
Abstract
In the last decade, vitrification protocols to preserve human ovarian tissue have been regularly reported, even more often than the protocols developed for large mammals, such as ruminants and nonhuman primates. In order to facilitate the use of domestic ruminants (cows, goats, and sheep) and nonhuman primates as animal models, application of similar protocols as used for human material is performed. Next to it, the addition of indispensable or exclusion of avoidable compounds in the vitrification of human ovarian tissue should be tested in such experiments with animal models. The objective of this mini-review is to summarize the current protocols used for the vitrification of ovarian tissue and to evaluate the vitrification methods in humans, nonhuman primates, and domestic ruminants.
Introduction
Though mice and rats are not the most appropriate models for large mammals regarding ovarian tissue cryopreservation, such approach helped to elicit further understanding of the preservation of female fertility. The first report of ovarian tissue vitrification in large mammals was published by Isachenko et al., 4 who performed vitrification of human ovarian tissue. More recent studies involving other large mammals, such as nonhuman primates and ruminants, have been carried out. In 2005, live births were reported after vitrification of hemi-ovaries, followed by autotransplantation in sheep. 5 Although such success has not been repeated, as yet, in other large mammals, this is a confirmation that vitrification of ovarian tissue is a very promising technique. In contrast to slow freezing, which can not be applied in whole organs, vitrification eliminates the risks of intracellular formation of hexagonal ice-crystals. 6 Furthermore, when wild mammals are found dead in the zoo or in remote areas, the ovarian tissue can be immediately preserved by vitrification without the need of electricity or complex equipments. In the present review, we summarize the advances and challenges involving the vitrification of ovarian tissue from primates and domestic ruminants in order to preserve PFs.
Animal Model or Direct Application?
Cryopreservation of ovarian tissue is an important tool to preserve the fertility of women prior to cancer treatment onset, 7 as well as to preserve animal biodiversity. 8 In both cases, domestic ruminants (sheep, goats, and cows) and nonhuman primates can be used as animal models to develop and optimize cryopreservation protocols. However, based on a compilation of publications with respect to vitrification of PFs at MEDLINE, most of the studies have been performed using human ovarian tissue.
Table 1 summarizes information on the vitrification of ovaries and ovarian fragments of primates (human and nonhuman) and domestic ruminants from 2003 up to 2011. The increased interest in ovarian tissue vitrification is shown by the high percentage (45.5%, i.e., 15 from 33) of the ovarian studies that have been published in the last 2 years. From 2003 to November 2011, 51.5% of the vitrification studies with ovarian tissue were accomplished with human tissue, while ovine and bovine ovarian tissue were second and third choice, representing 18.2% and 15.1% of the studies, respectively. In addition to these studies, there are two reports (6.1%) that used caprine ovarian tissue, and three (9.1%) applying nonhuman primate ovarian tissue.
It is well known that preservation of female fertility encompasses most of the ovarian tissue cryopreservation studies. However, screening of protocols used for the cryopreservation of animal tissues is indicated before introducing these protocols for the cryopreservation of human ovarian tissue into clinical practice. Replication is crucial to evaluate an experimental condition, and the ovarian tissue from different donors may respond differently to the vitrification procedure, which, for example, is due to tissue consistency, size, and donor age. In the studies involving ovarian tissue vitrification, the mean number of replicates varied from 6 (monkeys) to 15 (goats), while the number of experimental repetitions ranged from 3 (human) to 35 (sheep) trials per experiment. The ovarian tissue was collected from young and adult donors, and the size of the vitrified tissue varied from 0.5 mm3 to the whole organ (ovary) (Table 2). Therefore, it is difficult to compare studies performed within the same species and among different ones, demonstrating that there is no standardized guideline to perform studies on the vitrification of ovarian tissue.
Although every laboratory may have a standard procedure to test vitrification, an effective network among clinicians/researchers involved in the vitrification of ovarian tissue from human and animal models would help to define criterion regarding the size of ovarian tissue, the reproductive age of donors, the vitrification and the analysis methods, to develop a consistent evaluation system of the vitrification protocols.
