
Abstract
The biobanking literature frequently addresses donor and societal issues surrounding biobanking, but the biobanker's perspective is rarely highlighted. While not comprehensive, this article offers an overview of the human aspects of biobanking from the viewpoint of biobank personnel—from biobank formation, through the process, and in addressing post-biobanking issues. As every biobank and biobank network may differ, such factors may vary. Before biobanking can commence, the purpose of the biobank network must be defined, and buy-in achieved from many stakeholders. An attitude of trust and sharing is essential, as is good communication. Developing a biobank is time consuming and laborious. Forming a network requires significantly more time due to the need for cross-institutional harmonization of policies, procedures, information technology considerations, and ethics. Circumstances may dictate whether development occurs top-down and/or bottom-up, as well as whether network management may be independent or by personnel from participating biobanks. Funding tends to be a prominent issue for biobanks and networks alike. In particular, networks function optimally with some level of government support, particularly for personnel. Quality biospecimen collection involves meticulously documented coordination with a network of medical and nursing staff. Examining and sampling operative specimens requires timely collaboration between the surgical and pathology teams. “Catch rates” for samples may be difficult to predict and may occur at a frequency less than anticipated due to factors related to the institution, staff, or specimen. These factors may affect specimen quality, and have a downstream effect on competition for specimens for research. Thus, release of samples requires a fair, carefully constructed sample access policy, usually incorporating an incentive for researchers, and an encouragement to form collaborations. Finally, the public and patient groups should aim to understand the benefits of a biobank network, so that patient care is improved through coordinated biobanking activity.
Introduction
The purpose of this article is to shed light on the human side of biobanking. Most biobankers face the daily challenge of supplying researchers and clinicians with high-quality specimens and data for translational research on one hand, while protecting donor rights on the other. Further, they must work closely with multiple stakeholders within and outside the biobank. This article focuses on cancer tissue biobank networks, although the conclusions may also be relevant to other types of biobank networks. Operating an efficient biobank network requires a collaborative, transparent attitude, and at least a partial suspension or dilution of the prevailing culture of individual achievement. Our observations are based on recent experience in establishing and managing Spanish, Swiss, Irish, Israeli, Dutch, Canadian, and many other biobank networks.
Purpose, Goals, and Getting Started
At the outset, the purpose and goals of the biobank network must be clear: biobanking is not an end in itself. A biobank network has potential to expedite translational research, providing sufficient numbers of biospecimens and data in rare diseases or subgroups of common ones, for clinical trials, and for validating new biomarkers and drug targets. Harmonization of the participating biobanks (information technology/database; ELSI, certification, etc.) can promote improved data interconnectivity. Eventually, the utilization of biospecimens and stored data can be optimized resulting in an increased number of collaborations and exchangeability. Biobanking activities may be restricted (eg, only breast cancer), may facilitate both prospective projects and biobanking for undefined future projects, and may or may not release samples to industry. 7
Every biobank network is different, being managed either by representatives of a participating biobank or independently. In the former case, the potential risk of a conflict of interest is greater. In either case, representatives of the participating biobanks may be included in an Advisory Board. The main interactions of a biobank manager working in a network are highlighted in Fig. 1.
