding, and the other maternity practices that comprise the WHO/UNICEF Ten Steps to Successful Breastfeeding. 90 During emergencies, doctors who work with women and children can make their offices available as havens for breastfeeding support, if they are able to provide it. 29
Furthermore, medical doctors, especially those who care for children, should be involved in emergency preparedness plans as governmental and philanthropic organizations may not be aware of the importance of breastfeeding to these plans.
Educating the Public
During an emergency, members of the public, often far from the event, want to help. Members of the public should be encouraged to give monetary donations rather than goods to enable resources to be provided when, where, and in the form required and to avoid the “second disaster” caused by an influx of donations 91 and the particular harms caused by infant feeding-related donations. Breastfeeding mothers living far from the disaster can donate their milk via local milk banks but should not seek to send their milk to the emergency area. The public should be specifically discouraged from donating CMF and from sending CMF to an emergency area. 23
Other Considerations
It is important to specify that breastfeeding is important in emergency situations, not merely human milk, and the two terms should not be used interchangeably in policies or elsewhere. While human milk is superior to animal milk or CMF, feeding human milk without direct breastfeeding requires expressing milk and feeding using cups or other equipment, all of which are challenging during an emergency and present hygiene risks, and additionally may not provide the same immune protection to the child. 92
Lack of emergency preparedness for infant and young child feeding appears to be a global problem.93–95 Mapping of many plans to deal with humanitarian emergencies has shown inadequate attention to infant and young child feeding issues. 96 Emergency preparedness plans should be audited periodically.
Disaster-Specific Information
Blizzards
Blizzards may leave people trapped in their homes (or other locations) for days, often without electricity. This situation will most affect mothers who exclusively feed pumped milk, and all mothers who have caches of frozen stored milk. If exclusively pumping mothers do not have a manual pump available and/or power to heat water for washing, they should hand express their milk and/or attempt to directly breastfeed their infants. Trained breastfeeding help may only be available remotely and only if there is electricity to power mobile devices or the internet. It is often unknown how long a power outage will last when it begins. One must weigh opening the freezer door against using contents within the freezer. Using stores of frozen milk before using freshly expressed milk may make sense, particularly if there is concern that frozen milk may thaw and spoil. If outdoor temperatures are consistently well below freezing, one can consider moving frozen milk stores outdoors, stored in a container that would be safe from tampering by animals.
All families experiencing power outages will face challenges preparing food for themselves and should follow local guidelines.
Fires
Women and children exposed to wildfires may be exposed to particulate matter on their hair and clothing, and may have inhaled toxins from burning buildings, including polyaromatic hydrocarbons (PAHs). Research from the Australian bushfires of 2019–2020 suggests that the amounts of such PAHs in breast milk were low and no samples contained lead, chromium, nickel, or aluminum. 97 Women should be reassured that there is no concern regarding breast milk and exposure to bushfire smoke. Women may also be prone to dehydration and missed feeds due to heat and rushed evacuation, leading to compromise of milk production. Rehydration and increased feeding frequency will be necessary. In heavy smoke, infants may be fussy at the breast and come on and off the breast to breathe (similar as to if they have a blocked nose with a cold). 29
Earthquakes
Earthquakes occur without warning and may result in mother–infant separation or circumstances in which either the mother or infant is either injured or dead. Typically, multiple aftershocks follow the initial earthquake, which may cause further damage and collapse of buildings, causing uncertainty and anxiety. In China, concern about future collapse of hospital buildings led to a marked increase in cesarean deliveries to eliminate uncertainties about birth timing. 98 Families may be in temporary housing for extended periods of time and may be without reliable power, clean water, or food. Skin-to-skin contact for infants may be especially important to keep infants warm and calm if availability of safe warm shelters is limited. Concern regarding aftershocks may result in mothers being unwilling to put their infants down, which will support frequent and continued breastfeeding.
Floods
Floods, including those accompanying hurricanes and typhoons, are often complicated by the contamination of floodwaters with raw sewage and chemical toxins, which then also contaminate drinking water and any surfaces the water touches. Breastfeeding is particularly important because of the protective impact of breast milk against diarrheal disease and because the availability of safe clean water to wash infant feeding supplies and reconstitute CMF may be compromised. Mothers who exclusively pump their milk are at high risk and should be aided in transitioning to direct breastfeeding as soon as possible.
Armed conflicts
A systematic review has shown that despite its importance to child survival, breastfeeding is reduced in areas of conflict. 99 Armed conflict situations tend to last longer than those of natural disasters. Therefore, the nutritional needs of children may be a long-term concern. For example, infants older than 6 months are unlikely to have severe nutritional deficiencies within one to two weeks if they are not fed appropriate complementary foods. Over the course of months, however, it is important to ensure that the nutritional status of such infants is stable, including adequate macro- and micronutrients. Supporting infant and young child feeding during armed conflict can be particularly challenging as personnel and supply access to affected populations may be difficult or impossible.
Armed conflict often has constantly changing areas that are impacted. The impact to structures such as roads and water lines may be similar to that of natural disasters, but there is the additional challenge of providing services under fire. Emergency plans need to include protections of mothers and infants from aerial attack (bomb shelters) and supply distribution to civilians in battle conditions. As with earthquakes, there may be situations in which either mother or child is either injured or dead and the same supportive provisions apply.
