
Abstract
Ethical, legal, and social issues related to the collection, storage, and use of biospecimens and data derived from children raise critical concerns in the international debate. So far, a number of studies have considered a variety of the individual issues crucial to pediatric biobanking such as decision making, privacy protection, minor recontact, and research withdrawal by focusing on theoretical or empirical perspectives. Our research attempted to analyze such issues in a comprehensive manner by exploring practices, rules, and researcher opinions regarding proxy consent, minor assent, specimens and data handling, and return of results as faced in 10 European countries. Because of the lack of comparative analyses of these topics, a pilot study was designed. Following a qualitative methodology, a questionnaire draft mostly including open-ended queries was developed, tested, and sent by e-mail to a selected group of researchers dealing with pediatric biobanking (n=57). Returned questionnaires (n=31) highlighted that the collection, storage, distribution, and use of biospecimens and data from children were widely practiced in the contacted laboratories. In most cases, pediatric biobanking was subjected to national or local regulations covering adult biobanks (n=26). Informed consent was generally given by parents or legal representatives (n=17). Children's opinions were frequently sought and taken into account (n=16). However, minors were usually not recontacted at the age of maturity to express their own choices (n=26). Based on the collected data, dedicated recommendations are needed to govern unique ethical and regulatory issues surrounding pediatric biobanking.
Introduction
During the last decade, there has been increasing interest in ethical safeguards that will allow inclusion of children in research studies intended to find therapies that are appropriate for pediatric use, while protecting the children from potential harms as subjects of the research.
Accordingly, several articles have outlined the ethical frameworks governing pediatric research3,4 and they have concentrated on ethical, legal, and social issues surrounding the use of biospecimens and data derived from children5–7 for clinical or research purposes.
With regard to pediatric biobanking, informed consent, privacy protection, and transfer of data and specimens, research withdrawal has been analyzed as separate topics in the international literature rather than in a comprehensive manner.8,9 Theoretical papers have reviewed ethical positions and/or guidelines concerning the use of pediatric samples and related information for disease or population-based studies,10–12 whereas empirical investigations have focused on the opinions and attitudes of parents and children,13–15 health professionals,16,17 and the general public18–20 toward the inclusion of minors in research using their biomaterials and data.
Our study explored key ethical and regulatory issues concerning pediatric biobanking, such as informed consent, minor assent, specimens and data handling, and return of results through a comparative analysis of practices, rules, and researcher opinions related to this process. In particular, it aimed to analyze (a) how these issues were handled in practice, (b) how they were regulated, and (c) what researchers thought of practices and rules governing pediatric biobanking.
As a pilot study, our research involved a small group of health professionals dealing with the collection, storage, and use of biospecimens and data derived from children in 10 European countries. It followed a qualitative methodology based on a survey mostly including open-ended questions.21,22
Our study aimed to collect preliminary data to contribute to the ethical discourse on regulations of pediatric biobanking.
Methods
A pilot study was designed to allow comparative analysis of practices, rules, and professional opinions related to ethical issues in pediatric biobanking, such as informed consent, minor assent, specimen and data handling, and return of results.
Following a qualitative methodology, a questionnaire mostly including open-ended queries was developed. Open-ended survey questions were preferred to interviews or focus groups, as they are widely recognized to offer greater confidentiality and naturalness to respondents.23,24
The questionnaire draft was finalized with face-to-face interviews and sent by e-mail to a group of researchers handling pediatric specimens and data. No monetary or other incentives were offered. The study was approved by the Ethics Committee of the Institution promoting the survey (Scientific Institute “Medea”–La Nostra Famiglia).
Sample
A group of researchers involved in pediatric biobanking was formed on the basis of existing lists of biobanks at the time of the study. Because of the lack of specific official registries of children biobanks, names and addresses of eligible researchers were first identified in accordance with the “Catalogue of European Biobanks,” a list of collections of biospecimens and data collected from adults as well as from children, available on the website of the Biobanking and Biomolecular Resources Research Infrastructure—BBMRI. 25
Based on this, 27 (n=27) contacts of researchers were identified. This list was then supplemented with contacts of researchers (n=22) working in biobanks that were not reported in the “Catalogue of European Biobanks” but were associated with major pediatric hospitals on a national level.
