
Abstract
In the last few years, conditions for setting up a human biobank in France have been upgraded by taking into account (1) the new laws and regulations that integrate the ethical and societal dimension of biobanking and delineate the risks for patients associated with the procurement of human cells and tissues, (2) the increasing request by scientists for human samples with proven biological quality and sophisticated sets of annotations, including information produced through the evergrowing use of molecular biology in pathology, and (3) establishment of procedures concerning the safety of the personnel working with biological products. For this purpose, health authorities and national research institutes in France have provided significant support for the set up of biobanks. The present work was conducted to describe how we set up a biobank targeting diseases of a specific organ (thyroid gland), with the aim of rapidly developing translational research projects. The prospective experience of a single institution (Pasteur Hospital, Nice, France) over a 6-year period (2004–2009) is presented from the practical point of view of a surgical pathology laboratory. We describe different procedures required to obtain high-quality thyroid biological resources and clinical annotations. The procedures were established for the management of biological products obtained from 1454 patients who underwent thyroid surgery. The preanalytical steps leading to the storage of frozen specimens were carried out in parallel with diagnostic procedures. As the number of international networks for research programs using biological products is steadily increasing, it is crucial to harmonize the procedures used by biobanks. In this regard, the described thyroid biobank has been set up using criteria established by the French National Cancer Institute (Institut National du Cancer) to guarantee the quality of different collections stored in biobanks.
Introduction
As the final goal of translational research is not only to identify new cellular and molecular mechanisms that lead to the onset, or modify the course of a disease, but also to improve treatment and establish preventive programs, the setting up of such biobanks is of key importance. 5 In this regard, substantial efforts have been made in recent years to build a network of human biobanks in France. A significant number of projects were supported by different French institutions to set up biological collections for clinical and translational research (www.e-cancer.fr/Espace-tumorotheques; www.crbfrance.fr). Many of these human biological collections mostly include frozen tissue specimens. 6 Thus, the criteria for collection and storage of human biological products of high quality have been established. 7 As some of these criteria were recently redefined, a number of collections that were set up a few years ago do not currently fulfill all new defined criteria. 7 Thus, numerous frozen human tissues and other biological materials collected by many biobanks in France cannot be fully exploited, particularly for international network projects and/or for current programs that use sophisticated biotechnological approaches, such as deep sequencing technology. 8 Moreover, a great number of frozen specimens stored in these biobanks have probably not been collected with the signed consent of patients and thus cannot be used for clinical research in Europe.
Despite the large number of human biobanks that exist all around the world and the importance of biobanking for the development of translational research, there are only a few reports reviewing the practical aspects of setting up such a biobank. Since 2004 we set up a prospective human biobank, focusing on a limited number of diseases and organs, particularly the thyroid gland (http://www.biobank06.com). 9 For this purpose, we used the different criteria defined and recommended by the French National Cancer Institute [Institut National du Cancer (INCa)], 7 to which we added complementary clinical and pathological criteria for this organ. Moreover, we collected frozen tissue, plasma, serum, constitutional DNA, and embedded paraffin tissue for tissue microarrays (TMAs) from each patient and developed primary cultures of thyrocytes from certain specimens of interest.
This article is intended to provide our view of “best practices” referring to thyroid pathology biobanking. We address issues related to the collection and annotation of thyroid samples and the ethical and administrative aspects of biorepository management. Through the evaluation of our experience (Pasteur Hospital, Nice, France) from 2004 to 2009, we provide clues on how to prospectively set up an organ-oriented biobank that can be rapidly used for translational research as a high-quality resource for both nontumoral and tumoral diseases.