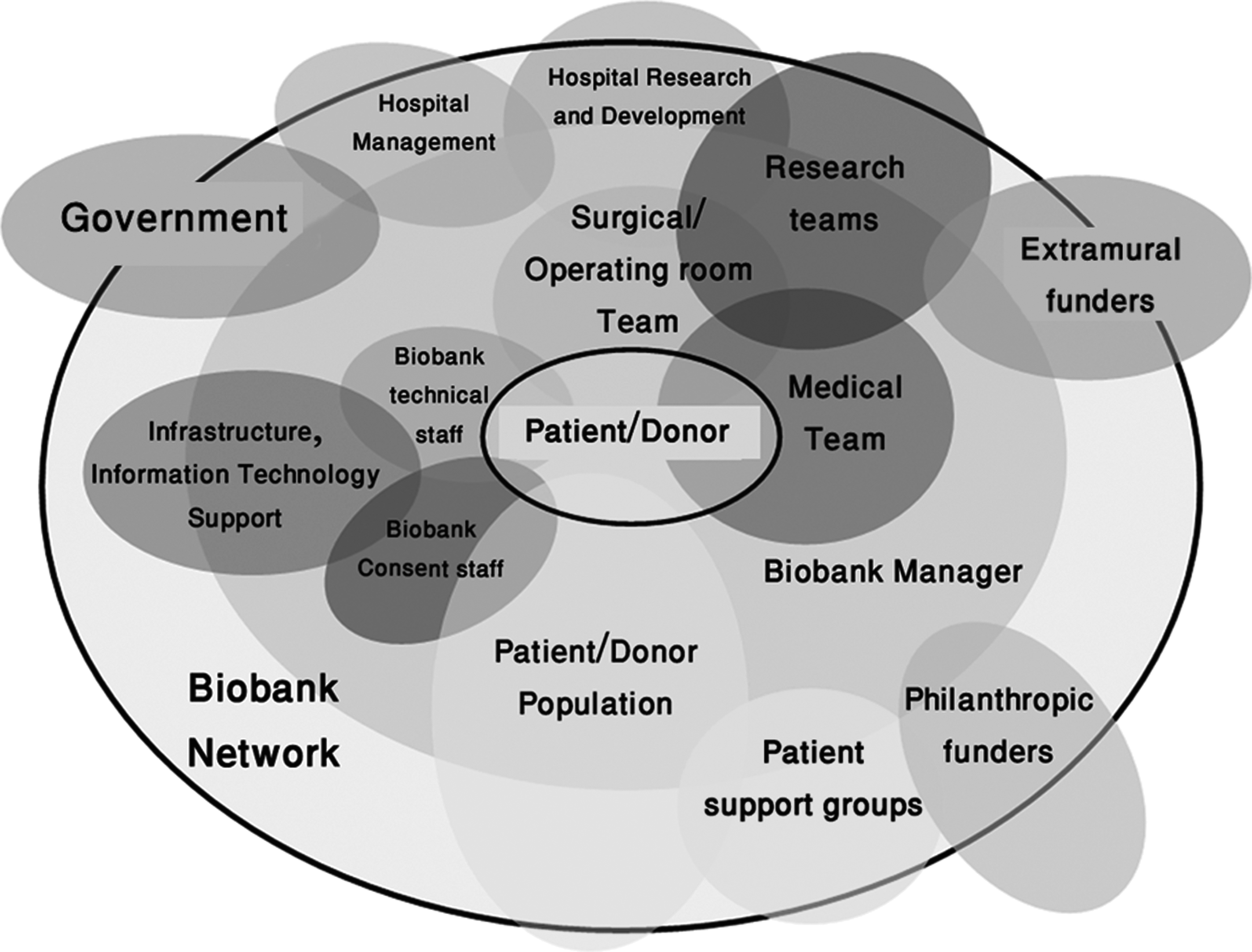
A manager within a biobanking network regularly interacts with at least 13 groups, some of which may overlap, over the course of the network's life cycle.
Establishing a national biobank network is a lengthy process, and depends on local, regional, and national circumstances, regulations, and the actions of managers and ethics committees. The process takes even longer if the biobank is not supported by government or institutional funding.
Donor Buy-In
Historically, patients tend to trust their carers and give consent, once they are consulted and have faith in the biobank. 8 Regardless, patients need to be informed and consent that their samples and non-personal data will be shared across a network. Donors are typically altruistic and want their samples to be used appropriately and efficiently to benefit others who develop their disease in the future. 9 Public awareness of the benefits of biobanking may eventually lead to widespread use of “broad consent” in which donors understand that tissue samples surplus to diagnostic requirements will normally be taken for research unless they opt out.
Institutional Buy-In
Institutional review boards/human research ethics committees (IRB/HREC, REB) are becoming increasingly concerned by the possibility, even if remote, that the information gleaned from genomic, proteomic, and other “-omic” studies might bring harm to sample donors. Thus, the ethics deliberation and approval process may take several months or longer for some new biobanks. 10 Biobanking regulations are lacking in many countries, and IRBs/HRECs/REBs and funders alike still wrestle with decisions regarding biobank activities and biobank networks, that is, access, return of research results, and intellectual property.
As many well know, establishing a biobank and managing one within an academic center are very different experiences, both with unique challenges. The biobank personnel will know this, but often the funding stakeholders not involved in daily operations may not be as aware of critical issues such as formulating legal documents, or the complexity required for reaching a fair compromise between collectors and end-users (who may be the same people) about sample access. Conflict of interest should be evaluated in this instance. Research utilization committees and Technology Transfer Offices may offer additional guidance and support in this regard, but are often just one part of the solution. Regardless of approach, transparent and timely communication across all parties is crucial to foster success (Box 1). In the long term, demonstrated public and private support from the governing stakeholders is frequently the most critical success factor for viability of a biobank and/or biobank network.