Finally, names of candidate participants were provided by contacted health professionals.
Overall, 57 (n=57) researchers working in biobanks handling samples and data derived from children in 12 European countries were identified and invited to take part in the survey (Table 1). Questionnaires were sent together with letters of invitations presenting the study. Contacted researchers were asked to distribute the questionnaire to colleagues, if appropriate. Letters of invitation and subsequent contacts were managed by e-mail from March to June 2010.
Questionnaire design and finalization
A questionnaire draft organized in 3 sections exploring practices, rules, and researcher opinions related to pediatric biobanking was developed. Selected topics were identified by referring to the international literature addressing ethical issues pertaining to the collection, storage, and use of biospecimens and data from children, such as proxy consent, minor assent, privacy protection, and return of results.6,9,17
To finalize the questionnaire, 9 structured interviews were conducted with health professionals involved in biobanking processes. Based on collected data, the questionnaire was revised. A first section relating to social and demographic data of researchers taking part in the survey was added to gather information that could be helpful for further analyses. A fifth section, left free for comments, was included to stimulate spontaneous reflections on the analyzed topics from contacted researchers.
Because of the different nationalities of respondents, the final version of the questionnaire was written in English (Fig. 1).
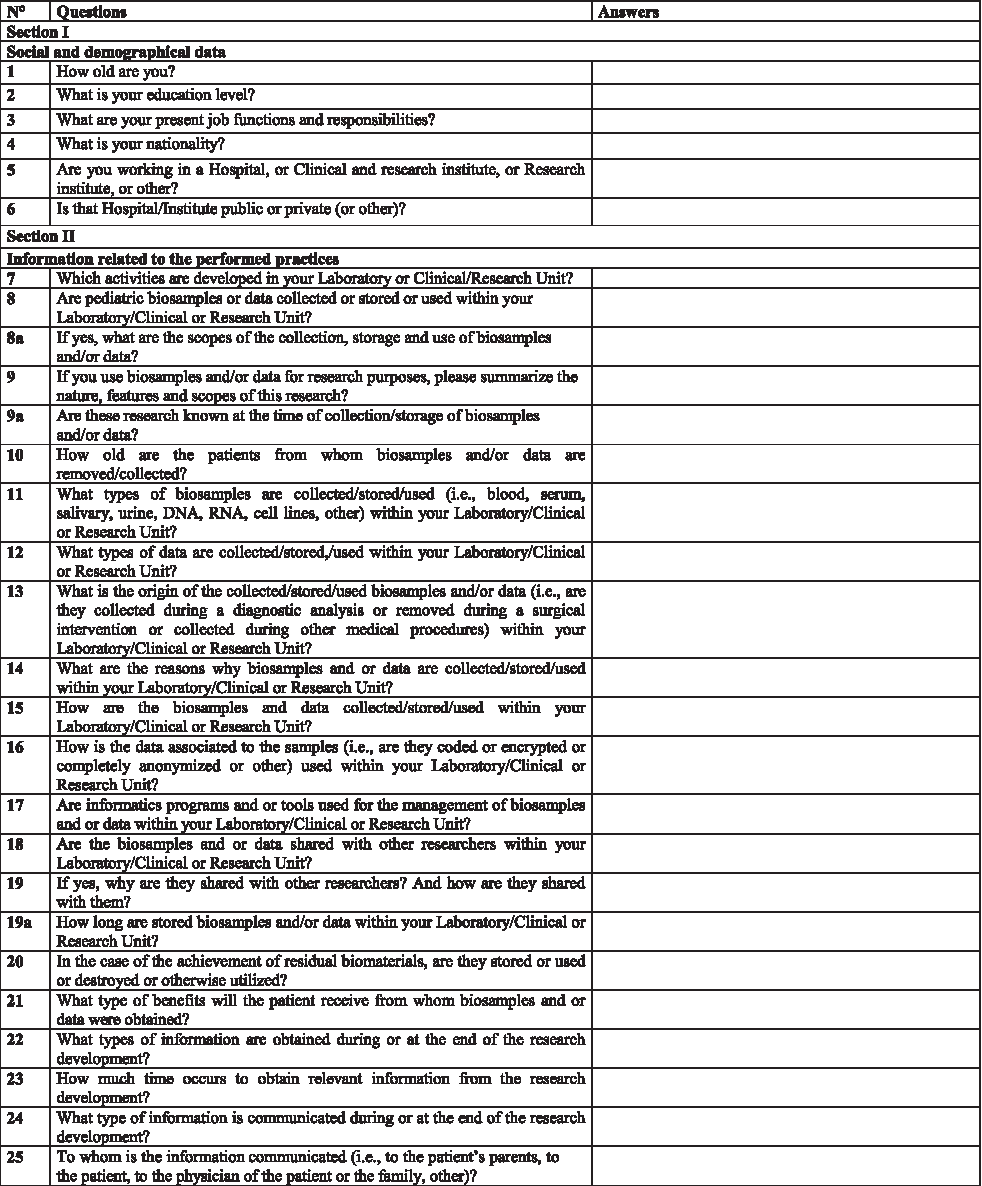
Questionnaire form used to explore practices, procedures and researcher opinions related to key ethical, legal and social issues surrounding pediatric biobanking.
Results
Completely filled out questionnaires were received from 31 researchers (n=31) working in biobanks distributed in 10 European countries (Table 2).
Ten people replied that they were unable to complete the questionnaire because of pressure of work and 2 replied that they were retired.
The response rate varied between countries. A number of questionnaires were obtained from researchers working in Italian biobanks, but no surveys were received from researchers working in biobanks based in Norway and Sweden. This was probably due to the different ways to administer the survey on a local level. However, the main aim of the study was to cover the existing diversity in handling key ethical and regulatory issues concerning pediatric biobanking and report same representative examples in the European region, rather than to obtain exhaustive data from each country.
