
Abstract
Background:
Due to their nonspecific symptoms, foreign bodies in the aerodigestive tract (FBA) are often misdiagnosed as respiratory conditions, especially when unwitnessed, posing significant risks for morbidity and mortality in the pediatric population.
Case Presentation:
We report a case of an otherwise healthy 4-month-old, predominantly breastfed infant with episodic “honking” breathing, choking with feeds, and a 2-month history of recurrent croup episodes requiring emergency services and an hospital admission. After referral to pediatric otolaryngology/respirology, a flexible laryngoscopy revealed a diagnosis of mild laryngomalacia, inconsistent with the severity of symptoms. A formal airway evaluation was performed, including supraglottoplasty.
Results:
Unexpectedly, extraluminal pulsatile tracheal compression was found, with correlating computed tomography findings of an innominate artery variation and a paraesophageal abnormality. This abnormality appeared as a fluid-filled density between the esophagus and trachea on magnetic resonance imaging, without patency to the esophagus on Upper GI series. Differential diagnoses included vascular malformation, esophageal diverticulum, and bronchogenic/foregut duplication cyst. Although evaluation with echoendoscopy was considered, collaboration with general/thoracic surgery for a flexible esophagoscopy revealed a 2-cm breast pump membrane embedded in a pseudo-diverticulum with a sealed esophageal perforation, which concluded with successful object removal via forceps. The patient’s respiratory symptoms have resolved; however, persistence of the pseudo-diverticulum on follow-up imaging and endoscopy warrants ongoing surveillance.
Conclusion:
This case demonstrates the challenging diagnosis of a breast pump membrane as an unexpected esophageal FBA, compounded by nonspecific respiratory symptoms and the membrane’s near-radiolucency on standard imaging. The exhibited multidisciplinary, collaborative approach was fundamental for the complication-free removal of the membrane.
Introduction
Foreign bodies in the aerodigestive tract (FBA) pose a significant risk of morbidity and mortality in the pediatric population, especially in children less than 3 years of age.1–3 This risk is heightened in younger ages, and aspiration has been shown to be one of the leading causes of incidental deaths in children under 1 year old.3,4 Despite its prevalence, diagnosing FBA in the pediatric population poses a challenge as the inciting event may be unwitnessed, and patients may present with nonspecific clinical symptoms. These symptoms can overlap with respiratory conditions and can include cough, stridor, wheeze, respiratory distress, and dysphagia. Thus, without definitive physical exam findings, patients may have delayed or missed diagnoses.5,6 Other conditions such as asthma, croup, pneumonia, and laryngeal cleft can present with similar symptoms to aspiration events and can therefore make diagnosing pediatric patients challenging.7–9 Not all FBAs are witnessed events, which can further the diagnostic uncertainty. The pediatric population is at increased risk of aspiration and ingestion due to physical development features as well as behavioral characteristics including mouthing, being easily distracted, and crying while eating.10,11 Unwitnessed events are more likely to have delayed presentations due to vague symptoms. 10 When left untreated, chronic FBA increases the risk of several complications including inflammation, erosion of the esophageal wall, esophageal diverticula, and fistulas. 5
The most common types of foreign bodies in the aerodigestive tract show some degree of variability based on country, sociocultural norms, and age. 12 Organic food products are more common in airway foreign bodies (FBs), including peanuts and grains, compared with inorganic products such as coins and toys, which are more frequently involved in esophageal FBs.13–15 Airway FBs are most frequently aspirated in the right main bronchus followed by larynx and trachea. 16 Esophageal FBs are more common than bronchial; however, they usually pass into the stomach. 4 To our knowledge, there are no cases reported of a missed breast pump membrane FB in the proximal esophagus. This case report presents the first delayed diagnosis and treatment of aspirated breast pump membrane causing airway and esophageal complications secondary to prolonged FBA.
Case Report
We report a case of an otherwise healthy, predominantly breastfed 4-month-old male infant presenting with a 2-month history of recurrent croup, intermittent “honking” breathing, and choking with feeds.