It is very important that individual biobank managers keep hospital management, ethics committees, and other stakeholders informed about their biobank's progress. Regular progress reports are aimed primarily at institutional and other funders, and management typically to demonstrate return on investment and early impact, but may also be useful to offer feedback to others invested in the biobank initiative (ie, surgeons, nurses, research coordinators, and pathologists). Within the biobank network, they boost morale by documenting gradual progress on all fronts.
Stand-alone biobank personnel may be wary of joining a network, fearing loss of control over their biobank. However, this can often be overcome by elucidation of the benefits and increased resource acquired from assembling a larger sample collection, offering sufficient samples from rare diseases, from subgroups of common diseases (eg, prostate cancer from men under 40 years), and numerous samples for validation of new biomarkers. By joining a network, biobanks may not only aggregate their collections, but also move toward benchmark level collections, optimize their structure and standard operating procedures (SOPs), while developing joint solutions for specific biobank issues, for example, informatics, governance, data sharing, and quality management. A useful approach to integrate these network functions and to ensure accessibility and communication with the network personnel is to develop a publicly accessible user-friendly Web site where knowledge can be centralized and displayed. This may also provide a portal for researchers interested in accessing catalog information about available samples, and can provide information within the site and through links to other sites that provide educational materials and opportunities for basic and advanced biobank training.
Funding
Funding is among the most difficult yet critical issues to confront. The great majority of individual academic institutional biobanks are funded by government, academic institutions, charities, or combinations thereof. Networks are sometimes even harder to support, even though there are unique advantages of a biobank network and biobank networks depend on government funding. However, European governments differ greatly in their funding commitments. For example, Sweden recently committed €40m, The Netherlands €30m, and Spain €6m/year/4 years to establish national biobank networks.
Like most biobank managers, biobank network CEOs hail from academia, where traditionally there has been less emphasis on profit than on product. Thus, biobanks are generally not often profitable. 11 The biobank network's most important resource and greatest cost is its trained personnel and physical infrastructure. An agreed business model must incorporate this. Issues of cost and pricing can be complicated, and it may be best to seek the guidance of an outside expert.
Forming a Network: Top-Down or Bottom-Up?
Since biobank networks are still a relatively new infrastructure, governments typically are slow to participate. This has led to bottom-up network formation in many countries (Ireland, Box 2), although Switzerland and The Netherlands (Pearl String Initiative) have successfully established top-down biobank network models (Box 3). The pioneer of the “network model,” the Spanish National Tumor Bank Network, illustrates both bottom-up and top-down development (Box 4). 12 In Israel the top-down model, envisioned for several years, has not yet been implemented. Instead, independent biobanks have developed bottom-up in the teaching hospitals, and forming a network with harmonized SOPs is now a challenge (Box 5). In Canada, the Canadian Tumour Repository Network (CTRNet) was established through a top-down process initiated by the Canadian Institutes of Health Research–Institute of Cancer Research with the cooperation of provincial biobanks that were already in place (Box 6). Harmonized SOPs and a common database will be used in the new Irish hospital network biobanks, but bringing in additional established stand-alone biobanks will be difficult. Institutional recalcitrance or aversity to change is particularly problematic when dealing with large internationally renowned centers.
SOPs—or “To Know the Road Ahead, Ask Those Coming Back”
Operating procedures must be standardized and harmonized, because a biobank's most important asset is its own human resource network. Sampling from operative specimens (not detailed in international guidelines) requires a standard sampling technique.13–15 The strengths of a biobank network include high-quality samples collected under standardized protocols and linked to a common database, with standardized data elements and definitions, and in the context of a network this is achieved by harmonized SOPs and data, and quality control. Notwithstanding, people are prone to error, and even the most airtight SOPs can suffer lapses due to the human condition, that is, long weekends, illness of a staff member, or a family emergency. SOPs should be robust, easily learned, followed by staff, monitored consistently, and their application recorded (including deviations, where these occur). Although there is no specific ISO normative for biobank accreditation/certification, 16 valuable best practice guidelines have been issued by the relevant organizations.17–20 For managers, it is useful to visit several biobanks, and then to develop SOPs locally in close collaboration with biobank staff. The Irish Network has benefited greatly from viewing the operations of 9 international biobanks visited over 10 years. Experimental data can help convey lessons learned while establishing invaluable personal contacts to aid future discussions and trouble-shooting.
