
Abstract
This article discusses the importance of biobanking to health research advancement in developing countries by analyzing the impact of the establishment of a tumor bank at the A C Camargo Hospital, a cancer care and research center located in Sao Paulo, Brazil. For the past 13 years, the human biological samples provided by the tumor bank have been used by investigators to study various types of cancer. We analyze the impact of biobanking in the overall quality of research projects performed at our institution. We also summarize the main findings of these investigations focusing on breast, prostate, head-neck, and gastroesophageal tumors, as well as the lessons learned over these years. We conclude that biobanking should be part of the strategy employed by scientists and research institutions dedicated to the study of human diseases.
Introduction
The A C Camargo Hospital Tumor Bank (ACCHTB) was established in 1997 to provide human tissue samples for the Human Cancer Genome Project, an initiative by the Sao Paulo Research Foundation (FAPESP) and the Ludwig Institute for Cancer Research. For the past 13 years, the ACCHTB has provided samples for the study of various types of cancer. Following patient consent, tissue collection is performed by pathologists and residents of the Department of Anatomic Pathology at the frozen section room, during surgical procedures. Sample selection, registration, and freezing take place within a 30 min window after the surgical specimen is removed from the patient. A blood sample is also obtained and processed in order to obtain and preserve plasma and genomic DNA from leukocytes. Research projects need to be approved by the appropriate ethics committee (local or national) before researchers are allowed to access samples.
Since 2004, the DNA & RNA Bank has concentrated the extraction of DNA and RNA from tissue and blood samples, so that, after quality analysis, investigators receive aliquots of the macromolecules they need in order to perform their research. If tissue samples are requested for laser-capture microdissection (LCM), after obtaining the slides for LCM the tissue is processed for DNA and RNA extraction and the macromolecules are stored in the DNA & RNA Bank. As a result of this new policy of sample acquisition, processing, and distribution, both facilities (the Tumor Bank and the DNA & RNA Bank) formed the A C Camargo Hospital Biobank (ACCHB). To date, approximately 36,000 samples (fresh frozen tissue, FFPE tissue, whole blood and derivatives, DNA and RNA) have been collected from approximately 15,000 patients.
Here, we analyze the impact that research projects had in our institution which used samples collected, stored, processed, and distributed by the ACCHB. We assess the impact the decision of setting up the biobank had in our Post-Graduation Program in Oncology, which was also established in 1997. We also summarize the main findings of the investigations that took place at our institution after the initial effort took place, focusing on breast, prostate, head-neck, and gastroesophageal tumors.
Materials and Methods
Since the Tumor Bank (the first facility of the ACCHB) was created, 42 articles that used human biological samples collected by this facility were published in international literature. However, many other articles that were published during the same period used data and resources derived from the publications that were associated with the creation of the biobank. For example, the tissue array facility, the LCM facility, and the gene array facility were made available to researchers after being introduced to conduct research projects that directly used biobank samples. Therefore, we analyzed, from 1997 to 2010, the total number of publications by ACCH's authors and collaborators, in regional (Portuguese and Spanish languages) and international (English language) journals.
The average impact factor of each journal at the time of publication was measured from 2000 (the year of the first publication that used biobank samples) to 2010. We analyzed the total number of master's dissertations and doctoral theses done by students of our Post-Graduation Program in Oncology (which was established in 1997, the same year the ACCHTB was created), identifying the number of research projects that were designed using human biologic material provided by the ACCHB. We also retrieved the number of research projects that requested access to samples in 2010, and the number of samples that were provided by the biobank.
Results
Along with a significant increase in the number of publications (from 107 in 1997 to 229 in 2010, Fig. 1), and a shift from predominantly regional to international publications (94% of publications in international journals in 2010, Fig. 1), there has been an increase in the average impact factor of publications (which doubled from 2.2 in 2000 to 4.123 in 2010, Fig. 2). With respect to the type of research, there were 11 basic research articles and 31 translational research articles that were published in basic/general journals or in specialty journals (Table 1). Some of the articles that contributed significantly to the establishment of the biobank as a valuable facility for research at our institution were mainly focused on breast, prostate, head-neck tumors, and gastroesophageal tumors, and are briefly described below.