Between the ages of 2 and 3 months old, multiple emergency visits were prompted by episodic breathing difficulties and stridor. This entailed at least three serious episodes treated with supportive care and one episode requiring ambulance transfer and community hospital admission due to significant respiratory distress and cyanosis. During each episode, he was diagnosed with croup and responded to intravenous steroid treatment. However, each croup diagnosis was based on honk-like breathing and gasping; however, the typical barking cough was never reported. The hospital admission resulted in inpatient monitoring for 3 days; the patient was once again diagnosed with croup and similarly responded to supportive care. Additionally, at baseline, he would demonstrate intermittent “noisy” breathing and would choke on feeds but nonetheless was objectively gaining weight.
A multidisciplinary outpatient combined airway clinic appointment was arranged at 4 months of age. This involved assessment by both pediatric otolaryngology and respirology to rule out tracheomalacia due to his history of noisy honk-like breathing, significant croup episode history, and choking with feeds. Physical examination revealed this previously cited noisy “honking” breathing and intermittent inspiratory stridor. Nasopharyngolaryngoscopy revealed mild laryngomalacia associated with shortened aryepiglottic folds and normal vocal fold movement bilaterally. Although components of his history were consistent with laryngomalacia, his honking-like breathing and the severity and frequency of croup episodes were not consistent with mild laryngomalacia. Despite the improvement of noisy breathing symptoms with anti-reflux medication, the decision was made to perform a micro-direct laryngoscopy, bronchoscopy, and supraglottoplasty to further assess his airway and rule out any synchronous airway lesions.
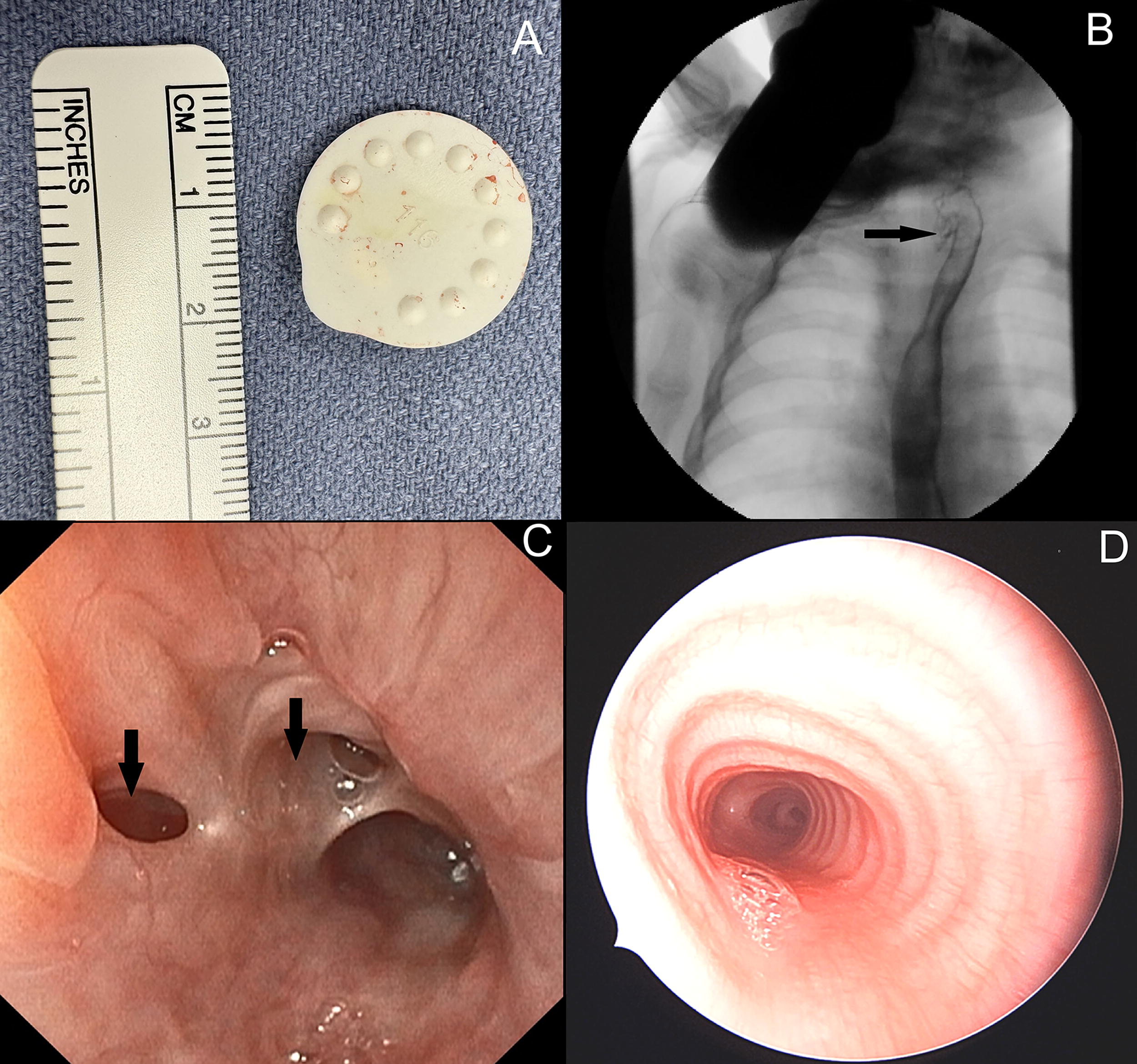
At 5 months of age he underwent formal intraoperative airway evaluation; there was significant anterior–posterior extraluminal compression at the posterior membranous trachea, somewhat pulsatile in nature, distal to the subglottis at the mid-trachea (Fig. 1A). The trachea visualized distal to this narrowing appeared completely normal. Pediatric cardiology consultation and computed tomography (CT) imaging revealed an innominate artery variation with a slightly leftward origin, as well as a paraesophageal soft tissue abnormality adjacent to the redemonstrated mid-tracheal luminal narrowing (Fig. 1B) characterized