
Abstract
Stakeholders are individuals, groups, or organizations that are affected by or can affect a particular action undertaken by others. Biobanks relate to a number of donors, researchers, research institutions, regulatory bodies, funders, and others. These stakeholders can potentially have a strong influence upon the organization and operation of a biobank. A sound strategy for stakeholder engagement is considered essential in project management and organization theory. In this article, we review relevant stakeholder theory and demonstrate how a stakeholder analysis was undertaken in the early stage of a planned research biobank at a public hospital in Norway.
Introduction
Stakeholder Analysis and Project Management
If you fail to plan, you plan to fail
Organizational changes, such as setting up a new biobank, are generally organized as a project. Projects can be divided into five stages; (i) initiation, (ii) planning, (iii) execution, (iv) monitoring and controlling, and (v) closing. The project stages are not static entities proceeding just in one direction. If necessary, the project plan must be adjusted. In some instances, it might even be necessary to go back to the initiation stage and adjust the overall goals of the project. The main task in the initiation stage is to develop a basis document for the project (Table 1). In the planning stage, one has to develop the plan from the initiation stage into more solid documentation. In complex projects, the planning stage is usually broken down into two parts; a concept stage and a pre-project stage. Independent of project complexity, the planning stage should, as a minimum, address the issues listed in Table 2.
Proper stakeholder management is essential in projects, 6 and assumed major stakeholders are often identified in the project initiation stage, while a proper stakeholder analysis is undertaken in the following planning stage.
Stakeholder Analysis: Theory and Practice
A stakeholder analysis usually includes the following five tasks (modified from Ref. 17); (i) identification, (ii) attributing values, (iii) prioritizing, (iv) devising a plan for engagement, and (v) monitoring. In the following we will describe these five tasks and illustrate each step of the process using a biobank project from our own practice as an example.
Example: Background
All individuals in Norway have a unique 11-digit identification code being used in all public registries. All health care providers are legally required to submit identifiable health data to a number of national health registries (eg. Birth Registry, Cancer Registry, and Death Registry). It is therefore possible to track information on every individual from birth to death.
Akershus University Hospital is an 800-bed public hospital in South-Eastern Norway. The hospital serves as a local hospital for 460,000 people. In 2009, there was an initiative to establish a biobank as a common resource for future cancer research at the hospital. It was proposed that the biobank should be operated by the Department of Pathology. In response to this proposal, the department established formal guidelines for research projects and biobanks in 2010. The department then started work on a preliminary business plan in early 2011. It was decided that the plan had to be based upon the hospital's overall strategy plan which emphasizes research based upon prioritized patient groups, collaboration between hospital and general practitioners, and collaboration between hospital and external organizations. It was also decided to downscale the project and focus on an organ specific project with established track record in the organization. Based on these considerations, the department decided to focus on a long-term, multi-disciplinary project on colorectal cancer.
A working group with members from the Departments of Gastrointestinal Surgery and Pathology, and one external advisor was established. As a national guideline on the treatment of colorectal cancer was published in 2010, it was decided that the plan had to be in line with recommendations in this guideline.
18
One of these recommendations is a 5-year follow-up plan after curative resections. Many hospitals have chosen to let general practitioners take care of some or all of these controls. Based on all of the considerations listed above, the group proposed the following general principles regarding the project:
• Encompass both quality improvement and research aspects. • Engage both departments within the hospital and general practitioners. • Exploit information from compulsory national health registries. • Engage with patients with respect to long-term quality-of-life data. • Base the project on informed consent. • Data and biological material collected should be considered an “open” resource for the research community. Realizing the extensive number of stakeholders involved, the working group decided to undertake a proper stakeholder analysis.
Identification of stakeholders
Rhenman 19 was one of the first to visualize the relationship between an organization and its stakeholders (Fig. 1). In practice, the identification can be done quite simply by a brain-storming session involving the project team. It is usually beneficial to have this list of potential stakeholders verified by someone outside the project team itself. As the list can potentially be very long, it is common practice to group stakeholders into categories containing persons/groups/organizations of similar nature. Working in a hospital environment, we find a generic model with the following eight stakeholder groups to be useful; (i) own organization (the hospital), (ii) hospital owner, (iii) patients, (iv) public bodies, (v) political bodies, (vi) media, (vii) funders, and (viii) others.