Patients and Methods
Ethics, consent, informative procedures, and confidentiality
This study was conducted between September 1, 2004, and December 31, 2009, in the biobank of the Pasteur Hospital in Nice. This biobank is certified according to NF 96S-900 certification (No. 2010/36548) and Inserm (Institut National de la Santé et de la Recherche Médicale) and IBiSA (Infrastructures en Biologie Sante et Agronomie; www.ibisa.net) criteria. Moreover, all patients hospitalized in the Department of Oto-Rhino-Laryngology (Pasteur Hospital) and who underwent thyroid surgery were systematically included in this study. Patients were informed by the surgeons (N.G., L.C., J.S.) of the reason for the different procedures and the goals in setting up a biobank. An information leaflet was provided to patients before surgery. A consent form was signed by both the patient and the surgeon before surgery, establishing permission to obtain frozen thyroid specimens, plasma, sera, constitutional DNA from blood, primary thyrocytes for culture, and embedded paraffin tissue for TMA construction. 10 The patients were informed that all data, particularly clinical data, stored in the biobank were anonymized to protect patients. The different procedures concerning the anonymization of patients' data were approved by the CNIL (Commission Nationale de l'Informatique et des Libertés; www.cnil.fr).
The thyroid specimens and derived products from blood patients were then systematically frozen in the surgical pathology laboratory [Laboratory of Clinical and Experimental Pathology (LCEP), Nice, France] and stored in the biobank unit.
Clinical and epidemiological data and patient follow-up
The clinical and epidemiological data were obtained by the physician during the preoperative visit of the patient. Collected items include the family and patient's medical history, physical symptoms, thyroid ultrasound results, main biological tests, and the results of thyroid fine-needle biopsy aspiration (an example of the recorded items can be seen at http://www.biobank06.com). After histological diagnosis, the therapeutic strategy was recorded. Patient outcome was systematically evaluated and updated every 6 months.
Tissue specimen management
After resection, each surgical thyroid specimen was placed in a plastic sterile container (125 mL; Dutscher, Brumath, France) and then in an envelope for vacuum transport (Décomatic, La Verpillière, France) from the Department of Oto-Rhino-Laryngology to the LCEP through a pneumatic tube. The time elapsed between the surgical procedure and freezing was recorded. Surgical thyroid specimens were photographed before freezing and these images were recorded in a database.
Specimens indicated for freezing procedures were obtained during the preparation of frozen sections for diagnosis, all else was routinely frozen. Selection of the different specimens was performed by a senior surgical pathologist (S.L., V.H., M.I., C.B., P.H.). This was done under a hood, with sterile gloves and a sterile razor blade, on a dedicated surface area cleaned with RNAse up solution (Molecular BioProducts, San Diego, CA). All scissors and forceps were cleaned with RNAse up solution before use. Specimens taken for freezing were selected by macroscopic examination of gross lesion(s) and normal tissue. In the case of several lesions, they were numbered (lesion 1, lesion 2, etc). Depending on the size of the lesion, between 1 and 10 specimens were frozen in liquid nitrogen (LN2). The size of frozen specimens depended on the size of the lesion(s). However, most of the frozen specimens had a volume of around 0.5 cm3. In parallel, and whenever possible, thyroid specimens (from 1 to 10) from macroscopically nonaffected areas were similarly processed. Finally, all specimens were stored in cryotubes (1 specimen per tube) (1.8 mL, Nunc cryotube; Dutscher) and weighed immediately before freezing. Among the different frozen specimens in LN2, 1 was used for subsequent RNA extraction (first specimen to be frozen) and 1 was used for subsequent DNA extraction (last specimen to be frozen). When regional lymph node excision was performed, specimens were similarly frozen for biobanking after frozen sections were obtained for diagnosis. The different lesions and areas to be frozen in LN2 were schematically reproduced on a sheet to give a thyroid cartoon. During the freezing procedure, the mirror image of the frozen tissue specimen was taken for formalin fixation. A deparaffinized section of this tissue mirror embedded in a paraffin block was stained with hematoxylin and eosin. Then, the mirror images of representative samples of snap-frozen thyroid lesions and normal adjacent tissue were photographed, and all images were archived with the biobank software (Cresalys Software; Alphelys, Paris, France). The samples obtained from patients with a known associated infectious pathology (human immunodeficiency infection, hepatitis B and C, tuberculosis, etc.) were stored separately from samples obtained from other patients. Some frozen specimens with potential value for improving diagnosis and/or prognosis (particularly for lymphoma and sarcoma) were separately managed. In this regard, registration with biobank software of these latter frozen specimens was linked to supplementary information saying that these rare specimens can be used immediately to obtain data for improvement of diagnosis and/or prognosis (for example, by doing molecular biology analyses) if necessary. The use of these specimens for research projects requires more than 1 frozen specimen. Finally, the main data were recorded and summarized on a single datasheet (www.biobank06.com) (Fig. 1). The different criteria allowing inclusion of thyroid tissue in the database are shown in Table 1.

