
Abstract
Background:
Full oral feeding (FOF) is a critical milestone in preterm infants, often delayed because of immature feeding coordination. The Fucile oral motor stimulation protocol aims to address these challenges and enhance feeding progression. To evaluate the effectiveness of the Fucile oral motor stimulation protocol in reducing the transition time to FOF, shortening hospital stays, and improving feeding-related outcomes in preterm infants.
Methods:
A systematic review and meta-analysis was conducted following the PRISMA guidelines (PROSPERO: CRD42022369514). Databases, including PubMed, Scopus, Web of Science, CENTRAL, and CINAHL (1990–2024), were searched. Randomized controlled trials comparing the Fucile protocol with control interventions in preterm infants (<37 weeks of gestation) were included. Outcomes included transition time to FOF, hospital stay length, weight at discharge, and milk transfer rate. Risk of bias (RoB 2) and evidence certainty (Grading of Recommendations Assessment, Development, and Evaluation) were evaluated.
Results:
Nineteen trials (1,031 infants) showed that the Fucile protocol significantly reduced transition time to FOF (mean difference [MD]: −5.77 days; 95% confidence interval [CI]: −6.64 to −4.90) and hospital stay duration (MD: −6.47 days; 95% CI: −8.41 to −4.53) with moderate-certainty evidence.
Conclusion:
The Fucile protocol accelerates feeding milestones and reduces hospital stays for preterm infants, providing moderate-certainty evidence to support its clinical use. However, methodological limitations, including small sample sizes and risk of bias, underline the need for larger, high-quality trials to confirm these findings and refine clinical guidelines. These results suggest the potential of integrating oral motor stimulation into neonatal intensive care unit practices to enhance feeding outcomes and optimize care for preterm infants.
Introduction
Mastering oral feeding is a vital developmental milestone, particularly in preterm infants born before 37 weeks of gestation. 1 These infants often face significant challenges due to physiological immaturity, which involves struggling to coordinate sucking, swallowing, and breathing.1,2 As a result, they frequently require initial gavage feeding, which delays the transition to oral feeding and increases the risk of complications such as aspiration, apnea, and prolonged hospitalization.3,4
The prevalence of oral feeding difficulties among preterm infants highlights the need for targeted intervention strategies. 2 Although prevalence estimates vary, delayed oral feeding progression imposes significant medical, emotional, and economic burdens on health care systems and families. Beyond the immediate medical concerns, these challenges significantly impact long-term growth, neurodevelopment, and maternal–infant bonding. This underscores the urgency of implementing effective interventions, making them a priority for health care providers.5,6
Among the various interventions studied, oral motor stimulation has shown promise. 7 This technique was introduced by Fucile, Gisel, and Lau 7 and involves structured stimulation of oral and preoral regions for 12 minutes, followed by 3 minutes of non-nutritive sucking (NNS) using a pacifier or finger, administered at specific times before feeding. Evidence suggests that this approach improves feeding efficiency, reduces the time required to achieve full oral feeding (FOF), and shortens hospital stays.8,9 However, existing studies often suffer from limitations, including small sample sizes, inconsistent methodologies, and variable intervention protocols. 10
While previous systematic reviews and meta-analyses have attempted to evaluate the effectiveness of prefeeding oral stimulation strategies, their broad scope has hindered precise evaluations of individual protocols and has resulted in significant heterogeneity among the included studies. For example, Green 1 assessed multiple interventions, including the premature infant oral motor intervention, 11 the Fucile oral motor stimulation protocol, 7 and other techniques,12–16 making it difficult to isolate the specific efficacy of individual approaches.
Additional constraints, such as language restrictions in reviews, 17 have raised concerns about the reliability of evidence. The Cochrane Library highlights the importance of regularly updating systematic reviews to integrate new evidence and guide health policies. 18 Addressing these limitations requires a focused and comprehensive approach.
This systematic review and meta-analysis sought to evaluate the efficacy of the Fucile oral motor stimulation protocol for facilitating FOF in preterm infants. The primary outcome was the time to achieve FOF, while secondary outcomes included hospital length of stay, days of life at FOF, milk transfer rate (mL/min), and weight at FOF and discharge.
This study addressed a significant research gap by exclusively examining the Fucile oral motor stimulation protocol. By narrowing the focus, we aimed to reduce heterogeneity and provide more reliable and actionable insights into its effectiveness, addressing unresolved questions from earlier research. To ensure comprehensiveness, we expanded the search time frame and imposed no language restrictions. Furthermore, this review used rigorous methodologies, including the revised Cochrane Collaboration tool for assessing risk of bias (RoB 2) and the Grading of Recommendations Assessment, Development, and Evaluation (GRADE) framework, to ensure a comprehensive synthesis of high-quality evidence. By synthesizing available evidence, we aimed to inform clinical guidelines and optimize care strategies for this vulnerable population.