Cryoprotectants, Supplements and Vitrification Methods: Miscalculated Risks
Before vitrification, ovarian tissue is permeated with intracellular cryoprotectants such as ethylene glycol (EG), dimethyl sulfoxide (DMSO), propylene glycol (PROH), glycerol (GLY), or other compounds alone or in combination. To this end, ovarian tissue exposure/perfusion to cryoprotectants has been performed for just some seconds 9 or for long periods, for example, for 45 minutes.10–12 Although exposure time depends on the temperature, tissue size, cryoprotectant type and concentration, the methods of tissue permeation, and cryoprotectant removal, we must bear in mind that cryoprotectants are generally toxic to the cells and, when used at high concentrations as in vitrification procedures, they may represent a risk of osmotic stress and genotoxicity. Cytotoxicity is the major problem caused by vitrification solutions 13 and has been indicated as the most important barrier to successful vitreous preservation of complex tissues.14–16 As highlighted by Aye et al., 17 cell exposure to high concentrations of EG and PROH induce chromosomal damage in eukaryotic cells.
Composition of a vitrification solution is variable from a single intracellular cryoprotectant (e.g., EG alone),4,18 to complex mixtures of these compounds (e.g., DMSO and PROH) 10 either or not supplemented with serum, sugars, or other compounds used to reduce osmotic shock. The chemistry of intracellular cryoprotectants and their toxicity have been reviewed 19 and will not be considered here. Emphasis, however, must be given to the vitrification cocktails and additives used for ovarian tissue vitrification. Cryoprotectant cocktails are used to improve vitrification. According to Vajta and Nagy, 20 combining low concentrations of different cryoprotectants decreases the specific toxicity of an individual cryoprotectant. However, it is crucial to determine if the compounds present additive or synergic characteristics, which either reduce or increase cytotoxicity. 