as a linear high attenuating structure. The concurrent innominate artery variation and the lack of feeding vessels associated with paraesophageal abnormality necessitated additional investigations. Magnetic resonance imaging (MRI) redemonstrated the soft tissue abnormality along with surrounding fluid, extending from the anterior esophagus, interposed between the esophagus and trachea, and deviating the trachea rightward due to mass effect. An upper gastrointestinal (GI) contrast study demonstrated a fluid-filled structure suggestive of an esophageal diverticulum; however, it lacked communication with the esophagus. He continued to have episodes of difficulty breathing and honking-like breathing. An echoendoscopy was considered and the decision to return to the operating room was made in collaboration with pediatric general surgery and thoracic surgery, for a flexible esophagoscopy and a repeat micro-direct laryngoscopy and bronchoscopy.

At 6 months of age, repeat micro-laryngoscopy and bronchoscopy showed significant tracheomalacia with near total collapse and narrowing at the mid-trachea. Flexible esophagoscopy revealed a very soft plastic circle that was found in the upper esophagus, at 12 cm from the incisors (Fig. 1C, D), corresponding to the trachea mass effect. The FB was lodged within a sealed esophageal perforation surrounded by chronically inflamed mucosa, compatible with pseudo-diverticulum. The object was easily removed using forceps through the working channel of the flexible esophagoscope, without any associated bleeding or perforation. After removal, the FB was measured to be approximately 2 cm in diameter and deemed to be a breast pump membrane (Fig. 2A). Following this FB removal, the patient’s symptoms resolved. Three repeat upper GI studies redemonstrated this pseudo-diverticulum with each assessment (Fig. 2B), warranting a liquid diet of breast milk and iron-fortified formula, and ongoing monitoring for stricture.
At 8 months of age, the pseudo-diverticulum remained, and his diet was advanced to purees. At 1 year old, on repeat esophagoscopy and direct laryngoscopy–bronchoscopy, the pseudodiverticulum appears to be starting to heal and did not have debris lodged within it (Fig. 2C), and the tracheal wall no longer appeared narrowed respectively (Fig. 2D). The team is hopeful for its independent resolution with plans for reassessment at 18 months of age. Endoscopic management of an eventual symptomatic residual pseudo-diverticulum may be considered once the child is older.