Illustration of the relationship between a company and its stakeholders (modified from Ref. 19).
Example: Identification
Using this generic model, the working group identified a number of stakeholders and structured them into eight groups (Fig. 2).
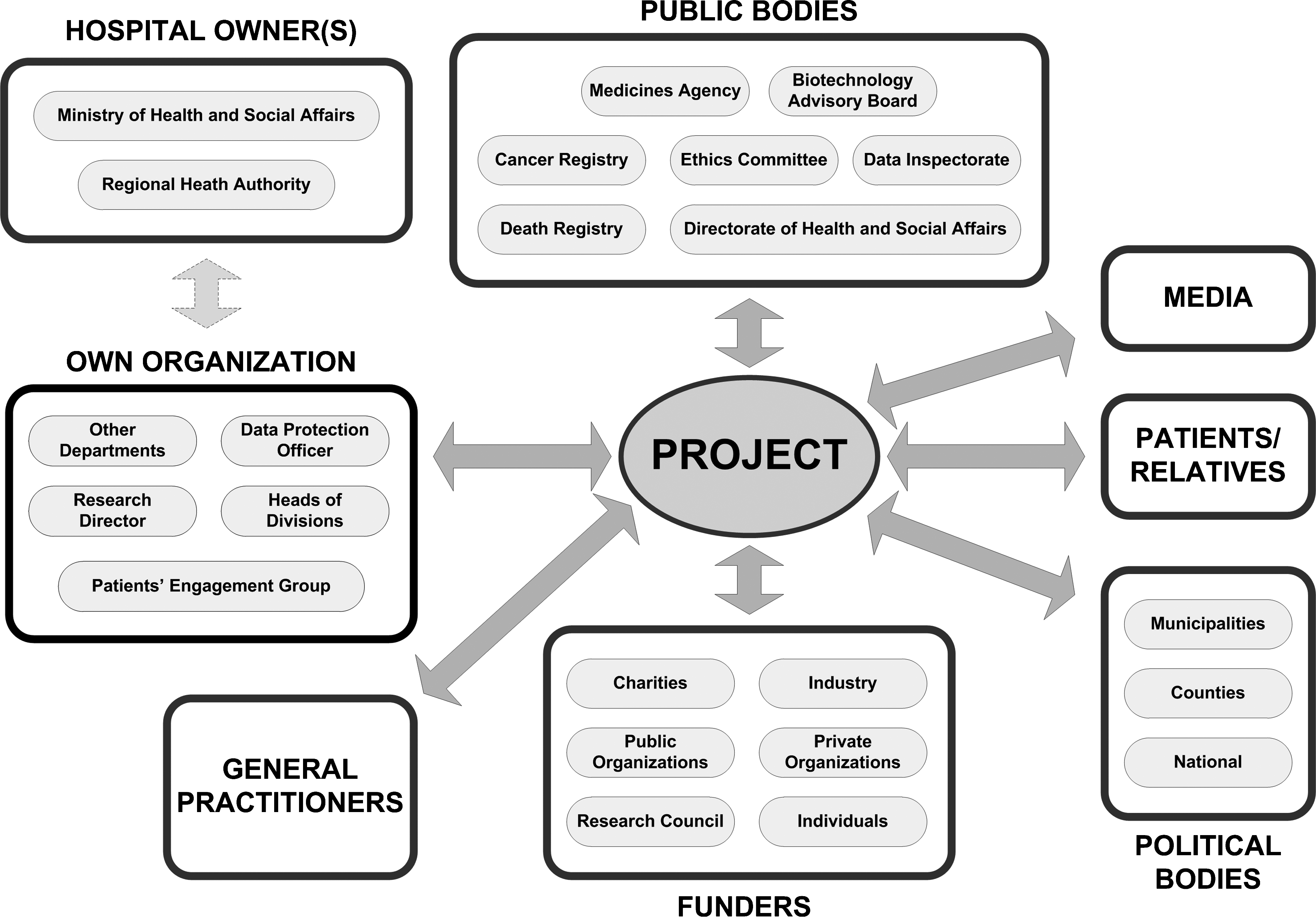
Identified stakeholders for a long-term, multidisciplinary project on colorectal cancer.