Publications per year (according to the type of publication).
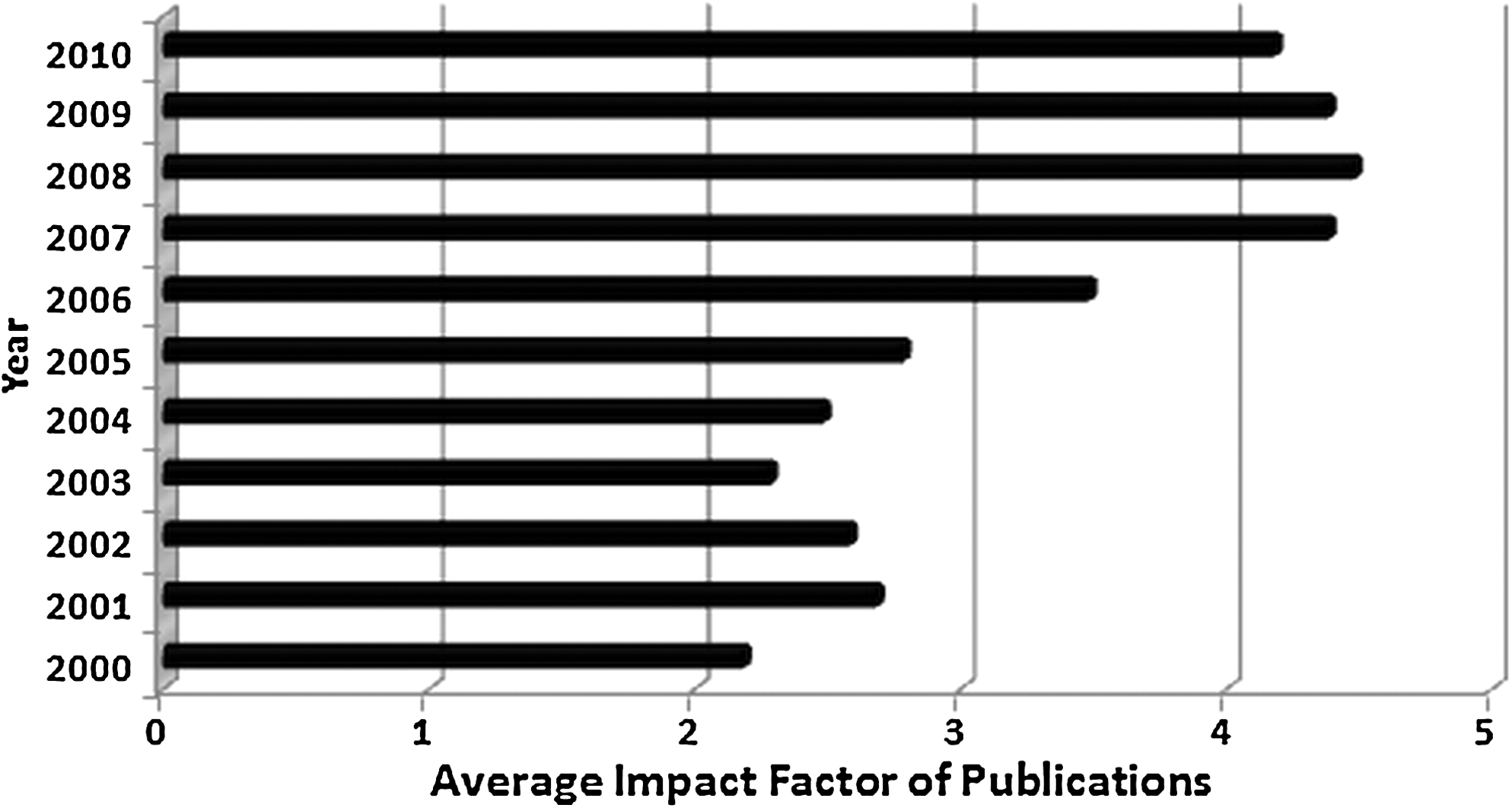
Evolution of the average Impact Factor of publications.