Example of a datasheet for recording the main data for inclusion. A color version of this figure is available in the online article at www.liebertonline.com.
Pathological data
Gross macroscopic and histological data and pathological tumor node metastasis staging were recorded on a sheet that was filled in by pathologists. The list of these items is available at www.biobank06.com. A subset of this collection appears at www.paca-biobank.com.
Tissue microarrays
The tissue specimens included in paraffin blocks were used to prepare TMAs that are specific for different thyroid pathologies. Depending on the size of the initial lesion, 0.6-mm spots were obtained in triplicate using an arrayer (Alphelys). At least 4 identical TMA paraffin blocks were set up in parallel using a booster system (Alphelys).
Blood sample management
Since October 2006, blood samples were collected in parallel in the biobank. A sample of blood was obtained from patients before surgery. Two tubes, 1 with ethylenediaminetetraacetic acid containing some tripotassium ethylenediaminetetraacetic acid 3 (Greiner Bio-One, Frickenhausen, Germany) and another without anticoagulant, with 10 mL of blood were transferred to the LCEP through a pneumatic tube. Blood was immediately centrifuged, and plasma and sera were collected under a hood in a culture room.
Primary culture of thyrocytes
A collection of primary cultures of thyrocytes was set up from certain surgical specimens representing diverse diseases (conventional papillary thyroid carcinomas, follicular variant of papillary thyroid carcinomas, tumors of uncertain malignant potential, adenomas, Graves' disease, and normal thyroid tissue). For this purpose, thyroid tissue was obtained from 39 human subjects undergoing surgery for solitary or multiple nodules. Nodules were removed and separated from healthy tissues. Both affected and unaffected tissues were used for the preparation of cells for culture in vitro. Follicles were prepared and plated on Petri dishes as previously described. 11
Quality assessment and nucleic acid collection
RNA and DNA collection were set up in parallel. One specimen of affected thyroid tissue and 1 specimen of presumably healthy thyroid tissue were specifically dedicated to the nucleic acid biobank. RNA was extracted using a Trizol procedure. The RNA quality was evaluated from the 28s/18s ratio and the RNA integrity number (RIN) on an Agilent Bioanalyzer 2100 (Agilent Technologies, Santa Clara, CA). Similarly, DNA was extracted from another pair of tissue samples. The DNA quality was measured by PCR amplification of a fragment of 950 bp. Extraction was done from 1 selected specimen of each tumor from 2004 to 2006 to set up stocks of nucleic acids. However, because of time and cost limitations, since January 2007, nucleic acid extractions were then performed once a week from 1 specimen only, to control the quality of the freezing procedure (particularly the time of cold ischemia). Moreover, once a month, 1 frozen specimen stored at −80°C for 6 months was taken, and both the DNA and RNA quality was evaluated by either PCR amplification or evaluation of the RIN, respectively, and recorded.
