
Abstract
Background:
Mothers delivering preterm are very often exposed to antibiotics in the peripartum period. We hypothesize this may select bacteria bearing antibiotic resistance genes (ARGs) in the breast milk and be transmitted to the neonate’s mouth while feeding. This study aimed to determine the prevalence of ARGs coding for extended-spectrum beta-lactamases (ESBLs) (including AmpC beta-lactamases [ACBLs]) and carbapenemases in breast milk and neonatal oral swab samples of preterm mother–infant pairs, the concordance of ARGs between paired samples, and risk factors of ARGs coding for ESBLs and carbapenemases.
Methods:
Breast milk and oral swab samples were obtained aseptically from 100 preterm mother–infant pairs (gestation 28–34 weeks) by postpartum day 10. Multiplex PCR was used to detect 15 common ARGs in these samples. Potential risk factors of the presence of any ARG coding for ESBLs or carbapenemases in breast milk and oral swab samples were studied.
Results:
The commonest ARGs for ESBLs, ACBLs, and carbapenemases in breast milk were blaSHV (28%), blaCIT (33%), and blaIMP (49%), respectively; and oral swabs blaCTX-M1 (30%), blaCIT (58%), and blaIMP (24%), respectively. ARGs common to breast milk and oral swabs included blaCIT (13%), blaIMP (10%), blaCTX-M-1 (9%), and blaSHV (6%). Formula milk intake was associated with less oral carbapenemase ARGs.
Conclusion:
ARGs for ESBLs and carbapenemases are highly prevalent in preterm breast milk and oral swabs.
Introduction
Antimicrobial resistance (AMR) seriously threatens neonatal survival, especially in developing countries, where antibiotics are often overused. 1 Worldwide, AMR is responsible for ∼214,000 newborn deaths annually. 2
In low- and middle-income countries (LMICs), multidrug-resistant (MDR) gram-negative neonatal sepsis is largely attributed to extended-spectrum beta-lactamase (ESBL)-producing and carbapenem-resistant Enterobacterales.3,4 ESBLs hydrolyze third- and fourth-generation cephalosporins and monobactams, but not carbapenems, and are inhibited by beta-lactamase inhibitors (BLIs). 5 AmpC beta-lactamases (ACBLs) are cephalosporinases resistant to BLIs, but cannot hydrolyze certain fourth-generation cephalosporins. 6 Carbapenemases inactivate all β-lactam antibiotics. 7
A resistome may be established postnatally in the infant gut even before any exposure to antibiotics.8,9 Although antibiotic resistance genes (ARGs) are reported in neonatal oral and fecal samples during the first week, their source is still unclear.10,11 The early acquisition of a neonatal gut resistome is of concern because it may increase the risk of subsequent MDR infections. 12
The breast milk microbiome establishes the oral and gut microbiota among breastfed infants.13,14 It has been shown that antibiotic usage in pregnancy is associated with more ARGs in maternal and neonatal fecal samples.15,16 Several studies have reported the culture-based prevalence of MDR bacteria in breast milk, highlighting the potential risks of vertical transmission, particularly in vulnerable neonates. 17 In our study conducted at a tertiary care hospital (PGIMER), we enrolled 100 preterm mother–neonate dyads. From the breast milk of 14 mothers, 14 pathogens of interest were isolated, 9 of which (64%) were identified as MDR. Oral swabs from 77 neonates grew 82 isolates, with 70.7% being MDR. Rectal swabs from 96 neonates grew 130 isolates, of which 80% were MDR. 18
To the best of our knowledge, only two studies (both on full-term mothers) have demonstrated ARGs in breast milk and shown the similarity of some of these ARGs with those in the infant’s gut.19,20 Data from these studies suggest that ingesting breast milk containing ARGs may be a pathway by which neonates acquire ARGs early in postnatal life. To date, there are no studies on ARGs in the breast milk of mothers delivering preterm nor are there any studies exploring the concordance of ARGs in breast milk and the neonate’s mouth. Compared with term mothers, preterm mothers have far greater exposure to broad-spectrum antibiotics because intrapartum antibiotic prophylaxis is often administered to them. 21 It is not known whether this antibiotic selection pressure results in a greater abundance of ARGs in preterm breast milk.
In view of the above gaps in knowledge, we conducted a study on the prevalence of common ARGs (coding for ESBLs, ACBLs, and carbapenemases) in preterm breast milk and the oral swabs of their neonates, the concordance of ARGs among paired samples, and the risk factors associated with these ARGs.