Attributing values to stakeholders
Some kind of relevant attribute must be associated to each of the stakeholders in order to relate to them in a meaningful way. In 1981, Mendelow 20 introduced a “power-dynamism matrix” for this purpose. This was later modified by Johnson and Scholes 21 to the “power-interest matrix” (Fig. 3). The attributes high power/low power and high interest/low interest are allocated to each of the stakeholders in order to assess how they can influence upon the project. Mitchell and coworkers 9 have proposed a more complex classification of stakeholders based on (i) power to influence, (ii) the legitimacy of each stakeholder's relationship with the organization, and (iii) the urgency of the stakeholder's claim on the organization (Fig. 4). Murray-Webster and Simon 22 proposed a similar classification system, but based on the attributes (i) power to influence, (ii) their interest in the project, and (iii) their attitude to the project (“back or block”).

Illustration of a “power-interest matrix” for attributing values to stakeholders. The four corresponding strategies for engagement are also shown (modified from Ref. 21).
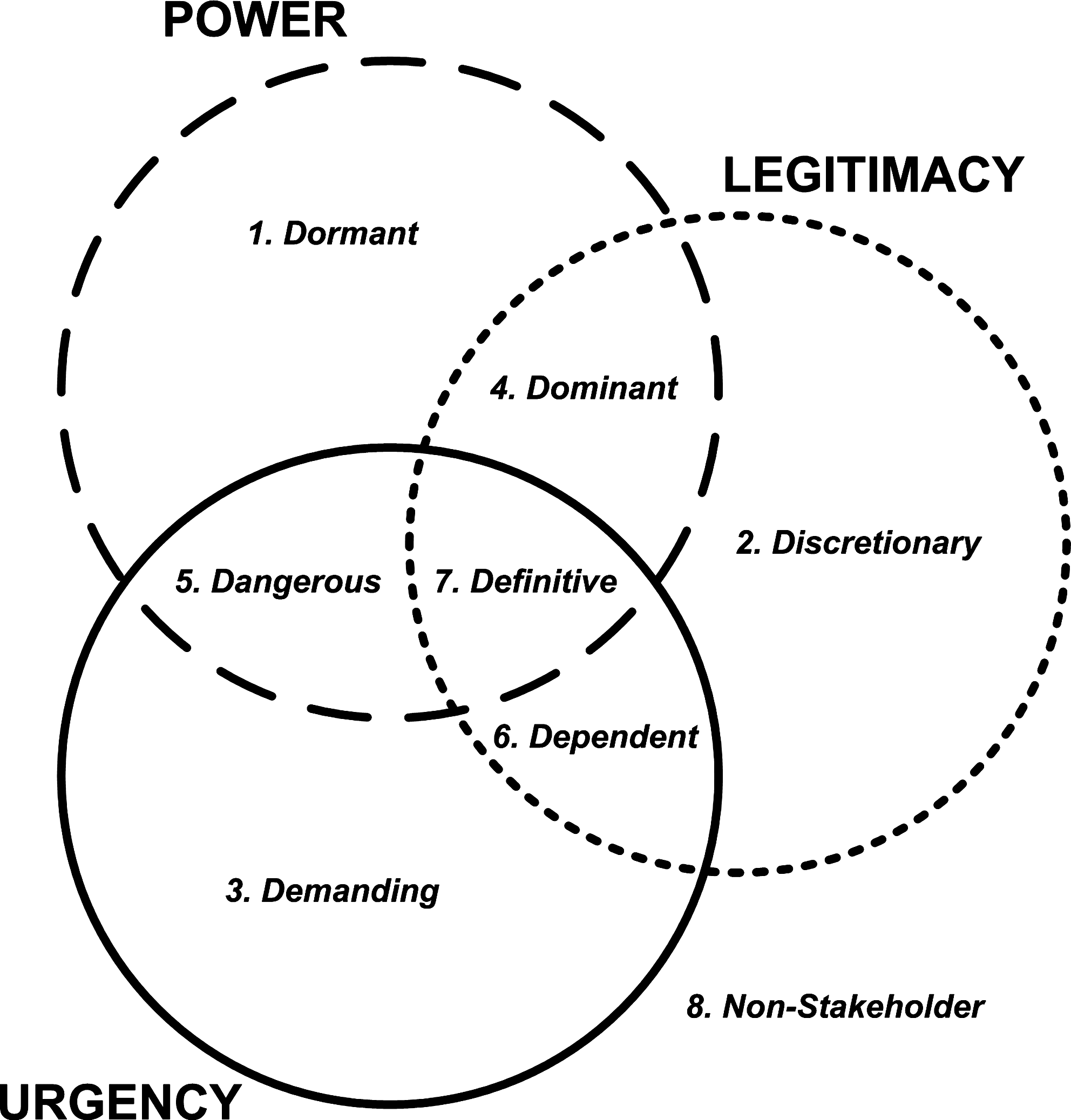
Classification of stakeholders based on power to influence, the legitimacy of each stakeholder's relationship with the organization, and the urgency of the stakeholder's claim on the organization (modified from Ref. 9).
Example: Attributing Values
The working group decided to use a “power-interest matrix” for attributing values. This method is easy to undertake in practice, and was considered good enough in the initiation phase. It was also decided to limit the value attribution to the group level, and not break it further down to individuals or individual organizations. The values attributed to the eight groups identified (Fig. 2) are shown in Figure 5.
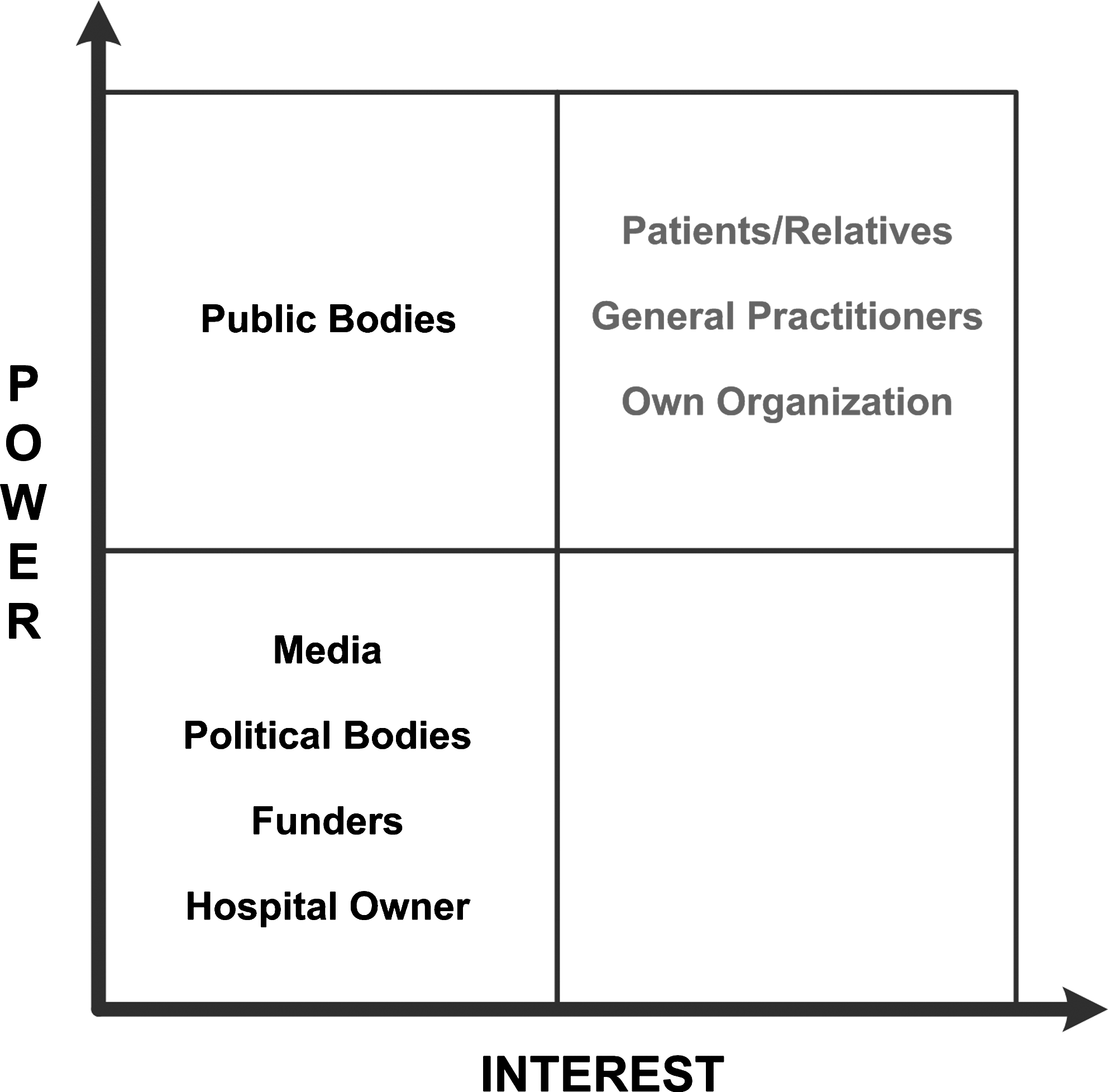
Power-interest matrix for the eight groups of stakeholders identified for a long-term, multidisciplinary project on colorectal cancer (see Fig. 2).
Prioritizing stakeholders
Independent of how one classifies the stakeholders, one has to make a prioritized list in the end. Prioritizing can be done based on a classification system as illustrated in Figures 3 and 4, or stakeholders can be grouped based on assumed high/moderate/low impact. When prioritizing, one should also reflect on how this information should be handled, and how stakeholders might react on being put into a particular “power group.” Not everyone might like to be put into a low interest/low impact group, and this could actually result in a change of interest and impact.
Example: Prioritizing
The working group decided to target the three groups of stakeholders deemed to have the combination of high power and high interest (own organization, patients/relatives, and general practitioners) as the project had limited resources and was in the initiation phase.
Engagement of stakeholders
Some stakeholders will clearly have more interest and ability to affect a project than others, so it is beneficial for the project to establish some form of interaction with these. Friedman and Miles 23 have devised a 12-step ladder model for overall stakeholder management and engagement (Fig. 6). Although steps such as “manipulation” and “therapy” appear cynical, the model in itself does not advocate such steps. The model only illustrates how an organization might appear to behave if observed from the outside.