Storage facilities and safety procedures
Cryotubes containing tissue specimens were initially placed in boxes (cryoboxes, which can contain 81 cryotubes; Dutscher) and stored in an LN2 container with a temperature recording system (Taylor-Warthon, Husum, Germany). However, a “backup” empty LN2 storage tank was available in the facility. Once a week, the cryoboxes were placed in −80°C freezers dedicated to thyroid tissue collection. Freezers were equipped with a permanent temperature recording system and an independent centralized alarm. Two backup empty −80°C freezers were available and a technician was on call in case of failure. Plasma and sera were stored in a −140°C freezer with an identical security system as that for the −80°C freezers. One backup empty −140°C freezer was available. RNA and DNA samples were stored in a −80°C freezer. Finally, primary cultures were stored in a nitrogen tank. The alarm was set to detect temperature increases above −65°C for the −80°C freezers and −130°C for the −140°C freezers. General access to the biobank unit and to the LCEP is regulated by personalized magnetic cards. Access to the cryoconservation room is strictly controlled and limited to staff members with a digicode system for regulating access. The opening of the different freezers was regulated and recorded. Paraffin blocks and slides were stored at room temperature and TMAs at 4°C. For these latter samples, the refrigerator had permanent temperature recording and an alarm setup to detect temperature increases above 8°C. Between 6 pm and 8 am, the biobank unit is protected by a central alarm and digicode access. The general organization of the surgical pathology laboratory (LCEP) and biobank unit space can be seen at www.biobank06.com and is shown in Fig. 2.

Floor plan of the biobank unit and the surgical pathology laboratory (Laboratory of Clinical and Experimental Pathology). A color version of this figure is available in the online article at www.liebertonline.com.
Information technology
The information technology system allows patient registration, specimen tracking, biological material cataloging, quality control, and specimen availability. Thus, the clinical, epidemiological, pathological (including images), and biological information and the inventory of tissues and biological products are managed with the same specific software (Cresalys Software; Alphelys). An example of available information can be accessed at www.biobank06.com (CHU of Nice). A summarized datasheet can be accessed for each patient (Fig. 1) (www.biobank06.com). Supplementary information can be accessed at www.biobank-paca.com. However, all available information for each patient is stored using the biobank software. Data are checked before final validation that displays the main information (Table 1).
Results
Patient consent and thyroid specimens
From September 1, 2004, to October 31, 2009, 1544 patients underwent surgery for a thyroid disease; 1454 of 1544 (94%) thyroid specimens and derived samples were included in the biobank; 6% (90/1544) of thyroids was not included because (1) the size of the tumor lesion was less than 0.3 cm, (2) the delay between surgical resection and tissue management (cold ischemia) was considered to be too long (longer than 30 min), (3) the patient did not give consent (n = 2); 93% (1440/1544) of patients signed consents for inclusion of tissue and blood samples in the biobank (Fig. 3). Consent was obtained before surgery in 1380 of 1440 (96%) and retrospectively in 60 of 1440 (4%) patients. If thyroid specimens were not obtained despite the patient's consent, a feedback note was given to the patient to explain why a sample was not stored frozen. The percentage of frozen thyroid tissues included with signed consent forms obtained per year is shown in Fig. 3A. Thyroid tissues associated with the following pathologies were included in the biobank: malignant tumors (253 cases), benign tumors, including the so-called tumors of uncertain malignant potential (388 cases), 12 nodular hyperplasia (673 cases), Graves' disease (111 cases), and thyroiditis (29 cases) (Fig. 3B).

Details of the different thyroid pathologies
The details of the malignant and benign pathologies are shown in Fig. 4A–C. For 34 of 1454 (2%) of cases, the potential infectious status was prospectively (22 cases) or retrospectively (12 cases) known. These include HIV (16 cases), hepatitis B or C (17 cases) seropositivities, and tuberculosis (1 case) disease; 2 of 1454 thyroids, which corresponded to mesenchymal (1 case) and lymphoma (1 case) tumors, were considered for inclusion in a different database following the INCa recommendations (www.e-cancer.fr). The age and sex of patients together with the different diseases are summarized in Table 2.