According to a content analysis methodology,26,27 collected data were categorized in the following groups: (1) features and scope of pediatric biobanking, (2) decision-making processes, (3) samples and data handling, and (4) return of results.
Data related to analyzed practices, rules, and researcher opinions are reported later. Representative quotations are enclosed in parentheses for credibility and confirmation. 26
Features and scopes of pediatric biobanking
Collected specimens and data were recruited by patients whose age ranged from 0 to 18 years (n=14) or from children and adults not over 35 years old (n=11). In few cases, samples and data were derived from heterogeneous groups including children, adults, and elderly patients (n=6).
Collected or stored samples differed widely in typology, including blood, serum, DNA, RNA, saliva, lymphocyte cells, bone marrow, cell lines, muscle, skin, breast milk, postmortem fixed or frozen brain tissue, and waste materials derived from surgical or diagnostic treatments.
Collected data mainly referred to clinical information and especially included genetic information.
Biospecimens and data were generally collected or stored for genetic diagnosis and research (n=17) or exclusively for genetic research (n=6). Cohort studies, biomonitoring, neonatal screening, and hematopoietic stem cell use for transplantation were also practiced. The specific attention for genetic analyses was stressed by respondents, reporting that pediatric biobanking was intended to “discover gene features such as mutations or deletions,” “study correlation between genotype and phenotype,” and “analyze data on risk factors, protective factors, and eventually the treatment of disease.”
The purposes for which biospecimens and data were collected or stored were generally known at the time of sample collection or storage (n=20). In particular, the use of residual samples and related information (known as “secondary uses”) was, in most cases, well defined at the time of recruitment.
In most cases, policies dedicated to pediatric biobanking were not adopted (n=23). Instead, international, national, or local guidelines pertaining to adult biobanking were extended to pediatric biobanking.
However, the importance of pediatric biobanking-based studies and the necessity to perform them in accordance with specific regulations were recognized by a number of responses (n=27). Researchers pointed out that “pediatric biobanking is the only way to increase diagnostic knowledge on pediatric diseases,” “it is useful and important to get insight into mechanism and biomarker development,” it is helpful “to improve knowledge on rare pediatric diseases and to link research groups,” and “necessary for disease risk assessment in childhood.”