By the end of 2010, 40% (n=142) of the master's dissertations and doctoral theses defended by the students since the beginning of our Post-Graduation Program in Oncology had used human biological material provided by the ACCHB (Fig. 3). In 2010, thirty-six research projects associated with master's dissertations or doctoral theses accessed the ACCHB database, requiring 722 samples from various types of tumors (Fig. 4), which were obtained from 638 patients.
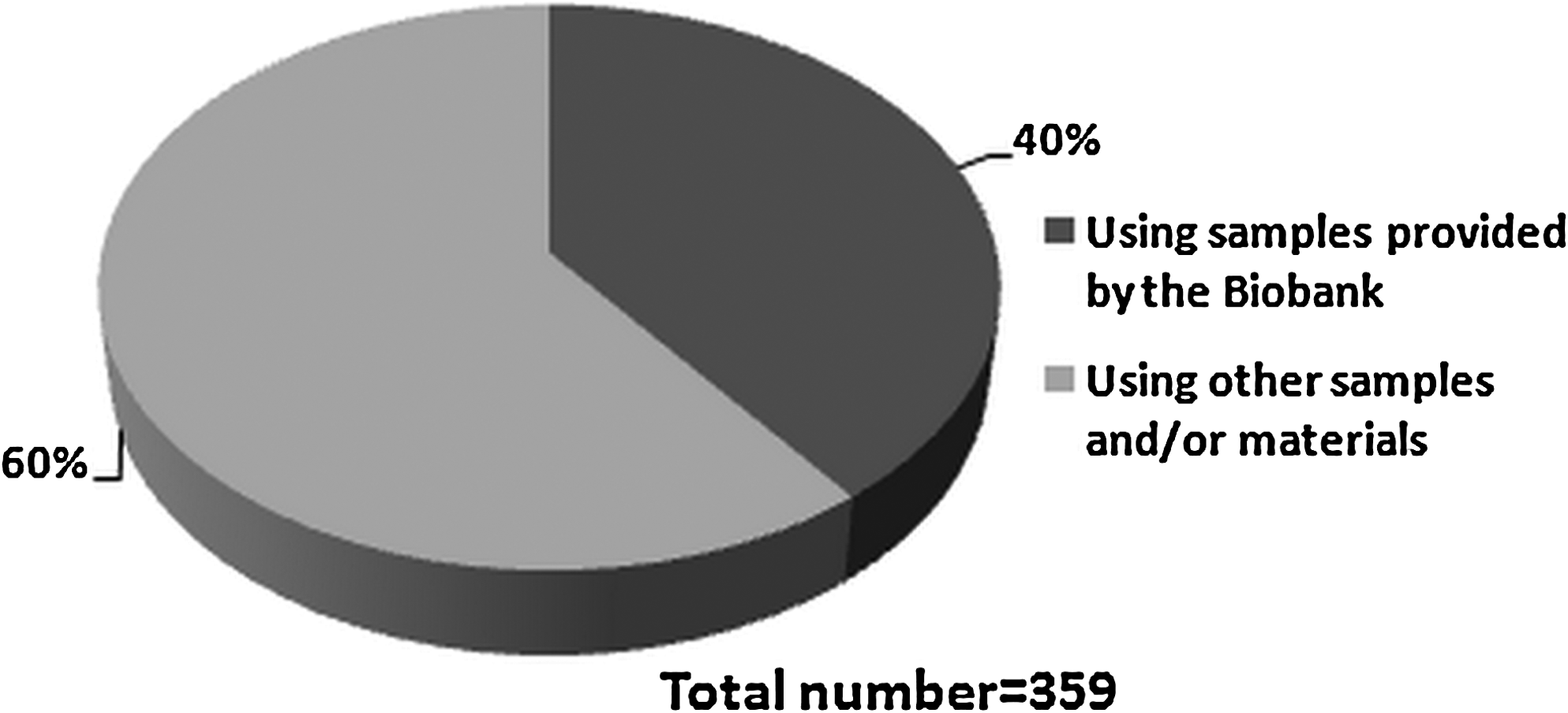
Number of master's dissertations and doctoral thesis defended at the A C Camargo Hospital Post-Graduation Program in Oncology, according to the type of samples/materials used.