Methods
This systematic review and meta-analysis followed the PRISMA 2020 guidelines. 19 The research protocol was registered in PROSPERO (CRD42022369514) and received ethical approval from Zahedan University of Medical Sciences (IR.ZAUMS.REC.1402.237 and grant number: 10825). To ensure transparency, a detailed protocol article was published. 20
Literature search strategy
A comprehensive search strategy (Supplementary Data S1) was conducted across multiple databases, including Web of Science, Scopus, PubMed, CENTRAL, and CINAHL, covering the period from January 1990 to May 2024. Manual searches of reference lists and clinical trial registries (clinicaltrials.gov, WHO platform, and ProQuest) complemented the electronic search.
Eligibility criteria
The inclusion criteria for this study followed the Population, Intervention, Comparison, and Outcome framework. Participants included preterm infants born before 37 weeks of gestation. The intervention was the Fucile, Gisel, and Lau 7 oral motor stimulation protocol, compared with sham interventions, standard care, or other nonoral interventions. Eligible studies reported at least one feeding-related outcome, including transition time to FOF, length of hospital stay, weight at FOF and discharge, or milk transfer rate (mL/min). Exclusion criteria included studies involving infants with congenital anomalies, chronic medical conditions, or conditions affecting oral feeding. To ensure inclusivity, no language restrictions were applied. Non-English studies were translated into English using Google Translate, with relevant data verified for accuracy before incorporation.
Study selection and data extraction
Search results were imported into Rayyan software, where duplicates were manually removed. Titles and abstracts were screened by three independent reviewers (F.A., K.B., and G.G.) using predefined criteria. Unclear cases were retained for full-text review. Full-text screening was conducted by two independent reviewers (F.A. and G.G.), with disagreements resolved through discussion. Reference lists of included studies were reviewed to identify additional articles.
Data extraction was performed using a predesigned form, capturing study characteristics, participant demographics, intervention protocols, and primary/secondary outcomes (Supplementary Data S2 and S3). The primary prespecified outcome was transition time to FOF. Secondary prespecified outcomes included hospital stay length, milk transfer rate, and weight at FOF and discharge. Days of life at FOF were analyzed post hoc.
For studies with multiple groups, only data related to the Fucile protocol and its control group (CG) were analyzed to prevent unit of analysis errors and double counting. For multiple reports from the same study, the most comprehensive report was prioritized, supplemented with additional data from related publications.
Quality appraisal
The Cochrane RoB-2 tool21,22 was used to assess the risk of bias across five domains as follows: randomization process, deviations from intended interventions, missing outcome data, outcome measurement, and selection of reported results. Two reviewers (F.A. and G.G.) independently conducted the evaluations, resolving disagreements through consensus. Bias levels for each domain were categorized as low risk, high risk, or raising some concerns. Results were visualized using the Robvis tool developed by McGuinness and Higgins, 23 (see Fig. 1).