21 These latter authors have shown that (i) combining cryoprotectants may increase toxicity synergistically, and (ii) due to negative osmotic effects, addition of nonpermeating solutes increases the cytotoxicity of vitrification solutions. Although a combination of cryoprotectants may lead to synergic toxicity, live births in large mammals were reported after vitrification of hemi-ovaries from sheep in a solution containing 2.62 M DMSO+2.60 M acetamide+1.31 M PROH+0.0075 M polyethylene glycol. 5 However, a malformed animal was born, and when the same solution was used to vitrify whole ovaries, no follicular survival was observed, while most damage was oocyte nucleus related. 22 Regarding nonpermeating solutes, Celestino et al. 23 have indeed reported the ineffectiveness of the addition of 0.5 M sucrose on the preservation of bovine PFs morphology during vitrification. More consistently, Bao et al. 12 showed that addition of sucrose to the vitrification medium was deleterious to bovine PFs. Sucrose is the most used nonpermeable cryoprotectant followed by trehalose (Fig. 1).
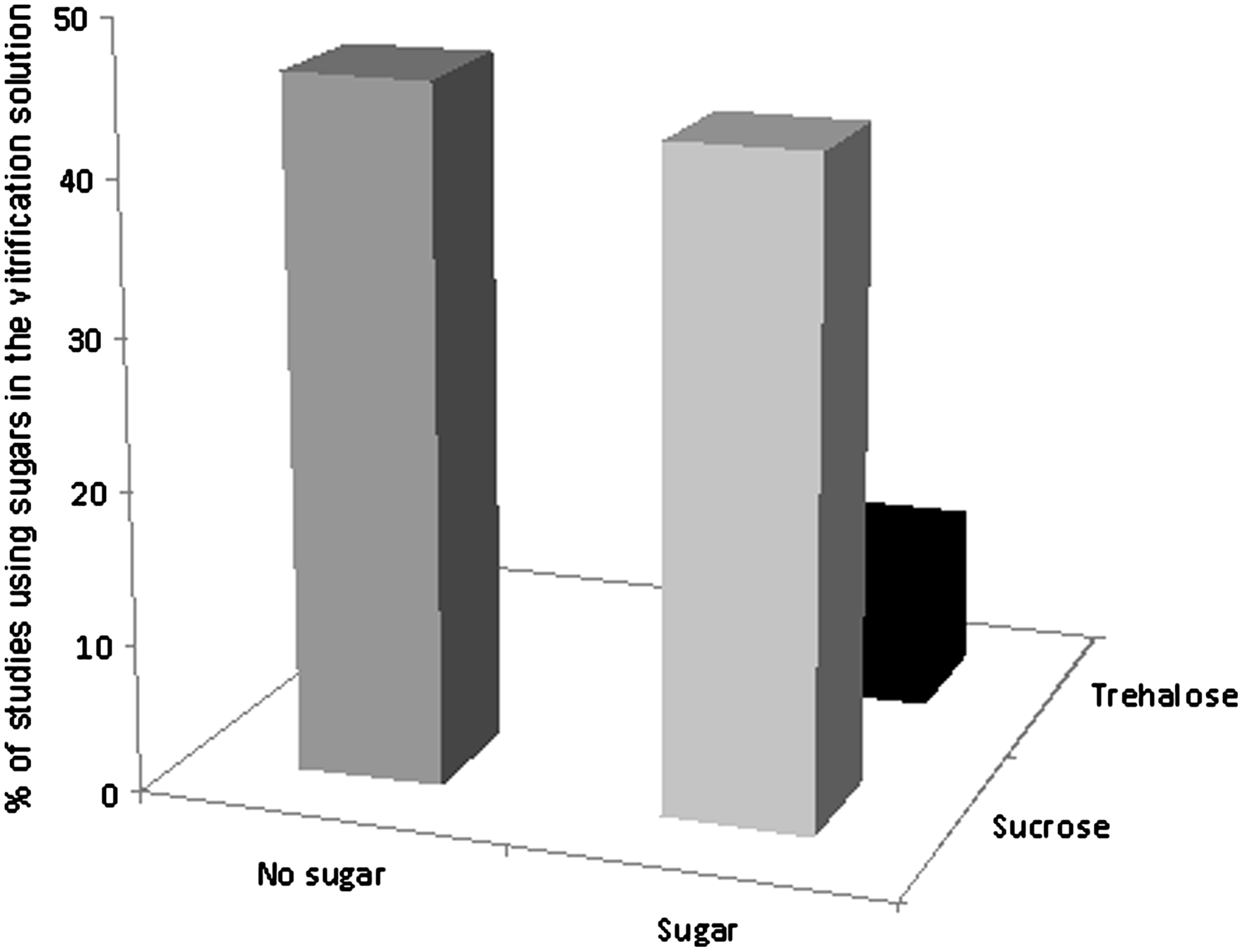
Mean percentages of studies reporting vitrification of ovarian tissue in the absence or presence of sugars (sucrose or trehalose).
Bovine serum, another additive commonly present in cryopreservation solutions, has been replaced by human serum albumin or synthetic serum substitute in most human ovarian tissue vitrification protocols.10,11,24–31 The most recent vitrification protocols studied in monkey also did exclude bovine serum from vitrification solution,32,33 as well as those performed in sheep.5,22,34–37 Figure 2 shows the decline of the use of bovine serum in vitrification protocols in the last years. Use of animal serum, commonly fetal bovin serum (FBS), is of particular concern in the entire cryopreservation process. Although FBS is rich in compounds that may support cell survival and is regulated by guidelines for production and handling, it does not totally eliminate uncharacterized substances, or even the risk of transmitting infectious agents or other pathogens. 38 Therefore, elimination of animal-derived additives, such as serum or egg-yolk from the vitrification solution, remains the best approach.