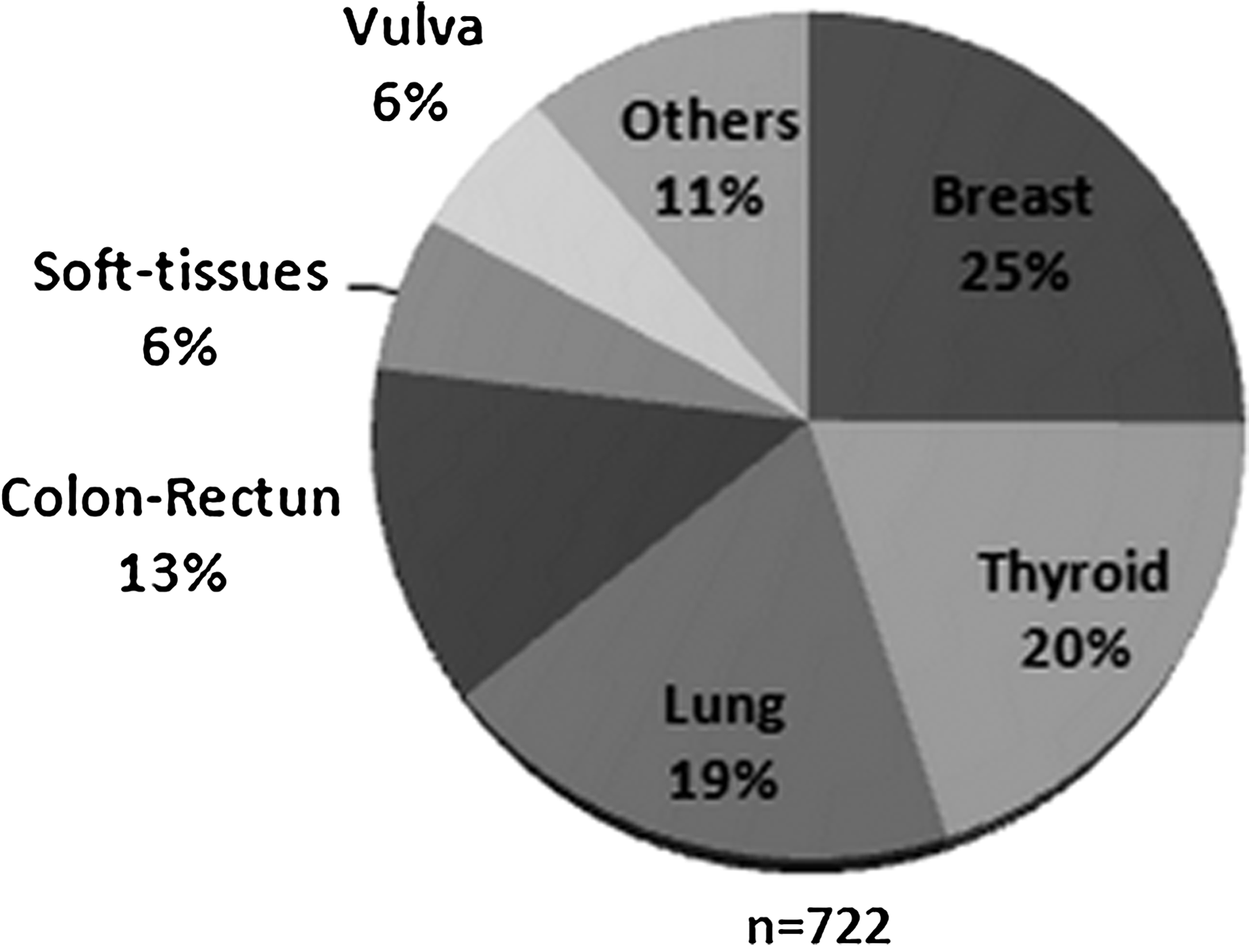
Number of samples provided to research projects by the A C Camargo Hospital Biobank in 2010, according to the different tumor topographies.