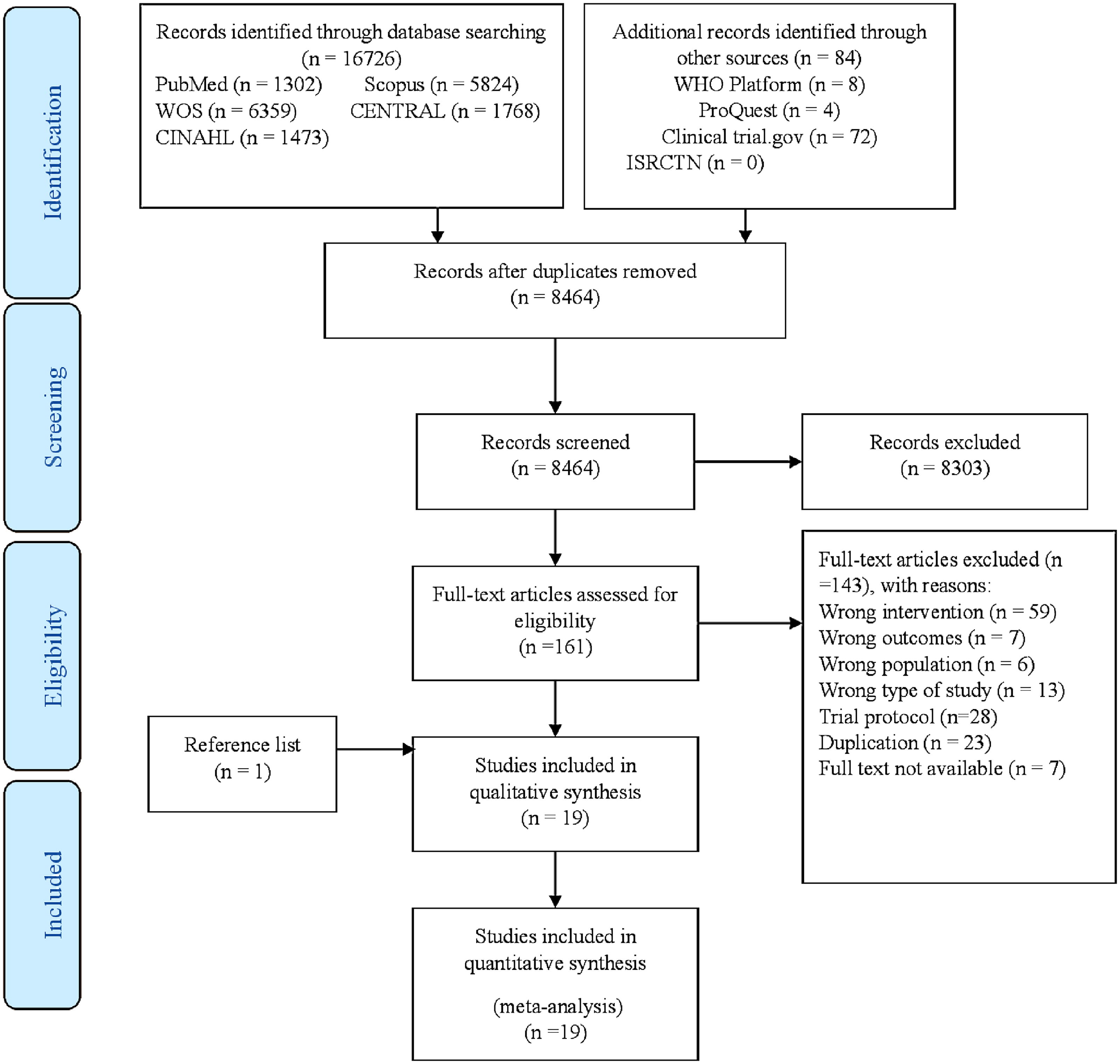
Flow diagram of search result.
Data synthesis and analysis
Analyses were performed using STATA version 16.1. A fixed-effect model with inverse variance weighting was applied due to the homogeneity of the intervention (Fucile oral motor stimulation protocol) and participant demographics. As the primary effect size measure (mean difference [MD] with 95% confidence intervals [CIs]) was not directly reported in most included studies, we calculated MDs using mean, sample size, and standard deviation (SD) data. For studies reporting medians and interquartile ranges, values were converted to means and SDs, using established methods. 24
Standardized mean differences (SMDs) were computed when appropriate. Depending on variance equality, as determined by Levene’s test, we used Hedge’s g (small sample sizes), Cohen’s d (large sample sizes), or Glass’s delta (unequal variances). Variance heterogeneity for outcomes such as weight at FOF and discharge, hospital stay length, and transition time at FOF necessitated the use of Glass’s delta. This precluded converting Cohen’s d to the number needed to treat (NNT) using the Furukawa and Leucht method. 25 For example, using a biased Cohen’s d, the NNT for transition time at FOF would have been three, indicating that one in three participants benefited from the intervention.
Heterogeneity and sensitivity analysis
Heterogeneity was evaluated using the Cochrane Q test and I2 statistic, with substantial heterogeneity indicated by a p value <0.1 and I2 > 50%. 26 Subgroup analyses, based on prespecified factors (e.g., gestational age, intervention frequency, birth weight, regional medical service levels, CG type, and quality scores), were conducted to explore heterogeneity sources.
Sensitivity analyses used the following three approaches: (1) the one-out removal method, recalculating MDs after excluding one study at a time to identify influential studies; (2) publication bias assessment using funnel plots, Begg and Egger tests (p < 0.1), and the trim-and-fill method; and (3) methodological quality sensitivity analysis.
Certainty of evidence at the outcome level was assessed using the GRADE approach. 27 Two authors (F.A. and G.G.) independently evaluated evidence quality, with GRADE not applied to outcomes supported by fewer than three studies. Details on the GRADE methodology and its interpretation are available in our protocol article. 20
Results
Study selection
Of the 16,810 records identified, 19 studies were included in this review, involving data from 23 studies with 1,031 participants. A PRISMA 2020 flowchart illustrates the screening, full-text review, and reasons for exclusion (Fig. 2). After removing duplicates, 8,303 records were excluded based on titles and abstracts, leaving 161 records for full-text review.

Risk of bias and overall risk for included studies (Domains: D1: Bias arising from the randomization process; D2: Bias due to deviations from intended intervention; D3: Bias due to missing outcome data; D4: Bias in measurement of the outcome; D5: Bias in selection of the reported result. Judgment: [] high; [ ] some concerns; [
] some concerns; [ ] low).
] low).