Recently, there has been a move toward development of biobank certification and accreditation programs in France, the United Kingdom, and Canada. When these initiatives come to full fruition, the ability to acquire and provide high-quality samples should be further assured by biobanks that take advantage of the opportunity for certification/accreditation. In Canada, a recent Certification Workshop (January 2011, Vancouver B.C.) organized by the Canadian Tumor Repository Network (CTRNet) revealed a great deal of interest in moving forward with this initiative on the part of funders, REBs, biobankers, and recipient scientists. Adoption of these processes will further improve the perception of biobank quality and reduce anxiety of scientists who wish to obtain high-quality samples.
Human Factors Affecting Specimen Collection
Many people are involved in biobanking. The patient donor is at the center of the hospital biobank network. Consent (if required, depending on local regulations and ethics policy around for example biospecimen anonymization status) is obtained by a physician or research nurse, and patients differ considerably in regard to the information they require. Communication of details regarding patients, surgical schedules, and likely suitability of a specimen for biobanking is pivotal and involves operating room nurses, surgeons, biobank personnel, and pathologists. This requires great commitment by all involved.
Several factors lead to fewer banked samples than anticipated (Table 1). This is due to various factors such as staff holidays, reduced bed availability, occasional outbreaks of infectious disease, deliberate nonsampling of very small tumors, communication lapses, or out-of-hours resections. Operative specimens may arrive in the laboratory much later than expected. The pathologist might be unavailable when the specimen arrives, and another pathologist must be found quickly. Critical sampling of a fresh operative specimen is an essential part of quality management, and must be directed by a pathologist, so as not to compromise pathological determination of tumor diagnosis and stage, and the patient's subsequent treatment. Positive reinforcement of the roles of everyone, including medical staff, data managers and other biobank personnel, the biobank director, hospital information technology staff, human resources, finance staff and senior management, and those in the other network hospitals, is very important.
Factors that lead to decreased number of specimens in tumor banks are hospital-based, specimen-based, and staff-based. The relative contribution of each type of factor is unknown and likely varies with each institution over time in any given network.
Competing Interests Surrounding Sample Release
Institution-based biobanks deal with challenging in-house competing interests. Whereas the philosophy behind biobanking for better healthcare may be altruistic, active participants are not always so. One issue is securing reliable support and adjunct expertise. Clinicians and all healthcare personnel who directly contribute tissue typically are able to offer the highest level of quality effort when provided fair reimbursement for their labor and expertise. Another issue is access to samples and related data. To be fair and offer operational relevance, the sample access policy must be carefully constructed. Formally constituted biobanks with a mandate and the resources to allow access to other users should follow equitable peer review processes. This issue becomes critical when merging multiple standalone sites of a single biobank, or when linking banks together into one network. Questions often under consideration include: How should a tissue allocation committee be appointed? Who should be on the committee? How should the committee review requests? One example may be offered by Spain. Under new Spanish legislation, every application submitted to a biobank is reviewed and approved by 2 external committees, scientific and ethical, whose decisions are final only in the case of a negative evaluation. However, if both committees approve the application, biobank managers are not necessarily obliged to provide the requested samples and data, since the legislation allows for the possibility that the final decision might depend on other local factors.
Recruiting donors and permission to bank their samples is a top priority for every researcher, and this exerts pressure on biobank staff. While the application process must not be too cumbersome, it should be thorough. Researchers' ability to use samples must be determined and, if necessary, tested. The biobank remains custodian of the samples, and samples do not belong to local researchers (even when surgery was performed by their surgeon). Biobanks, as core facilities and biological resource centers, 21 if functioning in a network, fall into the realm of service providers, and are therefore recommended to consider expanding access to include extramural researchers.