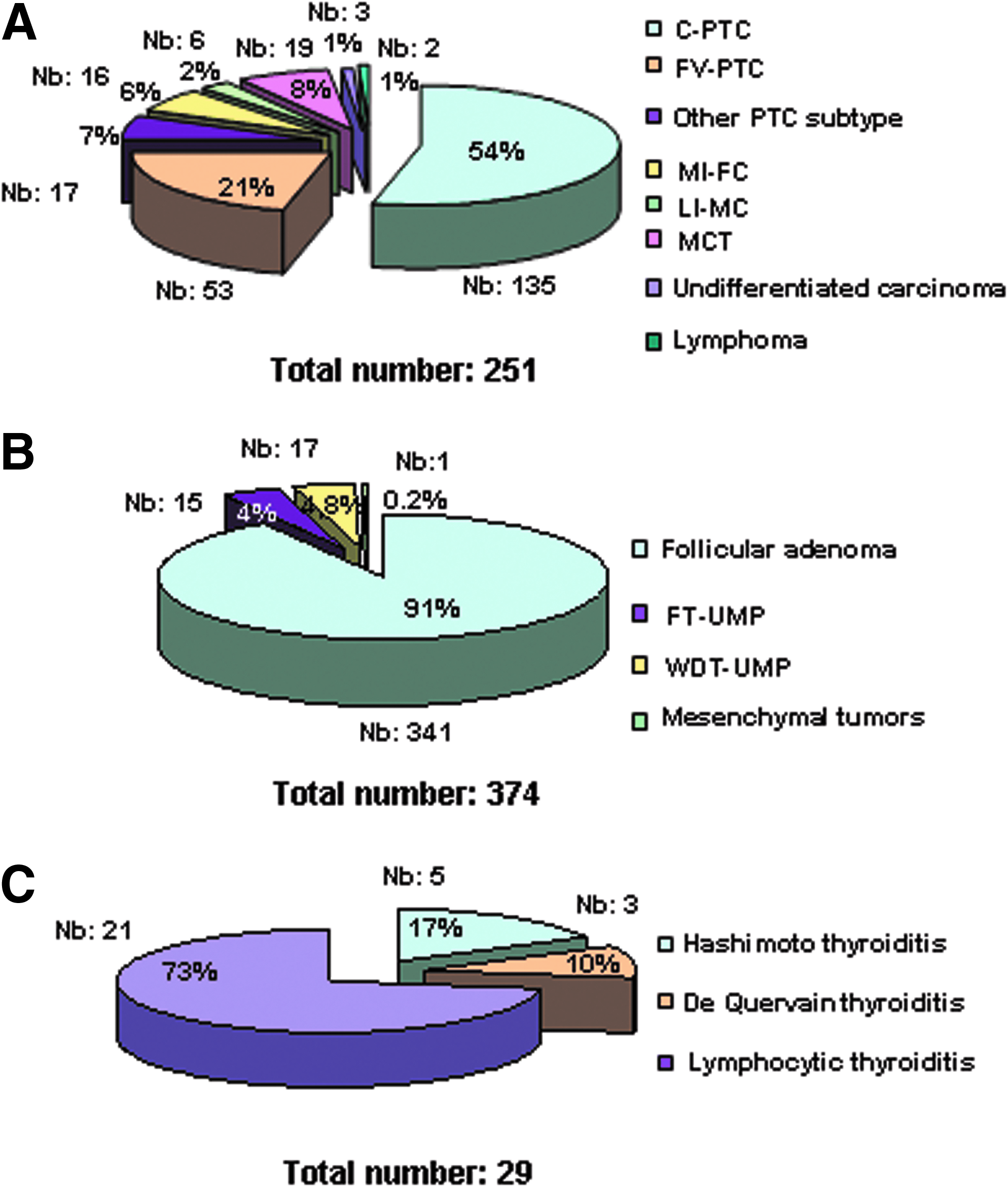
FT-UMP, follicular tumor of uncertain malignant potential; WDT-UMP, well-differentiated tumor of uncertain malignant potential; C-PTC, conventional papillary thyroid carcinoma; FV-PTC, follicular variant of papillary thyroid carcinoma.