Study characteristics
The studies, detailed in Supplementary Data S2 and S3, included sample sizes ranging from 20 to 151 participants across diverse geographic contexts. The United States contributed 21% of the studies, while Brazil and China each accounted for 21%. The meta-analysis focused on studies using the Fucile oral motor stimulation protocol, with comparative groups classified as sham interventions (10 studies), standard care or no intervention (8 studies), and alternative interventions (1 study).
In studies with two intervention groups, data from the more relevant group were included. For instance, in Khalessi et al., 28 data from the once-daily, 10-day oral motor stimulation group were included. Similarly, in Harding et al., 29 data from the pretube feed intervention group were used. All interventions took place in neonatal intensive care units, with equal gender distribution and preterm infants’ gestational ages ranging from 27 to 33 weeks.
Outcome measures
The meta-analysis evaluated transition time to FOF, length of hospital stay, weight at FOF and discharge, milk transfer rate, and days of life at FOF. A fixed-effect model with inverse variance weighting summarized the mean effect size due to methodological homogeneity.
Primary outcome: Transition time to FOF
A total of 11 studies, involving 607 preterm infants, reported data on transition time to FOF. A fixed-effect model with inverse variance weighting was utilized for meta-analysis. The results indicated that oral motor stimulation could significantly reduce the transition time to FOF in preterm infants (MD = −5.77; 95% CI [−6.64, −4.90]; Delta glass = −0.79; 95% CI [−0.97, −0.62]), see Table 1 and Figure 3. These findings suggest a near-high-grade efficacy of intervention, with preterm infants in the oral motor stimulation group achieving FOF approximately 6 days earlier compared with the CG.
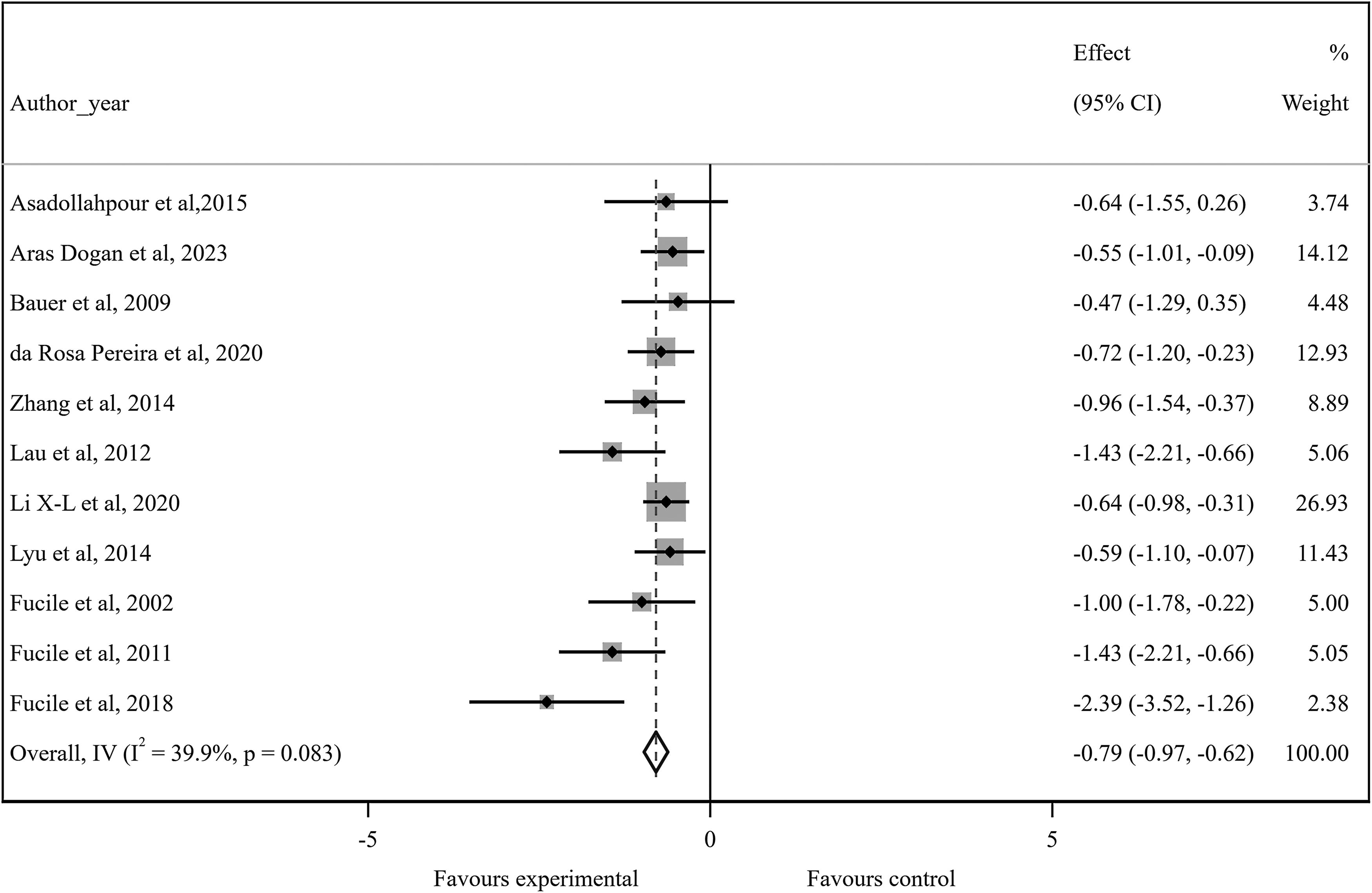
Meta-analysis of oral motor stimulation efficacy based on transition time to full oral feeding.