Breast tumors: identification of genes associated with tumor progression and response to therapy
Tumor progression
Castro et al. performed a microarray analysis using forty-one fresh frozen breast samples—4 nonneoplastic tissue, 5 pure ductal carcinoma “in situ” (DCIS), 22 DCIS associated with invasive ductal carcinoma (DCIS-IDC), and 10 invasive ductal carcinoma (IDC)—in order to identify genes associated with progression from “in situ lesions” to invasive disease. 3 All samples were provided by the ACCHB. The patients had a mean age of 49 years, and none of them had undergone neoadjuvant treatment before surgery and sample acquisition. Prior to microarray analysis, samples were submitted to LCM in order to obtain pure tumor cell populations from each component (in situ and invasive) and to define the point during the breast tumor progression, in which the cells change the molecular profile to acquire the capability for invading the adjacent tissue. It was demonstrated that most of the alterations in transcriptional profile occur during the transition from pure DCIS to the in situ component of a lesion DCIS-IDC. Cells of the in situ component of DCIS-IDC display a transcriptional profile very similar to the cells of IDC, implying that the molecular program for invasion is already established in the preinvasive lesion. Additionally, an expression signature of 147 genes was able to discriminate cells from preinvasive lesions that share similar morphology but completely different malignant potential. Eight genes (CGI-41, C16orf5, GOSR2, MARK3, LOX, STK25, SULF-1, and TXNL2) were randomly selected for qRT-PCR confirmation, using the initial sample sets, and later, 5 genes were tested in an independent group of DCIS associated with IDC. Three genes (GOSR2, LOX, and SULF-1) exhibited great potential to be used as molecular markers for predicting risk for progression from pure DCIS to invasive disease.
Response to therapy
The fact that not all patients diagnosed with breast cancer experience tumor reduction when selected for treatment with doxorubicin-based regimens prompted Folgueira et al. to design a study to identify genes that could predict a response to this chemotherapy regimen. 4 Tumor samples from patients treated at the ACCH and 2 additional reference centers were obtained at diagnosis (samples obtained from core biopsies) and manually dissected so that only samples composed of at least 80% malignant cells were submitted to microarray analysis. From the 51 patients included in this study, 47% (n=24) had fresh frozen samples provided by the ACCHB. The remaining samples were obtained from patients treated at Instituto Brasileiro de Controle do Cancer-IBCC (43%, n=22) and at Hospital Amaral Carvalho (10%, n=5). The median age of patients was 48 years. By comparing patients who experienced a response to chemotherapy (at least 30% tumor reduction) with nonresponders, the authors identified and validated a set of 3 genes (PRSS11, MTSS1, and CLPTM1) that could correctly classify 95% of the samples.
Koike Folgueira et al. 5 also tried to identify genes that could be associated with tumor resistance to additional cycles of doxorubicin-based chemotherapy, by comparing residual tumors (postchemotherapy) with nontreated tumors considered partially responsive after primary chemotherapy. The ACCHB provided 63% (n=10) of the 16 fresh frozen samples used in this study. The remaining samples were obtained from patients treated at IBCC (31%, n=5) and at Hospital Amaral Carvalho (6%, n=1). The median age of patients was 51 years. By using cDNA microarray analysis and qRT-PCR validation, they found that 2 genes (CTGF and DUSP1) were overexpressed in postchemotherapy tumor samples. This finding may be a reflection of resistance to further administration of doxorubicin-based regimen.