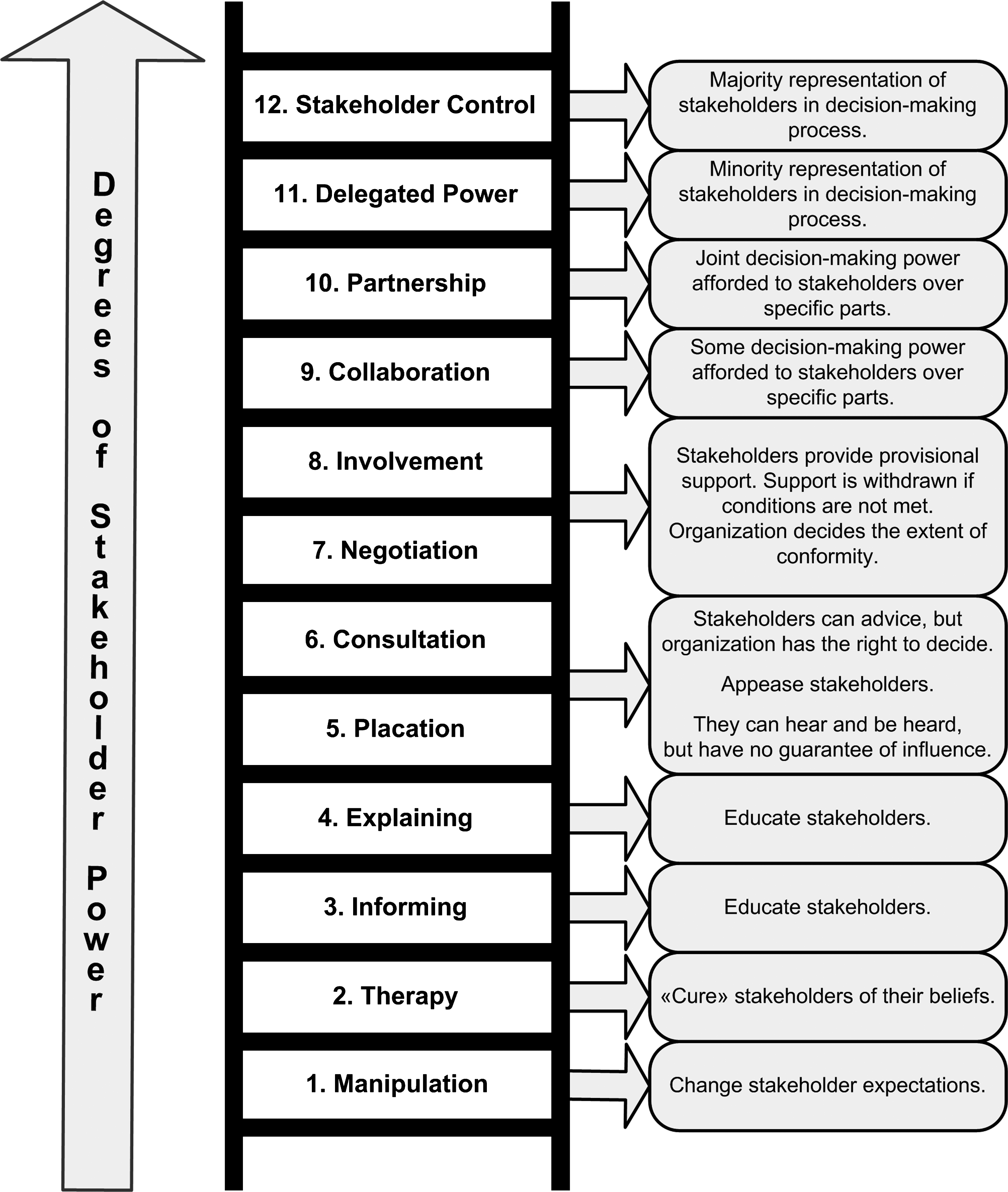
Model of stakeholder management and engagement (modified from Ref. 23).
Example: Engagement
The working group considered transparency about the project and a general feeling of partnership essential in order to succeed. The group accordingly opted for an engagement plan with high degree of stakeholder power (see Fig. 6). Formal letters were sent to patient interest groups, elected representatives for general practitioners in the county, and relevant stakeholders in the hospital. It was stressed that the project was in an early initiation phase, that a formal “go-ahead” had not been granted yet, and that the working group welcomed collaboration and input from all stakeholders. Representatives from the three stakeholder groups were also invited to an open meeting where the working group and external experts were to discuss the initiative.
Feedback was received from representatives of all three groups. Most of the feedback was positive with suggestions for improvement, but some responses also touched upon “ownership-issues”. Within the hospital, the initiative resulted in a high-level decision on the establishment of a formal working group.
Monitoring the stakeholders
As in the traditional “Plan-Do-Study-Act”-model of quality improvement, one has to establish a monitoring system on how the stakeholders actually react upon the project and the engagement plan. Such monitoring might be passive, or an active program might be established whereby the organization actively seeks out the information. If stakeholder attributes change, one has to evaluate whether this should lead to a change in the engagement plan, or ultimately, a change in the project plan.
Example: Monitoring
As the project was just in the initiation phase and the hospital had not formally decided that the project should move ahead, the working group decided to not establish a monitoring program at this stage.