Materials and Methods
Study design
A prospective cohort study was conducted in the Neonatology Unit and Obstetrics Department of a tertiary care hospital. Preterm mother–infant pairs (gestation 28–34 weeks) were enrolled at ≤10 days postnatal age if the neonate was fed mother’s milk. Mothers delivering after 34 weeks were excluded as they are likely to be discharged early and have low antibiotic exposure rates. Mothers delivering at <28 weeks were excluded because extremely preterm mothers do not have enough surplus milk that can be spared for research. Mother–infant pairs were excluded if the infant had gastrointestinal surgical conditions, life-threatening illnesses, or if the mother had mastitis or breast infections.
The empirical intrapartum antibiotic policy at our center involves administering ampicillin or amoxicillin to mothers at risk of early-onset neonatal sepsis, with cefazolin and vancomycin as alternatives. For cesarean sections, cefazolin is given 30 minutes preoperatively, with cefuroxime and clindamycin as alternatives. For suspected neonatal sepsis, the empirical first-line antibiotics are ciprofloxacin and amikacin; and the empirical second-line antibiotic is meropenem.
A convenience sample of 100 pairs was recruited. All experimental protocols were approved by the Institutional Ethics Committee of PGIMER, Chandigarh, India. The Institutional Ethics Committee approved the study (PGI/IEC/2018/00002, dated 12 January 2018), adhering to the ethical principles outlined in the 1964 Declaration of Helsinki and the subsequent amendments. Written informed consent was obtained from all participants.
Demographic variables
Data collected included maternal age, parity, comorbidities, perinatal antibiotic exposure, mode of delivery, neonatal sex, type and volume of milk feeds, neonatal antibiotic exposure, and age at initiation of feeding.
Milk sample collection
Breast milk was collected by research staff using stringent aseptic techniques an hour before a scheduled feed. The areola and surrounding skin were swabbed with a sterile saline-soaked swab to culture resident flora by standard methods and then cleaned with 2% chlorhexidine before repeating the skin swab culture. After discarding 2 mL of foremilk, 10–15 mL of milk was collected into an autoclaved, nuclease-free Falcon tube and transported via cold chain to the laboratory. To minimize contamination, self-expressed or stored milk was avoided, and donor milk was not used.
Milk sample processing
Samples were centrifuged at 2,250 g to remove the fat layer and recentrifuged at 230,000 g for 10 minutes. The pellet was resuspended in 1,000 µL sterile saline, transferred to an autoclaved, nuclease-free tube, and stored at –80°C, adhering to standard precautions in a BSL-2 facility.
Neonatal oral swab collection
At enrollment, sterile cotton swabs were used to swab the mouth, immersed in 500 µL sterile saline, vortexed, and stored at –80°C for DNA extraction.
Bacterial DNA isolation and multiplex PCR
Bacterial DNA was isolated using Qiagen DNA mini kits. DNA concentration and purity were assessed using a Nanodrop spectrophotometer and agarose gel electrophoresis. Multiplex PCR (BIORAD, T100 Thermal cycler, USA), targeting 15 ARGs organized into four panels, was performed to detect common ARGs known to be associated with ESBLs, ACBLs, and carbapenemases (Supplementary Table S1). 22 Multiplex PCR is a molecular technique that uses multiple sets of primers, allowing simultaneous amplification of multiple target DNA sequences in a single reaction, saving time and resources. This method is widely used in clinical diagnostics, genetic testing, and pathogen detection due to its high efficiency and ability to generate comprehensive results from minimal sample input. The PCR protocol was optimized using known ARG-producing strains as controls. Amplified products were analyzed by gel electrophoresis, using 50 bp and 100 bp DNA ladders as markers.
Risk factor analysis
Patients were grouped into “no detectable ESBL-coding ARGs” and “at least one ESBL-coding ARG” in the breast milk samples. Similarly, they were grouped into “no detectable carbapenemase-coding ARGs” and “at least one carbapenemase-coding ARG” in the breast milk. These groups were compared for the following potential risk factors: gestational age, maternal diet, multiple pregnancies, prolonged rupture of membranes (PROM), preterm PROM (pPROM), and maternal antibiotic exposure in the preceding 3 months. For neonatal oral swabs, the patients were grouped in the same manner as for the breast milk samples, and these groups were compared for neonatal antibiotic use, feeding type and route, and age at initiation of feeding, along with the above maternal risk factors.