Both studies provided information that can be further explored in order to introduce, in routine diagnosis, biomarkers that could be used to predict response to therapy in breast cancer patients.
Prostate tumors: looking at old data to discover new disease biomarkers
After the description of a new approach to identify human genes through the use of Open-Reading-Frame Expressed Sequence Tags (ORESTES), 6 about a million ORESTES sequences originated from tumor and corresponding nonneoplastic tissue samples provided by the ACCHTB were made available to the scientific community through GenBank. 7 Both studies used RNA extracted from fresh frozen human tissue samples (n=7 for Reference 6 and n=24 for Reference 7). Almost 30% of the sequences did not show similarities with known transcripts at that time and were considered no-match ORESTES. In 2009, Mello et al. 8 reported the construction of a cDNA microarray in order to explore the potential of these no-match ORESTES as tumor markers. Using total RNA extracted from 56 different fresh frozen tumor and normal tissues provided by the ACCHB, they were able to identify tumor-specific RNAs not previously identified as annotated transcripts. Some of these sequences were further explored by real-time PCR in prostate adenocarcinoma and corresponding nonneoplastic tissue and 3 differentially expressed sequences (BQ373258, BF910617, and AW93062) were validated as potential prostate tumor markers. ORESTES sequences BF910617 and AW93062 were aligned with introns of 2 genes, respectively, the KIAA1432 gene and the putative isoform of the RNF217 gene. The expression of both sequences was opposite to that previously described for the KIAA1432 gene and the RNF217 gene (which are highly expressed in normal prostate tissue, decreasing in prostate tumors according to the increase of aggressiveness), suggesting that these genes are repressed in prostate tumors when their correspondent ORESTES sequences are highly expressed. According to the authors, a large number of no-match ORESTES sequences may represent new genes, splice variants, natural antisense transcripts, or noncoding RNAs that could be used as molecular markers, not only in prostate but also in other human tumors.
Head-neck tumors: biomarker discovery and identification of genes associated with tumor progression
Biomarker discovery: gene silencing by promoter hypermethylation
Head and neck squamous cell carcinoma (HNSCC) is an important cause of morbidity and mortality, especially when patients are diagnosed with late stage of the disease. Diagnostic routine could be improved with the introduction of biomarkers of aggressive behavior and prognosis.
Calmon et al. 9 investigated whether gene silencing by promoter hypermethylation could be used for identification of biomarkers in HNSCC. Using HNSCC cell lines FaDu, UM-SCC-14A, UM-SCC-17A, and UM-SCC-38A, the authors combined rapid subtractive hybridization, microarray analysis, qRT-PCR, and bisulfite sequencing to identify highly methylated genes that were investigated in 140 fresh frozen primary HNSCC samples by methylation-specific PCR. All samples were obtained from the ACCHB. The authors observed that 2 genes (CRABP2 and MX1) were highly methylated when compared with lymphocytes from healthy individuals. CRAPB2 [cellular retinoic acid (RA) binding protein] binds all-trans-RA in the cytoplasm, being involved in multiple processes such as apoptosis, cell proliferation, and differentiation. RA and its derivatives have been used to treat many types of human tumors, including HNSCC. The authors observed, using immunohistochemistry in a tissue microarray containing 75 HNSCC samples, that CRAPB2 protein expression is diminished in tumor samples when compared with normal epithelium, and that tumors with negative CRAPB protein expression were associated with decreased disease-free survival, suggesting that CRABP2 could be used as a prognostic biomarker in HNSCC.