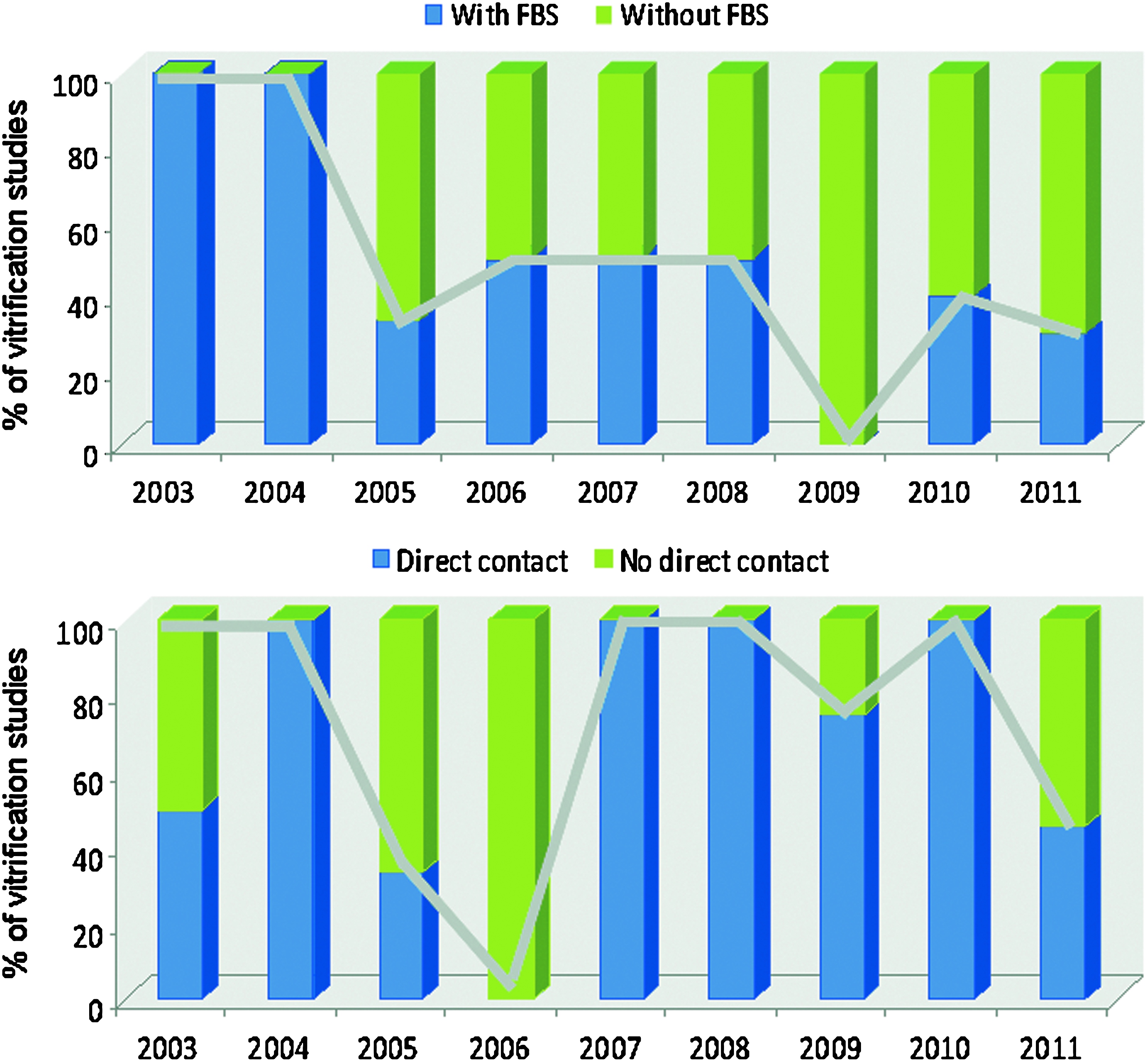
Mean percentages of studies reporting vitrification of ovarian tissue using solutions supplemented with fetal bovine serum
Risks of tissue contamination, however, are not limited to the presence of serum in the vitrification solution. There is some debate whether filtered liquid nitrogen is free from virus and prions. It is well known that various infectious agents may survive to adverse conditions, such as extreme low temperatures, including those in liquid nitrogen (−196°C). Therefore, although many vitrification systems can be successfully used to preserve ovarian tissue, the risk of direct contact of this tissue with liquid nitrogen becomes imperative to develop a safe cryopreservation protocol and germplasm banking. Although supplementation of the vitrification solutions with FBS has been diminished, the use of closed systems is not, as yet, a common pattern. Most of the new vitrification techniques, which are successful to maintain follicular morphology and viability, consist in the use of open systems. Fortunately, the return to the use of closed devices has been observed in 2011 (Fig. 2).
