
Abstract
Scientific studies in oncology, cancer diagnosis, and monitoring tumor response to therapeutics currently rely on a growing number of clinico-pathological information. These often include molecular analyses. The quality of these analyses depends on both pre-analytical and analytical information and often includes the extraction of DNA and/or RNA from human tissues and cells. The quality and quantity of obtained nucleic acids are of utmost importance. The use of automated techniques presents several advantages over manual techniques, such as reducing technical time and thus cost, and facilitating standardization. The purpose of this study was to validate an automated technique for RNA extraction from cells of patients treated for various malignant blood diseases. A well-established manual technique was compared to an automated technique, in order to extract RNA from blood samples drawn for the molecular diagnosis of a variety of leukemic diseases or monitoring of minimal residual disease. The quality of the RNA was evaluated by real-time quantitative RT-PCR (RQ-PCR) analyses of the Abelson gene transcript. The results show that both techniques produce RNA with comparable quality and quantity, thus suggesting that an automated technique can be substituted for the reference and manual technique used in the daily routine of a molecular pathology laboratory involved in minimal residual disease monitoring. Increased costs of reagents and disposables used for automated techniques can be compensated by a decrease in human resource.
Introduction
N
Materials and Methods
Study design and clinical samples
In order to compare the automated and manual techniques, 25 blood samples were obtained after informed consent from patients with a variety of malignant blood disorders (Table 1). Twenty milliliters of blood was collected in EDTA for each patient, either for diagnosis or for monitoring response to treatment (monitoring of minimal residual disease, MRD) during follow-up.
C
Acute leukemias are classified according to the FAB (French American British) classification (M0 through M7).
Abbreviations: ALL, acute lymphoblastic leukemia; AML, acute myeloblastic leukemia; CML, chronic myelogenous leukemia; MPD, myeloproliferative disease.
On the same day, cell processing before RNA extraction was performed at the biological resource center, according to institutional standard operating procedures. RNA was sequentially extracted from aliquoted processed blood samples with the manual and the automated techniques, the latter being systematically done within a longer delay than the former.
Sample processing prior to RNA extraction
Analyses were performed from mononuclear cells. Each freshly collected blood sample was loaded on a density gradient (Ficoll/Lymphoprep, Absys, France), and centrifuged at 600g for 10 min at room temperature. Mononuclear cells were recovered and washed in RPMI. Aliquots of 15 × 106 cells were prepared and maintained in conservation buffer (RNA Protect Cell Reagent®, Qiagen, France) at 4°C in a monitored refrigerator for immediate stabilization of RNA before extraction; RNA extraction was performed within a maximal delay of 1 month, as recommended by the manufacturer.
Manual RNA extraction
The RNeasy Mini Kit® (Qiagen, Germany) was used for RNA extraction. First, the RNA Protect Cell Reagent was removed by centrifugation (5,000g/10 min/room temperature). Biological samples were then lysed and homogenized in the presence of a highly denaturing guanidine-thiocyanate-containing buffer (RLT), mixed with β-2-mercaptoethanol. RNA extractions were performed according to the manufacturer's recommendations. Ethanol was added to provide appropriate binding conditions, and samples were applied to an RNeasy Mini column; RNAs longer than 200 bases bind to the RNeasy silica membrane, thus producing a relative enrichment for mRNAs, since most RNAs <200 nucleotides (such as 5.8S rRNA, 5S rRNA, and tRNAs, which together comprise 15%–20% of total RNA) are selectively excluded. At the final step, RNA was eluted in 40 µL of RNase-free water.
Automated RNA extraction
Cell processing and elution volume were similar to the manual technique. Manufacturer's recommendations indicate that β-2-mercaptoethanol is dispensable for RNA extraction; thus, 18 of the 25 samples were extracted without β-2-mercaptoethanol. Automated extractions were performed on the QIAcube device (Qiagen, France), as programmed.
RNA concentration
RNAs were originally recovered under 40 µL, with the manual and automated procedures, and further concentrated using the 5301 Concentrator (Eppendorf, Waterbury, CT). This device was previously validated for its ability to improve RNA concentration without deteriorating the quality of subsequent RQ-PCR analyses.1 RNAs were eluted in a final volume of 15 µL of RNase-free water.
RNA analyses
RNA concentration was measured by spectrophotometry, using the Nanodrop ND-1000 apparatus (Labtech, France), with 1.5 µL of sample. Measures were done in duplicate; absolute quantities of isolated RNA were calculated from the average measured concentrations, as shown in Figure 1. RNA quality was assessed by real-time quantitative RT-PCR (RQ-PCR), using a standard protocol with the Taqman 7900® device (Applied Biosystems, Foster City, CA), and in accordance with international recommendations.2 For each sample, the Abelson transcript (ABL)—together with a positive internal control—was amplified. Experiments were performed in duplicate, and the median cycle threshold (Ctm) value was calculated.