Coordinated hospital biobanking requires several key groups of hospital staff to work together. Willingness to collaborate in a patient-focused system that benefits all may direct a cultural change for those still reluctant to adapt. In Israel, hospital ethics committees stipulate that all project applications be submitted by either physicians or dentists. Thus, university-based, nonphysician researchers are required to partner with hospital-based physicians. In this way, new collaborative groups are formed, and researchers, particularly those who are not medical professionals, learn the value of the collections they use, and how by returning results of projects to the biobank they can enhance subsequent projects. Historical motivators for research have included primary and/or well-positioned authorship in publication. One might suspect that aggregated participation in research collaboration will lead to fewer cutting-edge first-authored publications, but this may not be the case. A large-scale biopharma collaboration in Ireland established a pre-treatment patient tissue testing infrastructure, although the 2 participating companies are direct competitors. The collaboration will soon extend to 5 pharmaceutical companies with overlapping rivalries. People, organizations, and businesses can collaborate in strategic alliances and public–private partnerships, even in the presence of competing factors—once they see the advantages from so doing. Networks increase such an opportunity, and anticipated output and advantages are greater than the sum of what each participant could accomplish alone. 22
Biobank Networks and the Public
Interacting with the public and other stakeholders can be very beneficial. Everyone is affected by cancer directly or indirectly, and members of the public constitute a redoubtable lobby group. Fundraising events, formal public meetings, and multi-stakeholder meetings (Marble Arch Group, Dublin 2008, Milan 2008, Montreal 2009) may all prompt media coverage. Radio interviews can potentially reach a large listenership, and are more suitable than short television interviews. Such encounters require preparation and practice. The goal of such events is often related to fundraising, but perhaps more important is that they provide a “feel good” factor for the activity associated with the message.
In Ireland, patient groups are invited to visit the biobank. They gain a better understanding of the process of biobanking, and this promotes ways of working together. Realistic hopes and expectations for personalized medicine are raised, but it is made clear that there are no quick solutions.
General practitioners, as patient gatekeepers, also benefit from increased comprehension from biobanking. Simply explained research results on the Web site or in print media, educational programs on cancer screening, and increased public awareness generally are vital if cancer is to be detected and treated early. With increasing public appreciation of the resultant benefits, biobanking will become accepted as standard of care by all who undergo cancer surgery, with only a minority choosing to opt out. Finally, when biobankers meet cancer patients, both sides gain a unique perspective that neither would realize otherwise.
Summary and Conclusions
Biobank networks are a relatively new development and increasing trend. Currently, all active biobanks experience funding challenges: biobanking lacks a politically high profile and is considered purely a research activity by many health authorities. But in practice, biobanking is becoming standard of care for those with cancer and other diseases, and can serve to bridge clinical care and biomedical/biotechnology research. 5 Biobanking has been listed as “one of the 10 ideas that will change the world, 23 ” but ignorance of its human aspects, logistics, and complexity mitigates against more effective global expansion. Biobankers are pioneers pursuing an important scientific, clinical, and social initiative. However, they face many unnecessary difficulties. One possible solution may well be a wider and more intensive public relations campaign, with the active participation of the multiple stakeholders involved, as illustrated in Fig. 1. The biobank network, biobank personnel, and network hospital staff form a huge Web of collaboration. The number of specimens recruited and disseminated depends on multiple factors related to the hospitals hosting the biobanks, the number, size and quality of specimens, and factors related to hospital and biobank staffing.
It should be remembered that biobanks signify much more than freezers, specimens, or data. Biobank networks are comprised of people working together, trying to make a difference in the lives of patients and improve public health. The focus is primarily on expediting patient-focused research to obtain better survival and quality of life, but researchers, hospitals, industry, and even national economies can be potential beneficiaries. An immediate objective of biobankers is to identify, coordinate, and inspire stakeholders willing to contribute in a positive way to promote biobank development and sustainability.
The new suggested Bio-Resource Impact factor and how it should be implemented is still very controversial. Nevertheless, it might assist biobanks and biobankers in assessing the impact of their work. If biobanks are indeed cited by end-users in their publications, and areas of impact reported, it would improve the ability of biobanks to secure resources and funding.
Collaboration and exchange are key concepts for the success of any biobank network. This article highlights the human face of biobanking because it is the authors experience and firm belief that it is the dedication, labor, and expertise of the people involved who guarantee high-quality work and the success of biobank networks.
Footnotes
Acknowledgments
The authors wish to thank Dr. Fay Betsou, Dr. Gerry Thomas, and Dr. Robert Hewitt for their contribution to discussions in preparation of this manuscript.
Author Disclosure Statement
No competing financial interests exist.