The possibility of sex-based violence adds to all the other factors that make uptake of exclusive breastfeeding challenging in armed conflict. 28 In addition, attention to both cross border and internally displaced refugees is needed. 27
Nuclear power plant accidents
The IFE Core Group has issued guidance on management for breastfeeding mothers and children in the first three days after a nuclear power plant accident, noting specifically that this guidance does not apply to nuclear weapons. 100
Potassium iodide (KI) is recommended for breastfeeding women and breastfeeding children because nuclear plant accidents cause emission of an iodine isotope (I-131), which can damage the thyroid. KI prevents this isotope from entering the thyroid gland. It should only be taken if authorities recommend it. 100
In nearly all cases, continuation of breastfeeding is recommended. The rare advice to temporarily stop breastfeeding is if the mother–infant pair was very close to the reactor, and cannot shelter in a safe location, and KI is not available, and the mother either has previously expressed milk available and access to safe feeding and cleaning supplies, or a safe supply of CMF and a safe way to prepare it. 100
Infectious disease outbreaks
Infectious disease outbreaks, including epidemics and pandemics, can pose challenges to infant feeding. The IFE Core Group has published two infographics to guide policy makers and program managers on the management of infant and young child feeding in infectious disease outbreaks. 101 Their recommendations emphasize support of breastfeeding when it is known that breastfeeding is safe with a particular infection, and how to support breastfeeding when the type of infection requires temporary disruption of breastfeeding.
There may be circumstances in which a new pathogen emerges and the safety of breastfeeding is initially in question. In these cases, health authorities will seek expert opinions, which would weigh factors such as the likelihood that the pathogen can be transmitted via milk, and if so, whether it is likely to cause significant disease in infants by that route, and whether the pathogen could be spread to the infant by other routes during breastfeeding. For example, a pathogen may be spread by a respiratory route during feeding, which could occur regardless of the feeding method, and may be preventable by appropriate respiratory precautions. Health decision science can be used to inform interim guidance102,103 until recommendations from the World Health Organization are available. 104
Failure to appreciate the value of breastfeeding has had public health consequences during epidemics with new pathogen epidemics. When breastfeeding is assumed to be something dispensable, the default assumption is often it is safer not to breastfeed in situations of unknown safety. 105 Similarly, failure to appreciate the comparative risks of CMF feeding can lead to recommendations in which it is inappropriately recommended over breastfeeding, particularly in low-resource settings in which CMF is not acceptable, feasible, affordable, sustainable, and safe. Such early guidance around HIV was responsible for the unnecessary deaths of many infants. 106 Early in the COVID-19 pandemic, many health authorities immediately created policies of separation of infants from their mothers combined with CMF feeding over breastfeeding, which again likely resulted in unnecessary infant deaths.107,108 Breastfeeding specialists can play an important role in informing policy makers regarding the importance of breastfeeding and the risks of CMF feeding to ensure that both are appropriately taken into consideration when developing recommendations.
In the case of a new pathogen, when international guidance from the World Health Organization is not yet available, the IFE Core Group recommends that continuation of breastfeeding be prioritized and that close mother–infant contact be maintained until and unless there is good evidence to inform that ceasing breastfeeding is safer. 104 If women cease breastfeeding because of infectious disease concerns, they should be supported to maintain their milk production so that they can resume breastfeeding when they recover or if this is not possible, they be supported to relactate.
Prolonged heat and other climate change issues
Long-term extreme heat can contribute to drought and food insecurity, and prompt migration of large numbers of people. Hot weather is associated with reduced rates of exclusive breastfeeding that may be a result of less time spent breastfeeding or maternal dehydration.109,110 The UNICEF Technical Note, Protecting Children from Heat Stress, provides guidance on how to help protect pregnant women, new mothers, and infants from extreme heat. 110 In the face of adverse climate change impacts, breastfeeding provides an opportunity for mitigation, adaptation and community resilience. 111
Other emergency experiences
Other emergencies include those related to refugee camps, volcanic eruptions, landslides, tornados, famines, tsunamis, building collapses, and fires that may destroy a single large building (such as London’s Grenfell Tower Fire of 2017). In addition, there is the possibility of unconventional warfare. The IFE Core Group has information on chemical, radiological, and biological attacks. 112 Slowly, developing emergencies, including famines and drought, often have extended periods of food insecurity. Breastfeeding remains vitally important in such emergencies, but attention also must be paid to maternal nutrition. Each type of emergency will have its challenges but the general principles will remain the same.
Summary
Protection, promotion, and support of breastfeeding before any emergency are critically important. It is essential to promote exclusive breastfeeding during routine care, and provide the infrastructure to enable mothers to exclusively breastfeed during ordinary times. During a disaster, breastfeeding provides an important lifeline and breastfeeding support must be part of all emergency preparedness plans, policies, and training impacting families with infants and young children. Education of emergency relief personnel in the importance of breastfeeding and in the basics of breastfeeding management is vital. Given that mothers who are dependent on breast pumps are extremely vulnerable during emergencies, extra efforts should be made to discourage this practice and promote direct breastfeeding during routine care of mothers with newborns. Nonbreastfed infants are a vulnerable group and they and their caregivers require special support. Breast milk options for these infants should be first explored and if breastfeeding is not possible, they should be provided with a comprehensive package of support.
Future Directions
As the climate crisis continues to evolve, there will be more climate emergencies as well as migrations and climate refugees. Technology will affect types of armed conflict and ways in which we can support breastfeeding. Data regarding infant feeding should be part of information gathered in emergency situations so that global learning can occur and lead to improvements from one event to the next.
For an additional resource supporting the recommendations outlined in this position statement, please visit our website at //bfmed.org/position-statements to access a complementary handout.
Footnotes
Acknowledgment
The authors would like to acknowledge Alessandro Iellamo for his advice in reviewing the article.
Authors’ Contributions
M.B., K.G., and D.Z.: primarily drafted the article, with review and contributions from all authors.
Disclosure Statement
The authors have no conflicts of interest.
Funding Information
No funding was received in the production of this Position Statement.