Summary Plot of the Effect of Oral Motor Stimulation on Oral Feeding Outcomes in Preterm Infants
□: 0 (not serious), ◪: ±1 (serious), ■: ±2 (very serious).
Due to the small number of studies, the GRADE was not done.
High: High confidence in the correlation between true and estimated effect.
Moderate: Moderate confidence in the estimated effect. It is possible that the true effect is very different from the estimated effect.
Low: Limited confidence in the estimated effect. The true effect may be very different from the estimated effect.
Very low: Very little confidence in the estimated effect. The true effect is very probably different from the estimated effect.
No, number of participants in included studies; MD, mean difference; SMD, standardized mean difference; GRADE, Grading of Recommendations Assessment, Development, and Evaluation framework; DoL, days of life; FOF, full oral feeding.
To identify sources of heterogeneity, six prespecified and post hoc subgroup analyses were conducted (Table 2). Subgroups were based on gestational age at birth (<30 weeks and ≥30 weeks), region of medical services (developing, developed), birth weight (<1,500 g and ≥1,500 g), frequency of intervention per day (once, twice, three times), type of CG (standard care, sham), and quality scores (high, low, some concerns).
Subgroup Analysis of Potential Factors and the Oral Motor Stimulation Efficacy Based on Transition Time to Full Oral Feeding
GA, gestational age; MD, mean difference; No, number of included studies.
Among these factors, the region of medical services emerged as the most significant source of heterogeneity, followed by gestational age at birth. The MD index was particularly influenced by the level of medical services. Subgroup analysis revealed that in both developing and developed regions, heterogeneity (I2) was below 50%, indicating that disparities in health care quality accounted for much of the variation observed. In addition, gestational age at birth contributed to variability in outcomes. Infants born at <30 weeks showed greater differences in transition time, but this subgroup included only three studies, limiting statistical power. Further research with larger sample sizes is essential to confirm these results.
Days of life at FOF
Some included studies did not report the transition time from introduction to FOF but reported the outcome of days of life at FOF. Therefore, a post hoc meta-analysis was conducted for this outcome. Eight studies involving 481 infants contributed data. The analysis revealed that infants receiving oral motor stimulation achieved FOF approximately 6 days earlier than those in the CG. Based on the SMD, the effectiveness of this intervention on the outcome of days of life at FOF was medium-grade efficacy.
Days of hospital stay
Sixteen studies, including 781 infants, reported the number of days of hospital stay. Infants in the intervention group had hospital stays that were approximately 6 days shorter than the CG. The effectiveness of intervention on this outcome was of small-grade efficacy.
Weight at FOF and discharge
Seven and ten studies, involving 458 and 481 infants, respectively, reported on weight at FOF and at discharge. The intervention showed a medium-grade efficacy on weight at FOF, but its effect at discharge was inconsiderable.
Milk transfer rate (mL/min)
Two studies involving 214 infants evaluated the milk transfer rate at FOF.30,31 Infants receiving oral motor stimulation demonstrated a milk transfer rate approximately 2.5 mL/min higher than the CG. While the intervention showed medium-grade efficacy, further research with larger sample sizes is required to validate these findings.
Risk of bias in studies
The Cochrane Risk of Bias-2 tool was used to evaluate the included studies (Fig. 1). One trial had a low risk of bias, 32 eight trials had a high risk of bias,7,9,29–31,33–35 and 10 trials28,36–44 raised some concerns. Subgroup analysis showed no significant differences in outcomes based on ROB classification (p = 0.122).
Sensitivity analysis and publication bias
The one-out remove method showed that excluding any single study did not significantly alter the effect size. The greatest variation occurred with the exclusion of the Fucile, Milutinov, Timmons, Dow 35 study. Funnel plots showed no asymmetry, but Egger and Begg tests suggested small study effects (p < 0.1). These findings were not corroborated by the trim-and-fill method, which indicated inconsiderable publication bias.
For sensitivity analysis related to the methodological quality of the included studies, the role of methodological quality on the final conclusion was investigated. The results showed that the MD (95% CI) was −3.33 (−5.82 to −0.84) in studies with low ROB, −6.09 (−7.21 to −4.98) in the high ROB subgroup, and −6.13 (−7.80 to −4.47) in the “some concerns” subgroup. These differences were not statistically significant (p = 0.122).