Lourenço et al. 10 investigated whether Claudin-7 expression could be associated with clinic-pathological parameters in oral squamous cell carcinoma (OSCC). In order to perform this study, the authors used formalin-fixed and paraffin-embedded tissue samples from 132 OSCC cases from the Department of Pathology of the A C Camargo Hospital. The Claudin-7 transcript was analyzed in fresh frozen tissue samples provided by the ACCHB (25 samples from normal oral mucosa and 36 samples from OSCC). Patients did not receive neoadjuvant treatment before surgery and sample acquisition. Claudin-7 belongs to a family of proteins known to be abnormally regulated in human carcinomas. Lourenço et al. performed an immunohistochemical analysis of Claudin-7 expression in OSCC and found that this protein was weakly or not expressed in the majority of the tumors included in a tissue microarray. Although loss of Claudin-7 protein expression was associated with decreased disease-free survival rates in univariate analysis, it was not an independent predictor of prognosis in multivariate analysis. On the other hand, the authors were able to confirm that Claudin-7 mRNA expression was diminished in fresh tumor samples when compared with normal tissue, and that, in OSCC cell lines, this loss of expression was due to promoter hypermethylation. Additional studies are being performed to explore the role of Claudin-7 gene hypermethylation in OSCC pathogenesis.
Tumor progression
Coló et al. 11 sought to identify groups of genes that could be associated with lymphnode status (N0 vs. N+) and recurrence status in HNSCC. For this study, the ACCHB provided fresh frozen tumor samples from previously untreated HNSCC patients or from patients with recurrent tumors after combined surgery and radiotherapy. Sixty-one samples belonged to the pN0 category, while 20 samples belonged to cases classified as pN+. The authors identified, by microarray analysis, modules containing genes associated with cell survival, cell-cell signaling, and the extracellular region that were repressed in N0 and in nonrecurrent tumors. The authors also identified some genes not previously described in HNSCC, like bone marrow stromal cell antigen 2 (BST2), inhibin beta A (INBHA), and SERPINA3. The regulation of these genes was found to be associated with disease-free survival (BST2) or lymphnode metastasis (INBHA and SERPINA3). Further investigations on the roles of these and other genes in the pathogenesis of HNSCC would help to establish their usefulness as biomarkers of prognosis or tumor progression.
Gastroesophageal tumors
Adenocarcinoma of the esophagus: exploring its origin and relation to Barrett's disease
Gomes et al. 12 also applied the association of microarray analysis and identification of functional modules to study the relationship between Barrett's metaplasia and esophageal adenocarcinoma. In order to perform the study, 71 fresh frozen tissue samples were collected during a 4-year period (2001–2004) and stored at the ACCHTB until RNA extraction, and comprised 39 esophagus and gastroesophageal junction (GEJ) samples (9 normal esophageal mucosa, 6 esophagitis mucosa, 10 Barrett's mucosa, 5 esophageal adenocarcinomas, 9 adenocarcinomas of the GEJ) and 32 gastric samples (6 normal body and antrum mucosa, 5 normal cardic mucosa, 9 intestinal metaplasias, 7 intestinal-type adenocarcinomas, and 5 diffuse-type adenocarcinomas). The authors found that the adenocarcinomas originated from the GEJ and gastric adenocarcinomas had a similar genomic profile, distinctive from that of esophageal adenocarcinomas originated above the GEJ and associated with Barrett's metaplasia, suggesting that adenocarcinomas of the GEJ are in fact originated from the cardia, invading the esophagus through the regional lymphatic drainage. They also observed a closer association of adenocarcinomas of the GEJ with gastric intestinal metaplasia than with Barrett's metaplasia. Their results contribute to the debate on the most appropriate classification for adenocarcinomas of the GEJ.
Gastric cancer: molecular classifiers can be used to distinguish normal from tumor samples and to identify samples of intestinal metaplasia with higher risk of malignant transformation
The definition of intestinal metaplasia as a precancerous lesion in gastric cancer is still a matter of debate. Meireles et al. 13 assessed this question by using a custom cDNA microarray to determine the genomic profile of 99 fresh frozen tissue samples comprising gastric adenocarcinoma (n=28), normal gastric mucosa (n=28), gastritis (n=21), and intestinal metaplasia (n=22). Samples were stored at the ACCHB until RNA extraction. They were able to identify samples of intestinal metaplasia that have a signature resembling that of gastric tumors, after using trios of genes to build classifiers for class distinction. Many of the genes were associated with extracellular matrix functions and were found to have an increased or decreased expression along the cascade from normal to tumor samples. In order to validate these trios of genes as useful predictors of malignant transformation, a large collection of samples of intestinal metaplasia with adequate follow-up of patients needs to be formed.