Statistical Analysis
Data were analyzed using SPSS v22. Categorical variables were summarized as frequencies and percentages, while numerical variables were expressed as mean (standard deviation) or median (interquartile range), depending on distribution normality assessed by the Shapiro–Wilk test. Group comparisons used chi-square or Fisher’s exact tests for categorical data, and Student’s t test or Mann–Whitney U test for numerical data. Effect sizes were reported as mean differences with 95% confidence intervals (CIs) for continuous variables and odds ratios (95% CI) for categorical variables.
Results
Of 130 screened pairs, 100 were enrolled. Preterm mothers with inadequate lactation (n = 9), anticipated early discharge (n = 14), maternal mastitis (n = 1), life-threatening neonatal illness (n = 1), and who did not give consent (n = 5) were excluded. The demographic data of the study participants are summarized in Table 1. Figure 1A–D displays the representative gel electrophoresis results for ARGs.
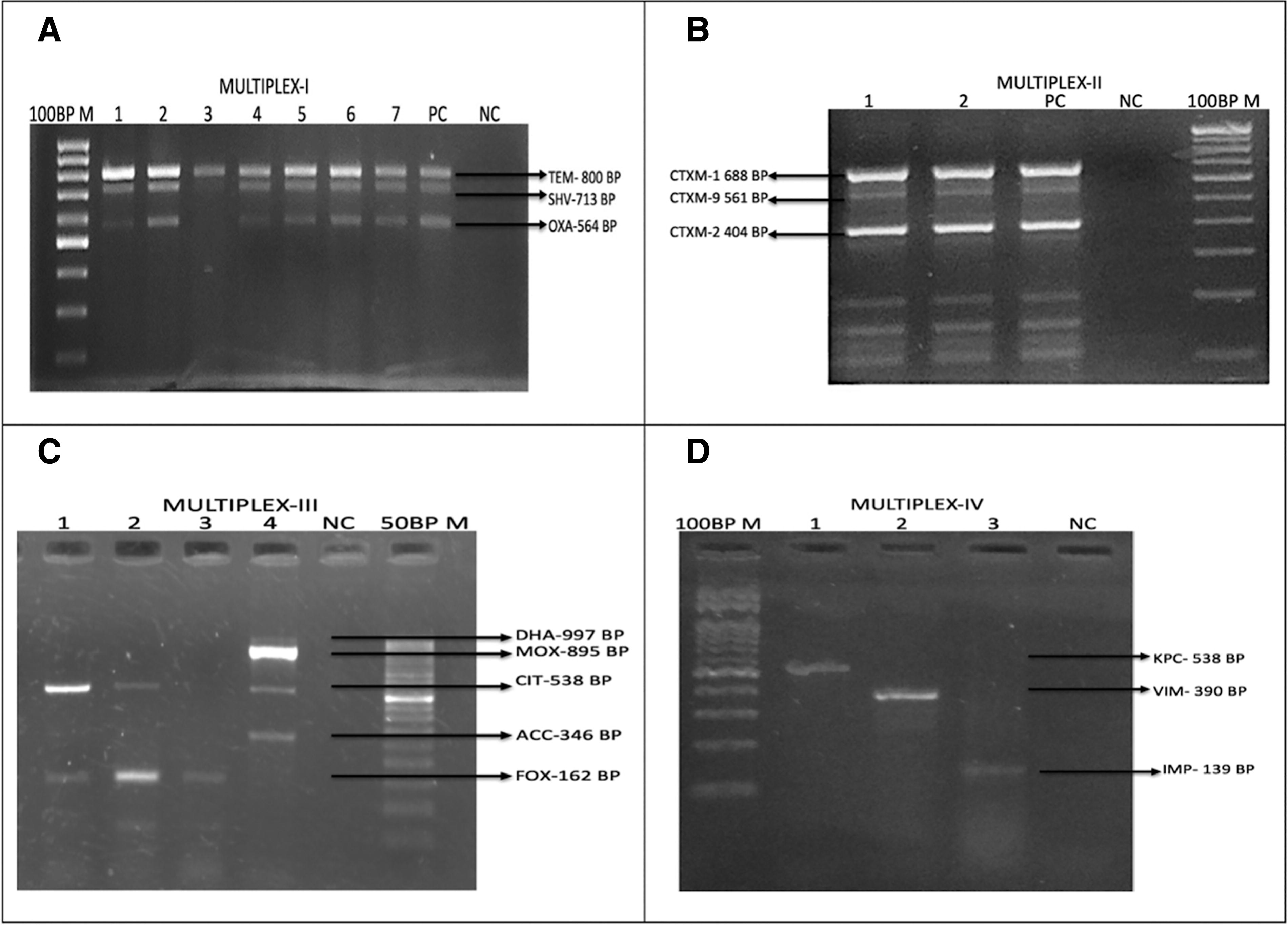
Representative gel electrophoresis pictures of the multiplex PCR assays.