Discussion
This case illustrates the diagnostic challenges of FBA in infants, particularly when presentation is delayed, as symptoms are nonspecific. The patient’s age of presentation (4 months old) made FBA an unlikely initial consideration, as infants in this age-group typically lack the fine and gross motor skills required to grasp, mouth, and swallow foreign objects. The clinical symptoms of recurrent noisy and sometimes honking-like breathing, and choking during feeds, complicated matters as these overlapped with other conditions such as laryngomalacia, croup, and gastroesophageal reflux. Recognizing inconsistencies between clinical history and physical findings (i.e., mild laryngomalacia not aligning with the recurrent severe croup presentation) was pivotal in identifying the need for further evaluation. Subsequent micro-laryngoscopy and bronchoscopy revealed tracheomalacia and extraluminal compression of the mid-trachea, prompting further imaging studies and expanding the differential. CT and MRI findings of a paraesophageal abnormality provided a clearer understanding, although the exact nature of the mass remained elusive. The differential diagnosis included vascular malformation, esophageal diverticulum, and bronchogenic or foregut duplication cyst. An innominate artery variation provided potential explanation for the pulsatile nature of the compression, particularly when the differential narrowed towards esophageal diverticulum, with the demonstration of a fluid-filled structure on upper gastrointestinal series. Colleagues in radiology were essential for the objective assessment of the paraesophageal abnormality’s unclear structure through multiple modalities, and colleagues in pediatric general surgery and thoracic surgery provided additional multidisciplinary diagnostic considerations and operative planning, which included considering echoendoscopy. Only a second procedure that added an esophagoscopy revealed the unexpected culprit: a breast pump membrane embedded in a pseudo-diverticulum in the esophagus. It was hypothesized that the object had caused chronic irritation leading to adjacent esophageal inflammation and the formation of a sealed pseudo-diverticulum. In contrast to the challenging diagnostic pathway, the retrieval of the object was uneventful, as it was easily removed during the same procedure without any complications. Fortunately, this early diagnosis and endoscopic removal prevented progression to benign acquired tracheoesophageal fistula, which would likely have required surgical management. The patient continues to be monitored for hopeful resolution of the pseudo-diverticulum and is on a normal diet. Further endoscopic intervention for a persistent pseudo-diverticulum may be indicated once the child is older.
Conclusion
This case of a 4-month-old infant with 2 months of noisy breathing illustrates the challenging diagnostic process of FBAs, particularly in the delayed setting and infant age, and the unique finding of a breast pump membrane as a foreign body. The patient had a reasonably decreased propensity for FBA risk due to presenting age and a lack of FBA events on history. Although nonspecific respiratory symptoms could be explained by findings of mild laryngomalacia on nasopharyngolaryngoscopy, this did not align with the exceptional history of severe recurrent croup-like episodes. Micro-laryngoscopy and bronchoscopy were essential for revealing an unexpected mid-tracheal compression, identified to be mass effect from a paraesophageal abnormality on medical imaging. A multidisciplinary collaborative approach was therefore essential in the differential diagnosis expansion and return to the operating room for esophagoscopy to remove this uncommon foreign body without any complications. The breast pump membrane was near radiolucent on standard imaging, and as a distal component of the pump apparatus, it was previously thought to be an unlikely foreign object for ingestion. Therefore, this case shares insight to the effective management of a delayed, unwitnessed FBA case and highlights the potential danger of breast pump membrane as a foreign body. It underscores the need for heightened clinical suspicion and a thorough, multidisciplinary approach in evaluating infants with persistent respiratory symptoms and atypical histories. It also highlights the potential hazards of breast pump components as foreign bodies, advocating for increased awareness and prevention efforts.
Footnotes
Acknowledgments
The authors thank the patient and their family for their permission to publish this case report, as well as all the providers involved in their care.
Authors’ Contributions
O.G.: Contributions to writing article, figure assembly, and formatting. G.P.: Contributions to literature review, references, and writing article. J.L.: Contributions to article writing. M.Q.: Contributions to article writing. T.M.: Contributions to article writing. S.M.: Contributions to article writing. I.R.: Contributions to article writing. J.S.: Contributions to article writing.
Patient Consent
Guardians of the patient served as Substitute Decision Makers for the care of the patient based on age and thus consented on behalf of the patient for the publication of their case for the purpose of education and research.
Author Disclosure Statement
All the authors have no interests to disclose.
Funding Information
There are no applicable sources of funding.