Discussion
This article aimed at determining the value of establishing a biobank to provide human samples for cancer research in a Brazilian institution. The decision to set up an institutional biobank is not trivial, since it requires the ability to involve different professionals and to spend resources and labor time in a long-term work.14–16 Biobanking is not an end in itself. In order to prove its value, the samples collected by a biobank need to be used in research projects that result in a gain of knowledge on the diseases being studied, which eventually will lead to the development of new treatments, as well as new diagnostic and prevention methods. In the new paradigm of preclinical studies, human biological samples can be used to investigate mechanisms of human disease, so that the data derived from these studies can be validated as biomarkers of diagnosis, disease progression, and response to therapy or provide insights for the development of new treatment approaches.
The studies described above were also beneficial for the improvement of the biobank's infrastructure. For example, the studies on gatroesophageal tumors led the ACCHB to provide the infrastructure for routine collection of endoscopic biopsies at the Department of Endoscopy. Doctors and nurses from this department have direct access to a liquid nitrogen container, cryovials, and a data collection form, so that samples can be collected from patients who provide appropriate informed consent prior to endoscopic procedures. Samples are collected and snap-frozen at the Department of Endoscopy, minimizing RNA degradation or changes in gene expression due to prolonged hypoxia.
On the other hand, this work also allowed us to assess how many studies that requested samples at the ACCHB acknowledged the contribution of this facility in their publications. While all doctoral theses and masters dissertations that used biobank samples acknowledged the contribution of the biobank in their Portuguese versions, explicit citation of the biobank's contribution was present in 26% of the correspondent English-language publications. Since it is the policy of this biobank not to include the staff as coauthors of the publications unless they have contributed to the research projects beyond their normal biobank functions, the institutional mechanisms adopted in order to guarantee the biobank's contribution must be refined. Likewise, an integrated strategy should be put in motion by different stakeholders (biobankers, investigators, journal publishers) in order to establish a minimum of information about biobanking of biosamples used for biomarker discovery.17,18
For the past 13 years, the ACCHB has been providing samples to scientists involved in cancer research. Over the years, the ACCHB has contributed to the increase in the number of research projects done at our institution. The studies summarized above, as well as others not discussed in this article, were responsible for the increase in the quality of research done at our institution, as measured by the increase in the impact factor of publications. Doctors, scientists, students, and collaborators have been able to use state-of-the-art equipment for genomic analysis. Research lines have been established to study different kinds of tumors. The number and overall quality of research projects done at our institution that were accepted for publication in international journals have been significantly increased. Students enrolled in our Post-Graduation Program in Oncology were able to participate in advanced research projects, thereby increasing the quality of master's dissertations or doctoral thesis defended at our institution.
Since the ACCHB has been a pioneer in Brazil in the collection, handling, storing, and tracking of human biological samples in order to perform molecular studies, different initiatives are developed in order to diffuse knowledge and help other institutions in Brazil and Latin-America in building their own biobanks. In order to improve the quality of its processes and protocols, the ACCHB has representatives in ISBER and the Marble Arch Working Group on International Biobanking.
Other institutions and research centers in Brazil, as well as in other developing countries, should consider setting up biobanks to help in studying not only cancer, but other human diseases.
Footnotes
Acknowledgments
The A C Camargo Biobank is supported by FAPESP-CEPID (grant No. 98/14335-2). We thank the pathologists, residents, and technicians of the Department of Anatomic Pathology of the A C Camargo Hospital for helping with the collection and processing of the tissue samples.
Author Disclosure Statement
No competing financial interests exist.