Demographic and Clinical Details of the Enrolled Mothers and Their Neonates
Figures are n (%) unless specified otherwise.
EOS, early-onset sepsis; LOS, late-onset sepsis; HIE, hypoxic ischemic encephalopathy; HT, hypertension; NNJ, neonatal jaundice; pPROM, preterm PROM; PROM, premature rupture of membranes; RDS, respiratory distress syndrome; SD, standard deviation.
In breast milk samples, the commonest ESBL-related ARGs were blaSHV (28%), blaTEM (24%), blaCTX-M-1 (24%), and blaOXA-1 (22%) (Supplementary Table S2). Among AmpC beta-lactamases, blaCIT and blaFOX were each detected in 33% of samples. Carbapenemase-related ARGs had varying prevalence as follows: blaIMP (49%), blaVIM (15%), and blaKPC (3%). In oral swab samples, blaCTX-M-1 (30%), blaTEM (23%), blaSHV (13%), and blaOXA-1 (5%) were the commonest ESBL-related ARGs, while blaCIT (58%) was the commonest AmpC gene. blaIMP was detected in 24% of samples, whereas blaVIM and blaKPC were less frequent.
Eleven percent of samples had all three ARGs of Panel I. Two percent of samples had all three ARGs of Panel II. Nineteen percent of samples possessed both the blaFOX and blaCIT ARGs. One sample contained four blaAmpC ARGs (blaFOX, blaMOX, blaCIT, and blaEBC). Two percent of breast milk samples had all three ARGs of Panel IV. The oral swab from one neonate had all three ARGs of Panel I.
ESBL-coding ARGs common to paired breast milk and oral swab samples included blaCTX-M-1 (9%), blaSHV (6%), blaTEM (2%), blaOXA-1 (1%), and blaCTX-M-2 (1%). Among AmpC beta-lactamases, blaCIT was found in 13% mother–neonate pairs. Regarding carbapenemase-coding ARGs, 10% of pairs had blaIMP, and 1% each had blaKPC and blaVIM.
Seventy-one percent of breast milk samples had at least one ARG coding for ESBLs, including AmpC ESBLs (Table 2). The mothers without any detectable ESBL-coding ARG in their breast milk exhibited a significantly higher prevalence of pPROM (83%) compared with those with at least one ESBL-coding ARG (59%) (p = 0.02). No other maternal or clinical variables, including maternal age, delivery mode, antibiotic usage, or feeding practices, showed any statistically significant association with ESBL-coding ARGs in breast milk. At least one ARG encoding carbapenemases was detected in 50% of the milk samples (Table 2). No statistically significant associations were found between any of the factors and the presence of carbapenemase-coding ARGs. There was no association between breast milk ARGs coding for ESBLs or carbapenemases and neonatal culture-positive sepsis or in-hospital mortality.
Antibiotic Resistance Genes Coding for Extended-Spectrum Beta-Lactamases and Carbapenemases in Milk Samples and Association with Risk Factors
Figures are n (%) unless specified otherwise.
p Values <0.05 are in bold.
ARGs, antibiotic resistance genes; ESBLs, extended-spectrum beta-lactamases; CI, confidence interval; SD, standard deviation; PROM, premature rupture of membranes; pPROM, preterm PROM.
Eighty-four percent of oral swab samples had at least one ESBL-coding ARG (including AmpC ESBLs) and 27% of oral swab samples had at least one carbapenemase-coding ARG (Table 3). Formula milk intake was inversely associated with carbapenemase-coding oral ARGs (p = 0.0001). No association was found between the presence of these ARGs and any other potential risk factors (Table 3).