A number of researchers also acknowledged the necessity to develop specific guidelines governing these researches (n=14).
Decision-making processes
In many cases, informed consent to collect, store, and use biospecimens and data derived from children was given by parents or legal representatives (n=15) or by parents only (n=7).
In a number of cases (n=16), children opinion (as assent or dissent) was sought and taken into account under the condition that minors were “able to understand” or “mature enough to assent.” In other cases, the opinions of minors were not considered (n=8) or “were rarely considered.”
The ability to make decisions autonomously was recognized according to different age ranging from “over 8 to 10 years,” “over 8 to 12 years,” or “over 11 years.”
In most cases (n=26), minors were not recontacted on becoming adults for the following reasons: “we do not have the opportunity to tackle this circumstance,” “to date we had no patients who have become adults,” “it is impractical,” and “we generally do not recontact children because in our country children tend to move their domicile and so recontacting them requires us to use resources for which we have no funding.” In 2 cases, patients were recontacted once they became adults or above 12-year olds.
Responses to the question “How do you think pediatric biobanking should be managed and regulated?” highlighted the fact that most researchers agreed on the use of regulations dedicated to pediatric biobanking, but they had different opinions on the nature of them. Few professionals referred to the use of national or international laws, whereas many of them (n=18) suggested that guidelines, policies, best practices, or standard operating procedures should be put in force at European as well as national or local level. In particular, some researchers stressed the need for using strict and rigorous rules (n=2).
Organizations entitled to put in force regulations governing pediatric biobanking were identified in multidisciplinary groups including physicians, researchers, biologists, or experts from the scientific community and parents, patients or patient organizations, ethics or scientific committee, and government.
Samples and data management
Apart from the case of stem cells collected for transplantation, specimens were generally handled as reversibly anonymized. According to the terminology used by the European documents, 28 we refer here to “reversibly anonymized” samples by meaning those that are not associated to personal information of patients whose samples are collected. Gathered data also showed that a large number of samples were coded (n=18), but few of them were encrypted.
Handled data were mainly coded and only 1 code was attributed to them (n=18).
In many cases, biospecimens and related data were shared outside the biobanks or laboratories for research purposes (n=24). All researchers reported that the adoption of material transfer agreements is necessary for specimens and data sharing within or outside the storing institutions.
Return of results
For these issues, only 18 of 31 respondents replied. They reported that diagnostic information resulting from the undertaken studies were communicated to parents (n=9) or to patients and parents (n=5) at scheduled visits. Diagnostic data were also communicated to health professionals by letter (n=4). Research results were communicated to parents 8 or to parents and health professionals by letter or newsletter. 6 They were also returned to patients on demand. 4 In no cases did patients derive any direct benefit from the participation in studies using their biospecimens and/or data. No standardized procedures on the return of result were adopted in any case.
Most researchers expressed a preference to keep a link with patients from whom biospecimens and data were stored to provide them and/or their relatives with relevant information on ongoing studies (n=17).
Discussion
This is the first analysis of key ethical and regulatory issues related to the collection, storage, and use of biospecimens and data derived from children addressing unique aspects of pediatric biobanking, such as informed consent, minor assent, specimens and data handling, and return of results through a comparative investigation of practices, rules, and researcher opinions regarding this process.
As a pilot survey, it involved a small group of health professionals handling biospecimens and data collected from children in biobanks distributed in 10 European countries.
Survey results offered an interesting picture of the state of the art of pediatric biobanking in the European region and they provided helpful information for interpreting the current debate on this topic.
Based on collected data, grouped in 4 categories, namely, “features and scope of pediatric biobanking,” “decision-making processes,” “samples and data handling,” and “return of results,” it emerged that the collection, storage, distribution, and use of biospecimens and information derived from children were largely practiced in contacted biobanks with the aim to improve knowledge on pediatric diseases. In particular, “the discovery of gene features as mutations or deletions,” “the study of correlations between genotype and phenotype,” and “the assessment of diseases risks in childhood” were considered typical aims of pediatric biobanking.