Frozen tissue specimens
Frozen tissue specimens were obtained during preparation of a frozen section for diagnosis (350/1454; 24%) or were prepared systematically (1104/1454; 76%). For most cases, at least 1 tissue specimen with a lesion and 1 specimen presumably without a lesion (confirmed by histological evaluation) were frozen. The average number of prepared cryotubes per surgical specimen of thyroidectomy was 14 (7 tubes for tumor or other lesional tissue and 7 tubes for presumably adjacent healthy tissues). For 200 of 1454 (14%) thyroids, only affected tissue specimens were frozen because normal thyroid tissue was not available. For 60 of 1454 (4%) surgical specimens, only presumably normal thyroid tissue was frozen because the affected area was too small to be taken for freezing. Finally, a total of 9967 specimens were frozen and the distribution according to the diagnosis is summarized in Table 3. The mean weight of the frozen specimens per pathology and per cryotube is listed in Table 4.
Blood samples
Since September 2006, prospective collection of plasma and sera was set up in parallel to tissue collection for all patients undergoing thyroid surgery. For 600 of 1454 (41%) patients, blood samples are available; 1250 plasma and 873 serum aliquots have been currently stored.
Nucleic acid samples extracted from tissue specimens
The time between surgical thyroidectomy and freezing varied from 15 to 30 min (mean time: 23 min). RNA and DNA were extracted from 510 specimens from 510 patients. The quality of the DNA and RNA was controlled as described in the Patients and Methods section and as previously described. 13 The quantity and quality of the extracted nucleic acids from a quite similar weight of tissue varied depending on the pathology. Overall, the quantity of extracted nucleic acids per 50 mg of thyroid tissue was higher in tumor tissues than in nontumor or normal tissues. However, quality was variable depending on the underlying disease. Thus, for example, lesional tissue showing an intense inflammatory infiltrate (thyroiditis or severe lymphocytic reaction associated with papillary thyroid carcinoma) had a lower RIN, between 4.5 and 6.9 (mean = 6.3), than those of the tumors associated with a low level of inflammatory and necrotic areas, which had an RIN comprised between 6.8 and 9.1 (mean = 7.5).
After having collected RNA and DNA systematically from each thyroid for 2 years, the extracts were made available for specific research projects. To check the quality of the different procedures set up for the biobank, the quality of the RNA of 1 of each 20 thyroids is systematically controlled nowadays.
TMA paraffin blocks
The selection of the areas of interest for building TMAs was made by one of the surgical pathologists (S.L., M.I., I.L., C.B., or P.H.) on the different sections stained with H&E. These different slides were stored. As a result, TMAs are available for the following diseases: papillary carcinoma (28 paraffin blocks), follicular carcinoma (26 paraffin blocks), tumor of uncertain potential malignancy (18 paraffin blocks), nodular hyperplasia (14 paraffin blocks), adenoma (28 paraffin blocks), Graves' disease (20 paraffin blocks), and thyroiditis (8 paraffin blocks). Each block includes between 45 and 90 cases (with both selected lesional and perilesional areas in triplicate).
Primary cultures of thyrocytes
The success rate in establishing cell lines from the primary cultures was high, as epithelial cells from only 4 of 39 thyroid specimens were not obtained for unknown reasons. We checked that cultured cells obtained from the thyroid biopsy specimens shared biological features of thyroid tumors in situ. In particular, we looked at the phenotype of these cells obtained from primary cultures by immunocytochemistry using antibodies against antigens expressed by neoplastic and/or normal thyrocytes (thyroglobulin, thyroid transcription factor-1, cytokeratin 19, galectin 3, HBME1). We obtained a similar staining profile for epithelial cells from both primary cultures and biopsies. We concluded that the phenotype of the cells in primary culture tolerate cryopreservation well. Thus, the primary culture of thyroid biopsy material should not affect the ability to preserve biospecimens for other research purposes.