Antibiotic Resistance Genes Coding for Extended-Spectrum Beta-Lactamases and Carbapenemases in the Oral Swab Samples and Their Association with Risk Factors
Figures are n (%) unless specified otherwise.
p Values <0.05 are in bold.
ARGs, antibiotic resistance genes; ESBLs, extended-spectrum beta-lactamases; CI, confidence interval; SD, standard deviation; PROM, premature rupture of membranes; pPROM, preterm PROM; OG, orogastric.
Discussion
Overall, there were high carriage rates of ARGs coding for ESBLs and carbapenemases in the breast milk of preterm mothers and their neonatal oral swabs, with concordance between breast milk and oral swab samples ranging between 1% and 13%. To the best of our knowledge, there are only two previous studies demonstrating the presence of ARGs in breast milk and both are limited to mothers delivering at term gestation.19,20 Using a whole metagenomic approach, Parnanen et al. studied ARGs in breast milk, maternal fecal, and infant fecal samples in 16 mother–infant pairs. 19 ARGs for tetracycline resistance were the most common among maternal fecal samples and for colistin resistance among infant fecal samples. While the authors provided individual patient data, they did not report the frequencies of specific ARGs in breast milk, making comparison with our data difficult.
Zhang et al. cultured only Staphylococcus epidermidis from fecal samples of full-term exclusively breastfed cesarian-born neonates and colostrum samples of their mothers. 20 On amplifying ARGs targeting S. epidermidis in 82 sample pairs, they found ARGs in 85% colostrum samples, including blaTEM and AmpC in 24% and 16% samples, respectively. The method that Zhang et al. used to clean the nipple and surrounding skin (normal saline cotton swab followed by wiping the nipple with a soapy towel) raises concerns about contamination with skin flora, especially since their study was limited to S. epidermidis.
Two research groups had cultured drug-resistant bacteria grown from breast milk of healthy mothers in the first year after birth. Huang et al. found significant resistance to nine clinically relevant antibiotics in milk samples from 30 healthy mothers. 23 Chen et al. cultured milk from 19 healthy women and identified 20 species, including commensal and pathogenic bacteria. Staphylococcus, Streptococcus, and Enterococcus isolates were found MDR, with some strains resistant to vancomycin. 24
Two research groups have reported neonatal oral ARGs. Among 108 neonates, Klassert et al. reported blaSHV in 8.3% oral swab samples, compared with 13% in our study, and blaCTX-M-1 in 8.3% samples, substantially lower than the 30% observed by us. 25 Gomez-arango et al. screened oral swab samples of 36 neonates for five ARGs and reported blaVIM in 16%. 11 There is scant published data on the concordance of ARGs in breast milk and neonatal oral swab samples. In our study, the highest concordance was for the blaCIT and blaIMP ARGs. Parnanen reported that 70% of the ARGs found in breast milk overlapped with ARGs in the infant’s gut. 19 They suggested that some of the shared ARGs may be attributed to direct transportation to the gut through breastfeeding. By multilocus sequence typing, Zhang et al. showed that 63% pairs of S. epidermidis isolates were homologous, suggesting that ARGs in the neonatal feces were mainly derived from maternal colostrum. 20
To the best of our knowledge, there are no previous studies that evaluated maternal and neonatal risk factors of ESBL- and carbapenemase-coding ARGs in the breast milk and the mouth. In our study, mothers with ESBL-related ARGs in breast milk had a lower incidence of pPROM (p = 0.02). This appears to be counterintuitive because one would expect that mothers with pPROM have greater exposure to beta-lactam antibiotics and hence to be at greater risk of harboring ESBL-related ARGs. Our finding of a lower incidence of pPROM may be a chance association, but a possible explanation could be that administering antibiotics for pPROM decreases the overall bacterial load in breast milk, including those with ESBL-related ARGs. Moreover, the presence of an ARG does not necessarily mean that the gene is being expressed. Likewise, Ji et al. found that the neonates of mothers who were treated with antibiotics (indications were not mentioned) had lower abundances of blaOXA10, blaSHV, cfxA, tnpA-04, and tnti1 in fecal samples. 15
Carbapenemase-related ARGs were more prevalent in the oral swabs of breastfed neonates compared with those fed with formula milk (p = 0.0001). Since formula milk does not contain breast milk-associated bacteria, it decreases the exposure to ARGs. A similar (although insignificant) trend was seen with ESBL-related ARGs (p = 0.1). It is important to emphasize that this study does not aim to promote formula feeding over breastfeeding. Breastfeeding is widely recognized for its numerous health benefits and remains the recommended mode of infant feeding. Our study suggests the potential dangers of unrestricted antibiotic usage in mothers during pregnancy and lactation. The detected ARGs may reflect the natural diversity of the breast milk microbiome, which includes nonpathogenic bacteria. Further studies are needed to understand the clinical relevance of these findings. On the contrary, Parnanen et al. showed that the ARGs were more abundant in the guts of formula-fed infants compared with exclusively human milk-fed infants. 26