The entire stakeholder analysis, including written documentation and drafts of letters to the three stakeholder groups, required approximately 40 man-hours.
Discussion
We have demonstrated how a stakeholder analysis was undertaken in the initiation phase of a biobank project to ensure adequate involvement with major stakeholders. Such an analysis is theoretically and empirically founded upon sound organization and project management theory. In real life, neither sophisticated equipment nor deep theoretical knowledge is required in order to do such an analysis. The one thing required though, is a will to face possible future negative factors and risks, a will to engage with people who might have different views, and a will to change own objectives and/or ways of acting if deemed necessary to reach overall goals.
Several well-known biobank initiatives and projects have engaged with stakeholders during the planning phase. The National Cancer Institute in the United States is sponsoring the development of a cancer Human Biobank (caHUB) as a national center for biospecimen science and standards (http://cahub.cancer.gov). Researchers 16 and academic and pharmaceutical industry leaders 15 have been consulted during the planning phase. In the period 2008–2011, the European Commission funded the preparatory phase of a pan-European Biobanking and Biomolecular Resources Research Infrastructure (BBMRI) (http://www.bbmri.eu). Part of the project was to establish a stakeholder's forum to collate “… the input and requirements of the broad and heterogeneous stakeholder community of BBMRI, comprising patients, clinicians, funding organizations, associated project partners, industry, and users.” How the project will move from preparation to operation is currently not clear. In the United Kingdom, the Department of Health, the Medical Research Council, and the Wellcome Trust have funded the establishment of the UK Biobank, a medical research project on the impact on health of lifestyle, environment and genes in 500,000 people aged 40–69 years (http://www.ukbiobank.ac.uk). As part of the planning phase, the opinions of the general public, primary care health professionals, industry, and other stakeholders were sought. To our knowledge, none of these projects have published data on stakeholder analyses undertaken.
The identification of stakeholders and the acquisition of their opinions are not always easy. A group such as general practitioners will have various levels of interests and opinions. Even the most (scientifically) well designed study may hit unforeseen stumbling blocks. In 2001, the Norwegian Institute of Public Health began a large research study on childhood diabetes involving 100,000 children. The study also included genetic testing. The project was well advertised through media and had all (presumed) necessary formal approvals. However, in 2006 one general practitioner raised concerns about ethical and legal aspects of the study based on the experience from one family attended in her practice. She also pointed out that general practitioners, who had to handle families affected after being informed about a positive genetic test, had not received relevant information about the project. After a lengthy public and political debate, the study was stopped in 2007 because the genetic testing was found to be in violation of Norwegian legislation. However, because of high-level political decisions, the study was allowed to use data already collected.
What can be learned about stakeholder engagement from this story? One of the main points of a stakeholder analysis is to look upon the project from the outsiders' point of view. 5 As each individual in Norwegian society is supposed to have one allocated general practitioner, the planning phase of the study should have taken into account that families being informed about a positive genetic test result for diabetes would get in touch with their family physician. Foreseeing this, general practitioners should have been targeted in an engagement plan. In his article “The Rise and Fall of a Biobank: The Case of Iceland”, Pálson described how the initially widely supported project gradually met increasing resistance from a number of stakeholders—and finally collapsed. 2 Many of the examples given in his article underscore the viewpoint that appropriate management of stakeholders is one of the best ways to avoid project failure.4,5
Time and economic restraints in a project may force a project manager to skip or short-cut an assumed resource-consuming stakeholder engagement. However, as exemplified by the Norwegian diabetes study and the Icelandic biobank project, this greatly increases project risk. Even if an initial stakeholder analysis is done and major stakeholders are engaged, type and duration of engagement chosen might affect the outcome. An open invitation to potential stakeholders to attend a meeting where an almost finished project plan is presented, scores very low on the stakeholder engagement ladder (see Fig. 6). In our opinion, real collaboration and partnership with major stakeholders from the early planning phase is advisable.
Footnotes
Author Disclosure Statement
Drs. Bjugn and Casati disclosed no conflicts of interest.