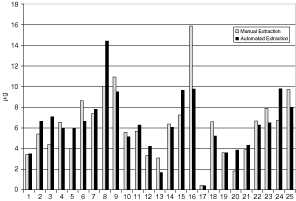
RNA quantity isolated from samples 1 through 25. Each bar represents the average value for each duplicate. P = 0.85 using a Wilcoxon test for paired samples.
Statistics
Wilcoxon nonparametric tests for paired values were used to compare results measured in parallel with RNA samples isolated from the same original cell samples, using either the manual or automated techniques described above. Differences were considered nonsignificant for P values >0.05.
Results and Discussion
After manual and automated extractions were completed, RNAs were immediately quantified using a spectrophotometer. At first, concentrations and absolute quantities of RNAs obtained from identical biological samples were compared. Figure 1 demonstrates that RNA quantities were quite similar, with the exception of 2 samples, one of which produced better results with the automated technique, while the other one produced better results with the manual technique. Overall, the difference in RNA quantity obtained with the 2 techniques was not statistically significant.
The RNA quality assessment was extended through the simple spectrophotometric evaluation of protein and salt contaminations, using the 260/280 nm and 260/230 nm absorbance ratios, respectively. Figures 2 and 3 demonstrate that results were very similar with the 2 techniques for the 25 assayed samples.
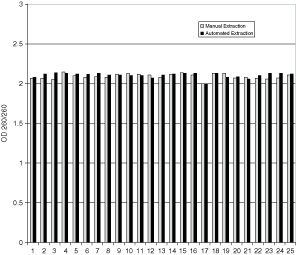
Protein contamination evaluated by the 260/280 optical density (OD) ratio for each of the 25 tested samples; P = 0.106.
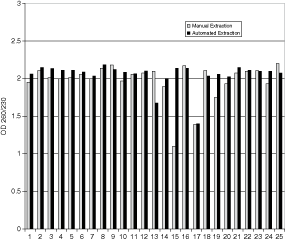
Saline contamination evaluated by the 260/230 optical density (OD) ratio for each of the 25 tested samples; P = 0.09.
Finally, it was determined whether the obtained RNAs were fit for quantitative RQ-PCR. Abelson (ABL) is a common internal control for detection and follow-up of fusion transcripts used in molecular hematology laboratories, with particular relevance to the detection of BCR-ABL in patients with chronic myeloid leukemias.2 Figure 4 shows that Ctm values obtained for ABL amplification were similar for RNA extracted with the manual or automated technique.

Median cycle threshold (Ctm) values for manual vs. automated techniques; P = 0.68.
The importance of RNA quality and the deleterious effects of inadequate pre-analytical handling and storage have been largely underlined, particularly for applications such as molecular profiling.3,4 Depending on planned uses, RNA obtained by one or another technique may be more or less fit. The data suggest that the use of an automated RNA extraction technique using the QIAcube device is an acceptable alternative to a manual extraction technique, for such routine applications as molecular diagnosis or minimal residual disease monitoring in patients with hematological malignancies. The QIAcube device yields high-quality RNA from cryopreserved human blood samples and appears to be suitable for clinical laboratories that process 1–24 samples per day.
Other reports have been published looking at various technical aspects of nucleic acid extraction techniques that can affect the quality and quantity of obtained material, as well as the sensitivity of the final analytical step. Many of these reports dealt with issues in microbiology5–14 or veterinary sciences,15 or both.16 Studies with cells or tissues of human origin are less numerous,3,4,17–21 and not all of those reported on RNA extraction.3,4,15,17,19,21 Several studies focused on RNA conservation at the preanalytical step3 or on the nature of used reagents and the RNA capture4,17,19 rather than on the question of automation. A previous study designed similar to this study,20 however, concluded as to the inferiority of the automated RNA extraction technique, when using the amplification of a housekeeping gene from bone marrow samples obtained from myeloma patients. Conversely, a semi-automated procedure was found to be superior to the manual technique for the challenging task of extracting RNA from formalin-fixed paraffin-embedded tissues.21
Automation of RNA extraction facilitates standardization, intra- and inter-laboratory reproducibility, and limits operator-associated variations, errors due to manual pipetting, and contamination due to unsealed intermediate steps. In addition, automation can contribute to cost reduction, through reduced workload for laboratory personnel. This is most important as recent years have witnessed the emergence of new and highly effective treatments for hematological malignancies; these treatments allow physicians to induce clinical and hematological remissions in higher proportions of patients, who are now monitored at the molecular level; this information is critical in order to adapt treatment. Thus the demand for molecular analyses searching and monitoring for somatic or constitutional genetic abnormalities is likely to increase in the forthcoming years.
Footnotes
Acknowledgments
This study was supported in part by Institut Paoli-Calmettes, and by grants from the Direction de l’Hospitalisation et de l’Organisation des Soins (DHOS) at the French Ministry of Health and from the Institut National du Cancer (INCa). The authors thank Mr. Olivier Ouvrard (Qiagen) for allowing the evaluation of the Qiacube instrument and providing reagents free of charge. The authors also wish to express their appreciation to Dr. Boris Calmels for helpful discussions.
Author Disclosure Statement
The authors have no conflicts of interest to disclose.