Discussion
The rules and conditions for biobanking have changed dramatically in France since the beginning of 2000. This occurred for 2 main reasons: (1) the continual increase in the use of human cells and tissues and other biological material for translational research, and (2) rapid progress in biotechnological approaches. 14 In this regard, “modern” biobanks are now dependent on different biotechnological methodologies.15,16 It is essential to develop national and international cooperation and to harmonize quality controls to satisfy future needs. The information given for “best practices” for biobanking by some institutions or organizations such as the International Society for Biological and Environmental Repositories (http://www.isber.org) is of great interest. 17 Although information concerning the diagnosis of many disorders can now be obtained from formalin-fixed, paraffin-embedded tissues using, for instance, PCR-based testing rather than depending solely on fresh or frozen tissue, the need for preservation of unfixed tissue and other biological material remains an important requirement for the development and validation of new molecular tests, including those ultimately designed to use fixed archived tissue. 5 Thus, frozen samples provide a crucial source of biochemically unaltered nucleic acids and proteins for translational research designed to investigate the mechanisms of diseases.
Frozen-tissue banks are an important resource for molecular pathology laboratories. However, the development of a frozen-tissue bank requires implementation of very efficient methods for collecting and freezing samples of fresh abnormal and normal tissues as a part of the routine activity of surgical pathology laboratories. It is also necessary to preserve additional types of frozen samples, such as cultured tumor or nontumor cells, serum, or plasma samples as well as aliquots of isolated DNA and RNA. Moreover, the growing clinical application of molecular diagnostic techniques requires standardization of the methods used to freeze, store, and inventory biological samples. 5 However, it is difficult to systematically perform all these procedures for all specimens in the course of the routine activity of a surgical pathology laboratory. Consequently, we strongly believe that it is best to initially focus these procedures on only selected pathologies and/or organs. Thus, the present study describes the experience of an academic institution (Pasteur Hospital) in setting up a biobank targeted mainly to thyroid pathology.
We focused on thyroid pathology for different reasons. First, the incidence of thyroid lesions, particularly of thyroid cancer, is currently increasing in different parts of the world, particularly in Europe and the United States.18–21 It is noteworthy that despite this increase, and in comparison to other types of carcinomas, there are currently only few available collections of such tumors, particularly in France. 6 We also took the opportunity to collect frozen and paraffin-embedded tissue (TMAs) and different biological fluid samples from patients with thyroid diseases, as thyroid surgery is a major activity of our institution and because of the high number of patients with diseases of the thyroid in our geographical area. From the pathologists' viewpoint, controversial aspects of thyroid diseases and interindividual variations in the diagnosis of certain lesions such as follicular well-differentiated thyroid lesions justify the development of new tools designed to improve the accuracy of diagnosis.12,22–24 In addition, recent studies that concern the molecular mechanisms of thyroid tumorigenesis and future studies that aim to develop new approaches leading to more accurate diagnoses will probably be done using frozen biological specimens.25–27 Finally, some thyroid cancers such as carcinomas refractory to conventional treatment and some medullary carcinomas are particularly aggressive. As they do not benefit from satisfactory therapeutic approaches, new targeted therapies are currently being developed.28,29 In this regard, targeted therapies will put into practice the discoveries of molecular mechanisms of carcinogenesis.30,31
The thyroid biobank of the Pasteur Hospital is made up of different biological collections obtained from the same cohort of patients. These collections were established in compliance with criteria defined by INCa in 2006. 7 Although most grants are targeted to projects into cancer research, particularly in France, it is also important to collect nontumor tissue from the same organ, because many interesting translational research projects can be developed for benign, dystrophic, autoimmune, and inflammatory processes that arise in the thyroid gland. Thus, we have set up a biobank that includes tumor and nontumor diseases. 9
In the last few decades, an increasing number of human biobanks have been set up around the world, which underlies the usefulness of obtaining different biological products for human clinical and translational research.32–34 Before beginning the current project, we questioned whether it was still worth creating yet another biobank. Finally, we concluded that it was necessary to go in this direction for different reasons. Some previously established collections may not remain available for research, as they cannot fulfill some of the criteria and standards for biobanking that were established later.35–39 Although there are many scientific justifications for the creation of tissue and DNA databanks, the storage and use of human biological materials continue to face legal dilemmas and stimulate discussion.40–49 It is necessary to obtain for clinical research a consent form signed by the patient. Moreover, complete epidemiological and clinical data, follow-up of the patient, pathological data, digitalized images corresponding to frozen tissue specimens, and data concerning the quantity and the integrity of nucleic acids are also necessary.