GRADE
The GRADE framework evaluated the strength of evidence for study outcomes (Table 1). The evidence for the primary outcome, transition time to FOF, was of moderate grade (downgraded 1 point for risk of bias and 1 point for publication bias, and upgraded 1 point for a large effect). The evidence for most secondary outcomes was graded as low or very low (except for days of hospital stay, which was of moderate grade).
Discussion
This systematic review and meta-analysis evaluated the efficacy of the Fucile oral motor stimulation protocol in facilitating FOF among preterm infants. The study focused on the primary outcome of transition time to FOF and secondary outcomes, including duration of hospital stay, days of life at FOF, milk transfer rate, and weight at FOF and discharge. Analyzing 19 clinical trials involving 1,031 preterm infants, the review identified moderate-certainty evidence that the Fucile oral motor stimulation protocol significantly accelerates the transition to FOF by an average of 6 days. The treatment’s effectiveness was rated as medium grade based on SMD. This effect is consistently reflected across individual studies. For example, Fucile et al. 7 reported a transition time of 11.0 days (SD 4.0) in the experimental group (EG) compared with 18.0 days (SD 7.0) in the CG, while Younesian et al. 9 observed 13.2 days (SD 4.31) in the EG versus 26.9 days (SD 4.79) in the CG. Despite these promising results, larger, well-powered studies are needed to improve the certainty of evidence and refine estimates of the effect size.
The intervention also demonstrated a beneficial impact on the secondary outcome of hospital stay duration, reducing it by an average of 6 days compared with controls. Although the effect size is small, the evidence has moderate-certainty, providing moderate confidence in this finding. Specific trial data reinforce this conclusion: Asadollahpour et al. 39 reported a hospital stay of 27.6 days (SD 12.57) in the EG versus 33.45 days (SD 13.46) in the CG, and Rocha et al. 36 documented 41.9 days (SD 17.4) in the EG compared with 52.3 days (SD 19.5) in the CG.
In contrast, the evidence for other secondary outcomes—such as weight at discharge, weight at FOF, and days of life at FOF—remains less robust, with low or very low certainty. For instance, weight at discharge showed minimal impact from the intervention. Bauer et al. 42 reported 2,202 g (SD 265) in the EG versus 2,143 g (SD 290) in the CG, while Khalessi et al. 28 found 2,438 g (SD 165) in EG1 compared with 2,286 g (SD 168) in the CG, yielding a negligible effect size. This lack of significant change may reflect the prioritization of energy expenditure for feeding skill development over weight gain in preterm infants, although the uncertainty in these findings limits definitive conclusions.
Conversely, the milk transfer rate exhibited a moderate improvement with the Fucile protocol, as evidenced by a medium effect size in two studies.30,31 Xiao-Li et al. 30 reported a rate of 10.6 mL/min (SD 5.1) in the EG versus 8.1 mL/min (SD 4.7) in the CG, and Lyu et al. 31 found 10.41 mL/min (SD 4.42) in the EG compared with 8.15 mL/min (SD 4.66) in the CG. Although these results suggest a potential benefit, the limited number of studies precluded a formal assessment of evidence certainty, highlighting a gap that future research must address.
From a clinical perspective, the Fucile oral motor stimulation protocol can be considered a viable intervention to address feeding delays in preterm infants, particularly in settings with established neonatal care resources. The structured and targeted nature of the protocol allows for standardized implementation, which may help mitigate variations in practice and outcomes across different neonatal intensive care units. Policymakers and clinicians could use these findings to develop evidence-based guidelines that integrate oral motor stimulation into routine neonatal care, ensuring consistency and maximizing benefits for this vulnerable population.
Comparison with other studies
Previous systematic reviews have explored various oral motor interventions. Our review, however, focuses exclusively on the Fucile oral motor stimulation protocol for a more precise and targeted analysis. For instance, a Cochrane review 45 analyzed 28 randomized clinical trials, of which only 13 specifically evaluated the Fucile protocol. While the Cochrane review reported reductions in time to FOF (MD: −4.07 days; 95% CI: −4.81 to −3.32; very low certainty) and hospital stay duration (MD: −7.17 days; 95% CI: −8.04 to −6.29; very low certainty), the inclusion of heterogeneous protocols and low-certainty evidence limited the reliability of these findings.
In contrast, our review included six additional studies, encompassing 356 more preterm infants, and utilized a more targeted approach to evaluate the Fucile oral motor stimulation protocol exclusively. This enhanced precision in effect size estimation and increased the certainty of evidence for primary and secondary outcomes, particularly for FOF transition time and hospital stay duration. However, regarding the effectiveness of oral motor stimulation on weight gain at discharge in preterm infants, the effect seems to be inconsiderable (SMD: −0.05 [−0.24 to 0.13]). This may be because these infants, as their energy consumption increases, do not gain weight as rapidly as they develop feeding skills. However, further research is required to confirm this finding, as the current evidence is of very low certainty.