What Does a Successful Ovarian Tissue Vitrification Mean?
Although there are many techniques and cryoprotectant solutions available, the assessment of ovarian tissue vitrification relies mostly on the maintenance of follicular morphology. However, preserved cell morphology is not a guarantee of gamete functionality. Therefore, morphology preservation should not be considered as a major criterion of success. As an alternative, vital staining of follicles through Trypan Blue exclusion or viability fluorescent markers (e.g., calcein-AM and ethidium homodimer) is applied. According to Amorim et al., 39 Trypan Blue staining has the same accuracy of classical histology to detect normal follicles. However, the Trypan Blue exclusion test will depend on the person who counts the number of positive cells, and unstained follicles are not a guarantee that cells are free of apoptosis.
The use of fluorescent markers to detect esterase activity in the ooplasm (through a positive calcein immunoreaction) and membrane integrity (through a positive ethidium homodimer immunoreaction) 40 is a more accurate method to evaluate follicular cell viability. Nevertheless, integer membrane and esterase activity are not exclusion parameters for degenerating cells in the near future, and these temporary survival analyses of the follicles do not assure their ability to grow.
Biochemical parameters such as hormonal assays4,5,10,25 or lactate dehydrogenase assay41,42 do contribute in the investigation on the follicular functionality. However, investigation of follicular development remains the best method to evaluate the success of ovarian tissue vitrification. Although IVC (in vitro culture) for 2 hours 39 or even 42 days 43 has been used to determine follicular survival after vitrification, there is no effective protocol for the complete in vitro development of primordial follicles from large mammals. Therefore, ovarian tissue auto- or xeno-transplantation is preferred as a direct method to detect follicular functionality. In this context, it has to be remarked that the ability of a follicle to develop will not always end up with an oocyte able to be fertilized. Moreover, if fertilized, embryo development and risk of offspring with malformation may be experienced. 5
There is a paucity of studies on the up- or downregulation of genes encoding growth factors involved in the follicular survival and development after vitrification of ovarian tissue, or simply after exposure of ovarian tissue to vitrification solutions. As reported on MEDLINE, in this regard only one study has been published, describing the expression of GAPDH. 10 However, as GAPDH is a so-called stably expressed gene, information regarding genes related to ovarian tissue function after vitrification is not available. In a recent study (data not yet published), we have observed that nonhuman primate ovarian tissue exposed to vitrification solutions shows ooplasm vacuolization, which was related to downregulation of superoxide dismutase and upregulation of a protein related to endoplasmic reticulum stress.
Finally, in 78% of the studies, only follicles were evaluated after ovarian tissue vitrification, whereas stromal cells and vessel integrity have been neglected. Only in a few studies have these two compartments gained some attention (16% and 6% of the studies referred to stromal cells and vessel integrity, respectively). A summary of methods used to evaluate ovarian tissue quality after vitrification is presented in Figure 3. The main results obtained are shown in Table 3.