With the widespread use of nucleic acids and proteins, hundreds of biomarkers are in need of validation in cohorts of well-annotated clinical samples. TMAs are emerging as the tool for performing rapid protein expression analyses on a large number of clinical samples. 50 As TMAs represent an increasingly validated means of understanding the clinical impact of diagnosis-, prognosis-, and therapy-related markers, we decided to prospectively set up TMAs that are representative of different thyroid pathologies.
Attention must be paid to different safety procedures. The strict confidentiality of all clinical and pathological data must be respected. This should allow the use of human biological products for targeted projects and help the transfer of collected tissue to other countries. Except for some rare lymphomas or sarcomas arising in the thyroid, all collected tissues in our thyroid biobank qualify for use in clinical and translational research. 51 Before giving access to human thyroid samples, each project is evaluated by a scientific committee. All projects are submitted to the ethics committee at our institution. The different procedures used before transfer of material for translational research are listed in Fig. 5.

Different steps from the submission of a project for translational research to the discharge of samples for performance of the project. *See criteria for inclusion of samples in Table 1. MTA, material transfer agreement.
All procedures for setting up the thyroid biobank have been made by a permanent and professional staff that is specifically dedicated to this activity: technicians working with the pathologists in freezing and storing samples; technicians for nucleic acid extraction and control of integrity; technicians for the plasma, sera, and primary culture bank; technicians for data and quality control management; a secretary for registration and procedures; and a pathologist to control the different histological images (www.biobank06.com/annual). The biobank is physically located in the Department of Surgical Pathology (www.biobank06.com; center of biological resources/partners) and its operation is supervised by a surgical pathologist who oversees the scientific and administrative aspects.
The usefulness of establishing such a biobank targeted to a single pathology needs to be evaluated in the future. Different indicators will rapidly help check if setting up this large biobank is of interest. In particular, these indicators will include the evaluation of the ratio between the number of stored and used samples, the number and impact factor of publications where the name of the biobank is mentioned, the number and quality of scientific collaborations, and the number of samples sent and sold to academic and private partners. Estimation of the cost of human biological resources is difficult and depends in particular on the different facilities set up in the biobank and on the expertise area of the biobank. As an example, for academic partners, we used the costs recommended by the INCa in France (www.e-cancer/recherche/les-ressourcesbiologiques). Finally, a biobank of high standing could become a cornerstone in large translational consortia. In this regard, the thyroid collection of the biobank will be included in different programs of translational research currently sponsored by the INCa. Moreover, it is probable that such a thyroid biobank will benefit patients, by exploring different new molecular events.
There are many reports of the modus operandi of population-based and disease-specific research biobanks. These publications reveal both the diversity of the approaches and some common difficulties. The cost of establishing a human biological collection is high. It is thus necessary to establish collaboration with academia and industry and network with different biobanks working on similar targeted pathologies. For this reason, this biobank participates in the local canceropole Provence Alpes Côte d'Azur (PACA) consortium (http://www.canceropole-paca.com) as well as in the current European biobanking project. 8 We strongly believe that the development of a human biobank requires implementation of efficient methods for collecting and freezing samples of fresh tumor and normal tissues and biological fluids as a part of the routine activity of surgical pathology laboratories. Moreover, the effort made will only be productive if biobanking and its associated computing systems encourage the translational bridge linking new molecular information to its clinical significance.52,53 Finally, it should be kept in mind that the setup of a biobank of high quality for different types of human biological materials ultimately aims to satisfy the interests of the patient community. 54 In this regard, the integration of biological resources from well-organized biobanks with powerful molecular and “omics” approaches and bioinformatic tools hold promise in advancing further our knowledge of disease development, thus leading to better prevention and treatment strategies.
Footnotes
Acknowledgments
Author Disclosure Statement
No competing financial interests exist.