The primary source of uncertainty in our review was the risk of bias. Future studies should address this issue by using higher quality randomized clinical trials to achieve higher certainty of evidence for these outcomes. A 2021 systematic review and meta-analysis by Chen, Yang, Chen, Wang, 17 which included 18 studies with 848 preterm infants, reported that oral motor interventions (any type of oral stimulation) significantly reduced transition time to FOF (MD: −4.61; 95% CI: −5.69 to −3.53) and length of hospital stay (MD: −3.24; 95% CI: −4.60 to −1.87) while improving feeding efficiency and weight gain. However, this review had language limitations and did not use the GRADE framework, limiting the reliability of its findings.
Another 2021 review 46 of seven studies with 507 infants found that oral sensory-motor stimulation improved independent oral feeding in preterm infants (SMD:−2.24; 95% CI: −2.65 to −1.83) and reduced length of hospital stay (SMD: −0.57; 95% CI: −0.93 to −0.22). However, the inclusion of diverse oral stimulation protocols and high heterogeneity, combined with the absence of GRADE framework, precluded definitive conclusions regarding the certainty of evidence.
Another review in 2024 45 with eight randomized clinical trials and 419 infants examined the effects of various oral motor interventions and NNS on oral feeding outcomes in preterm infants. The findings indicated that oral motor interventions significantly reduced transition time to FOF (SMD: −1.186; 95% CI: −2.160 to −0.212) compared with NNS alone. However, there was no significant effect on the length of hospital stay (SMD: −0.346; 95% CI: −0.147 to 0.838). Notably, this study also did not assess the certainty of evidence related to the outcomes.
Subgroup analysis
We conducted prespecified subgroup analyses to explore the effects of oral motor stimulation on transition time to FOF across various factors, including gestational age at birth, level of medical services by region, type of control group, birth weight, intervention frequency, and quality score.
For gestational age, oral motor stimulation showed significantly greater effectiveness in preterm infants born at <30 weeks (SMD: −1.29; 95% CI: −1.74 to −0.84; I2 = 0.0%) compared with those born at ≥30 weeks (SMD: −0.70; 95% CI: −0.89 to −0.52; I2 = 32.1%). This finding suggests that younger, developmentally immature infants benefit more from oral motor stimulation interventions. One possible explanation is that oral motor stimulation addresses the more pronounced feeding challenges in these infants, while those closer to maturity may naturally transition to oral feeding with less external support. However, this conclusion should be interpreted cautiously, as the analyzed data reflect average gestational ages and may not fully account for individual variability.
Interestingly, a review by Chen et al. found no significant differences in transition time between gestational age subgroups (28–30 weeks versus 31–34 weeks). 17 Unlike Chen’s review, which included diverse oral motor stimulation protocols, our study focused exclusively on the standardized Fucile oral motor stimulation protocol, potentially explaining the differences in our findings. This targeted approach may explain the observed greater effectiveness in our subgroup analysis. These results underscore the importance of standardized intervention protocols and subgroup analyses in understanding the nuanced effects of oral motor stimulation in preterm populations, particularly those with varying degrees of developmental immaturity.
In addition, Chen et al. examined the effects of oral motor stimulation based on the level of medical services across different regions. 17 The results indicated that regional differences did not significantly influence the transition time to FOF in preterm infants (p = 0.73). In contrast, our study revealed a notable regional disparity. Oral motor stimulation was more effective in developed countries (SMD: −1.14; 95% CI: −1.86 to −1.02; I2 = 0.0%) compared with developing countries (SMD: −0.66; 95% CI: −0.85 to −0.46; I2 = 23.6%). Based on the 50% law and the heterogeneity test (p = 0.001), the level of medical services by region significantly influenced effect size.
One explanation for this difference is the use of diverse oral motor stimulation protocols in Chen’s review, 17 which may have been implemented with varying levels of precision across regions, diluting the observed effect sizes. In our study, the exclusive focus on the standardized Fucile oral motor stimulation protocol likely reduced variability and highlighted regional disparities.
In addition, the greater efficacy of oral motor stimulation in developed countries may reflect differences in health care systems. Developed countries often provide comprehensive follow-up care and high-resource neonatal services, which can enhance the impact of interventions such as oral motor stimulation. In developing countries, limited access to such resources might reduce the effectiveness of intervention.
While our findings suggest a stronger impact of oral motor stimulation in developed regions, these conclusions require cautious interpretation. Further research is needed to explore the underlying factors contributing to regional differences and to determine how to optimize oral motor stimulation protocols for diverse health care settings.