With regard to the handling of specimens and data from children, queried researchers reported that, in most cases, no dedicated regulations were applied to govern this process but laws and guidelines addressing the collection, storage, and use of samples and information derived from adults were extended to the collection of specimens and data derived from children.
Regarding this point, most researchers recognized the need to develop specific policies for governing pediatric biobanking on a European or national level and many of them identified an adequate model for pediatric biobanking regulation in “soft law” instruments.
These results confirmed data reported in previous studies. First, the opinion of researchers related to the importance, necessity, and usefulness of pediatric biobanking confirmed the point of view expressed by other scientists. Indeed, some scholars argued that genetic research could equally be conducted on adults as on children, 29 whereas others claimed that pediatric genetic research is necessary. 30 In particular, they stressed that specimens and data collection should start as early as possible to study a number of diseases affecting children. 18
Second, the lack of specific policies for pediatric biobanking and the need to adopt regulations dedicated to this process were in accordance with data reported in previous research8,12 and topical policy forum on pediatric biobanks. 10
A wide correspondence between survey results and the literature was also found out with regard to “decision-making processes.” In accordance with other studies,6,7,17 our survey showed that the informed consent to collect, store, and use biospecimens and data derived from children was usually given by parents or legal representatives. Minor opinions were mostly sought and taken into account. However, they were generally not engaged in the decision-making process related to the use of their biomaterials and/or data in an active way. In particular, concerned children were generally not recontacted at the age of maturity to express their choices regarding the stored samples and information.
Finally, information related to “specimens and data handling” and “return of results” provided interesting data with regard to the privacy protection of children involved in biobank-based research.
Survey results reported that samples and data collected from minors were mainly handled as linked anonymized. 28 They also showed that this practice was considered adequate by a number of researchers willing to keep a link with children or their relatives to communicate to them relevant information on studies undertaken with the use of their specimens and data.
In the current debate, the identifiability of specimens and data collected from pediatric patients is controversial. 10 Some authors suggest that an irreversible anonymization is adequate to remove risks for privacy breaches, 31 whereas others believe that even if the risks for personal harm is minimal after permanent anonymization, results of genetic research may lead to group stigma. 32 Others, again, argue that samples and data can be kept coded, where personal identifiable information can be retrieved by using 1 or more keys. 6 With regard to these conflicting positions, the referred practice to use specimens and data derived from children as reversible anonymized and the opinion of researchers willing to keep a link with patients or their families to communicate relevant information resulting from undertaken studies could indicate a suitable approach for the privacy protection of children involved in biobanks.
Despite the aforementioned aspects, we acknowledge that our study has several limitations. As a pilot and qualitative survey, it reported practices, rules, and opinions of a numerically limited sample of researchers. Moreover, our study used a sample of researchers identified on the basis of an existing official list of biobanks, including both adult and children collections. Finally, it considered the opinions of health professionals only.
Further analyses exploring key ethical, legal, and social issues associated with pediatric biobanking within a broader sample including representatives from health professionals, patients, families, and advocacy organizations could provide comprehensive information for developing specific policies. Moreover, changes in the sample composition based on new or updated data taken out from specific lists of pediatric biobanks could contribute to form selected groups for further studies, particularly large-scale studies addressing ethical and regulatory issues associated with pediatric biobanking. Finally, interviews and/or focus groups can offer greater understanding of motivations underlying opinions and attitudes of all of the stakeholders involved in pediatric biobanking processes helpful to identify appropriate multidisciplinary strategies to govern this field.
Footnotes
Acknowledgments
The authors are grateful to Robert Hewitt and Lisa Miranda for helpful comments and suggestions. This article was written within the context of the project “La disabilità neurologica del paziente bambino: individuazione e sviluppo dei problemi etici e giuridici inerenti al pediatric biobanking,” supported by a grant from the Italian Minister of Health, “Ricerca Corrente 2010.”
Author Disclosure Statement
No competing financial interests exist.