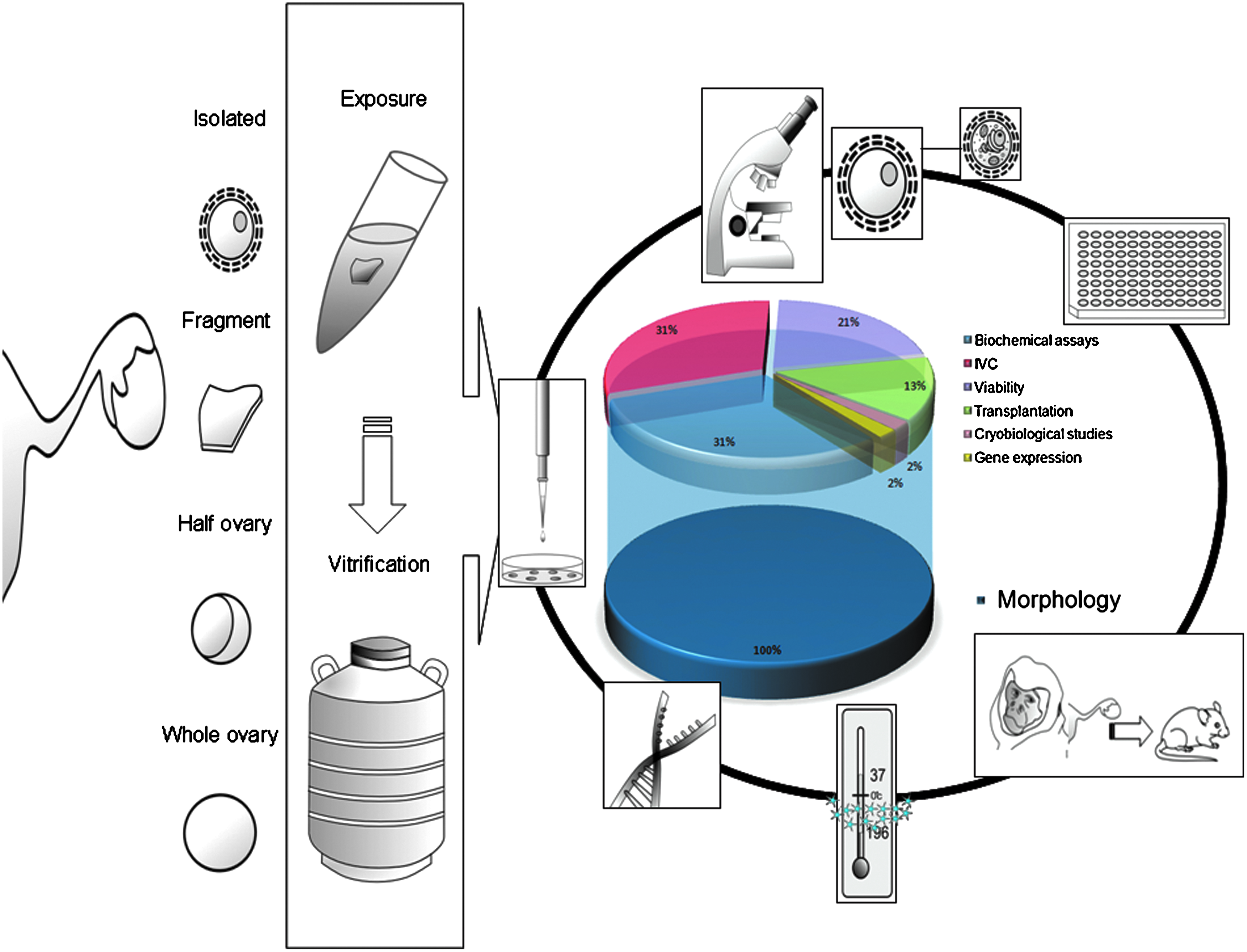
A summary of the methods used to evaluate ovarian tissue quality after vitrification. A color figure is available in the online version of this article at www.liebertpub.com/bio
AMH, anti-müllerian hormone; E2, estradiol; GAPDH, glyceraldehyde 3-phosphate dehydrogenase; IVC, in vitro culture; P4, progesterone; PEG, polyethylene glycol; PVP, polyvinylpyrrolidone; ROS, reactive oxygen species.
Conclusions
Many vitrification protocols have been developed and are readily available to be applied in human clinical practice and animal reproduction centers. However, several issues related to vitrification safety and risks need to be controlled. Any cryoprotectant, as a chemical compound, may be considered a hazard, which means that high or low risks due to cryoprotectant exposure must be evaluated. It is essential to exclude possible contaminants during vitrification, such as serum or contact with liquid nitrogen. Success of vitrification protocols must be evaluated following concrete parameters other than be limited to morphological issues. The implementation of tests using animal models such as domestic ruminants must be considered, but protocols must fulfill the same safety guidelines proposed to human and nonhuman primates.
Footnotes
Author Disclosure Statement
This research was supported by CNPq and CAPES. R. R. Santos is supported by CNPq (project 483439/2009-6), Brazil. L. Santana is supported by a grant from CAPES. The authors reported no competing financial interests.