A limitation of our study was the lack of a control group of term, healthy mothers to directly compare preterm versus term mother–infant pairs. Recruiting postnatal age-matched healthy, term mothers is difficult as they are discharged early and often reluctant to revisit the hospital within days of discharge just to donate a milk sample for research purposes. We could not compare our data with previous studies on ARGs in term breast milk because one study lacked information about frequencies of ARGs 19 and one was limited to S. epidermidis. 20 Moreover, our study was conducted in a region where there is a high burden of AMR and MDR neonatal sepsis,27–29 and our results may not be generalizable to centers with less AMR. There are no studies on ARGs in breast milk from other LMICs, where there is a similar burden of MDR colonization and sepsis as ours. Including maternal and neonatal fecal samples would have provided a more complete picture of the source and pathway for transferring ARGs.
From this study and previous data, we cannot directly conclude that ARGs in breast milk and oral swab samples play a role in MDR neonatal sepsis. However, circumstantial evidence suggests that this may be a contributory factor. In a substudy of the BARNARDS study, ARGs in the mothers’ guts were associated with ARGs in their neonates’ guts and with sepsis in their neonates. 16 Antibiotic usage in pregnancy is associated with ARGs in maternal and neonatal fecal samples. Hence, we speculate that antibiotic overuse by adult women may contribute to ARGs in breast milk, and the acquisition of a gut resistome by newborn infants, which could contribute to MDR neonatal sepsis.
Although the transfer of ARGs via breast milk likely explains the concordance of ARGs between breast milk and the neonatal oral cavity, we cannot be sure that this is the only explanation since environmental bacteria can also colonize the mouth. Moreover, very preterm infants may have never been directly breastfed before oral sampling. Among them, breast milk bacteria bearing ARGs may have colonized the mouth via non-nutritive sucking (universally practiced in our unit), gastroesophageal reflux, or by “contaminating” the mouth during the process of gavage feeding.
Conclusions
In conclusion, our study highlights the prevalence and concordance of common ESBL- and carbapenemase-related ARGs in preterm milk and neonatal oral samples. Unexpectedly, the presence of ESBL-coding ARGs in breast milk was inversely associated with pPROM. This association could be due to chance or a reduction in the overall bacterial load due to antibiotic exposure. Larger studies are needed to validate this finding. No significant associations were observed between maternal or perinatal factors and the presence of carbapenemase-coding ARGs in breast milk. Breast milk feeding compared with formula milk was associated with carbapenemase-coding ARGs in oral swabs, possibly because breast milk has a microbiome that can harbor ARGs. Overall, our study shows the widespread occurrence of ARGs in maternal and neonatal samples and emphasizes the need to restrict the use of antibiotics in mothers and their infants.
Footnotes
Authors’ Contributions
S.D. and A.S. contributed to the design of the work, acquisition, analysis, and interpretation of the data, drafted the first version of the article and reviewed it critically, wrote the final version of the article to be published, and agreed to be accountable for all aspects of the work. M.B. contributed to the conception and design of the work, acquisition of data, reviewed the draft articles for important intellectual content, approved the final version to be published, and agreed to be accountable for all aspects of the work. A.C. contributed to the design of the work, the acquisition and analysis of data, reviewed the draft articles for important intellectual content, approved the final version to be published, and agreed to be accountable for all aspects of the work.
Data Availability
The dataset of the study is not currently publicly available but will be provided by the corresponding author on reasonable request made by email.
Disclosure Statement
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding Information
The study was funded jointly by the Indian Council of Medical Education and Research (ICMR) and the Department of Biotechnology (DBT), Government of India. This work was supported by the Indian Council of Medical Research, grant no. 5/7/1593/2017-RBMH&CH and the Department of Biotechnology, grant no. BT/DBT-ICMR/JWG/02/2018, Government of India.