Similarly, subgroup analysis revealed that preterm infants receiving oral motor stimulation had a significantly reduced transition time to FOF compared with those in the sham intervention group (SMD: −0.89; 95% CI: −1.13 to −0.65), corresponding to a large-grade efficacy. On average, infants in the oral motor stimulation intervention group achieved FOF approximately 7 days earlier than those receiving sham interventions. These findings align with the 2023 Cochrane review, 1 which also reported positive effects of oral stimulation on FOF transition time when compared with standard care and nonoral interventions. The consistency between our results and previous evidence reinforces the clinical relevance of oral motor stimulation.
The implications of these findings are significant for health care policymakers and neonatal care providers. By integrating oral motor stimulation protocols into neonatal intensive care unit practices, particularly as an alternative to sham, outcomes for preterm infants may be substantially improved. Further research should explore the specific mechanisms driving these effects and assess how oral motor stimulation can be optimized within different clinical settings.
The effect of oral motor stimulation on transition time to FOF was examined in two birth weight categories: <1,500 g and ≥1,500 g. Due to the limited number of studies in each subgroup, the classification was simplified, deviating from the originally proposed protocol (2,500 > weight > 1,500; 1,500 > weight > 1,000; and <1,000 g). Despite this analysis, no significant differences were observed between the subgroups.
Similarly, we evaluated the frequency of intervention per day (once, twice, or three times). Only one study involved a three-times-daily protocol, limiting the ability to draw meaningful comparisons. Quality scores were also analyzed as a source of heterogeneity, but no significant impact on outcomes was identified.
Unlike previous reviews, which did not report subgroup analyses based on birth weight, our findings suggest that oral motor stimulation benefits are not strongly influenced by this factor. These results emphasize the need for larger, more detailed studies to assess how birth weight and other variables, such as intervention frequency, might modulate oral motor stimulation effectiveness.
Strengths and limitations
A notable strength of this study is its comprehensive search strategy, which included updated evidence through May 2024. By incorporating six additional studies with 356 more infants compared with the 2023 Cochrane review, 1 this analysis provides more precise effect size estimates and improved evidence certainty.
However, it is crucial to interpret the findings within the context of the study’s limitations. The moderate certainty of evidence highlights the need for caution when generalizing results. Several factors limited the generalizability of these findings, including the exclusion of extremely low birth weight infants, unstable infants, and those with congenital or chronic complications. Methodological concerns, such as small sample sizes and risk of bias in included studies, underline the necessity for further research. Future trials should focus on enhancing methodological rigor, including robust randomization, blinding, and larger, more diverse sample populations. These improvements will not only strengthen the evidence base but also provide clearer guidance for tailoring oral motor stimulation interventions to varied clinical contexts.
In addition, the inability to conduct a dose–response analysis due to limited dosing data underscores the need for future randomized clinical trials exploring different oral motor stimulation intervention frequencies. Such studies should use rigorous design standards, including robust randomization, clear outcome definitions, and larger sample sizes, to enhance the quality of evidence and better inform clinical practices.
Conclusion
This study highlights the potential of the Fucile oral motor stimulation protocol as an evidence-based intervention to accelerate feeding milestones and improve neonatal outcomes for preterm infants. The findings support its integration into clinical practice within neonatal care units to enhance feeding efficiency and reduce hospitalization durations. However, the moderate certainty of evidence and methodological limitations of the included studies emphasize the need for further high-quality research. Future investigations should aim to confirm these findings, explore long-term impacts, and optimize the protocol for diverse clinical settings. By addressing these gaps, neonatal care providers can develop more robust guidelines, ultimately improving outcomes for this vulnerable population.
Footnotes
Authors’ Contributions
Data curation, investigation, visualization, and writing—review and revision were performed by G.G. The first draft of the article was written by M.A. Data curation and investigation were performed by K.B. The first draft of the article was written and revised by F.S. Conceptualization, data curation, formal analysis, investigation, methodology, project administration, supervision, validation, visualization, and writing—original draft were performed by F.A.
AI Disclosure Statement
ChatGPT-4o (Anthropic) was used to assist in improving the article’s readability and language clarity. Specifically, the AI tool provided suggestions for refining sentence structure, grammar, and overall scientific communication. The authors reviewed, validated, and incorporated these suggestions, maintaining full responsibility for the article’s scientific content and interpretations. Potential limitations include the risk of minor contextual misinterpretations, which were carefully scrutinized and corrected by the authors during the editing process.
Confirmation Statement
Each author confirms that the research is supported by an institution primarily involved in education or medical research and that they are not directly supported by the government, in compliance with the journal’s publication requirements.
Disclosure Statement
The authors have no conflicts of interest relevant to this article to disclose.
Funding Information
This systematic review and meta-analysis was supported by Zahedan University of Medical Sciences (grant number 10825, IR.ZAUMS.REC.1402.237) and is registered in PROSPERO (CRD42022369514).