
Abstract
Biobanks offer translational researchers a novel method of obtaining clinical research materials, patient data, and relevant ethical and legal permissions. However, such tissue collections are expensive to establish and maintain. Current opinion is that such initiatives can only survive with core funding from Government or major funding bodies. Given the present climate of financial austerity, funding agencies may be tempted to invest in fast-return research projects rather than in maintaining tissue collections, whose benefits will only become apparent in much longer timescales. Thus, securing additional funding for biobanks could provide a valuable boost enabling an extension of core services. Here we suggest that using biobank expertise to offer contract services to clinicians and industry may be an alternative approach to obtaining such extra funding.
Introduction
The benefits of such an operation are difficult to quantify and each stakeholder will have different expectations. For example, epidemiological information is of substantial macro-economic benefit for the entire population, but of minimal benefit for individuals; 3 conversely, personalized information can provide immediate micro-economic benefits to the patient. Ideally, there would be a straightforward investment/cost-benefit/profit assessment, similar to the ‘health impact assessment gateway’ of the UK's Department of Health. 4 However, for biobanks embedded within universities or hospitals, 5 costs are current while the benefits are very much in the future.
One of the major issues in mapping and improving the funding/output balance of a biobank, which can arise even before operations commence, is the lack of a clear operational model which impedes the evaluation of its activities. 6 A second obstacle is the lack of standardization, even among facilities with a similar scope. While it has been suggested that such standardization may be both ‘unaffordable and unfeasible’, 7 steps have nevertheless been made towards harmonization of international legislation, 8 and of issues involved in sample exchange, compatibility, and usage.9,10 There has, however, been less debate of economic operational models. Given that funding for biobanks is increasingly difficult to obtain, the need to develop additional novel funding streams has become of increasing importance. In this article, we describe how the Infectious Diseases BioBank (IDB) at King's College London has evolved an economic operating model that may be of interest to others.
Mapping the Stakeholders
A major issue in developing an economic operating model for biobanking is the dissimilar requirements of different stakeholders. In a private setting, the major stakeholders providing the initial investment need to realize some return on their investment within a short time-frame. This is perhaps the single most significant reason why some biobanks have experienced difficulties in becoming sustainable. 11
The issue is more complicated for a public institution because of the multiplicity of stakeholders (e.g., funding organizations, clinicians, researchers, and patients groups), each with different perspectives and expectations. Within a narrow typological frame and only in relation to data-sharing, Foster and Sharp identified a minimum of fourteen stakeholders. 12 A workable matrix that can help in mapping, but not ranking, both the stakeholders and the operational activities has been proposed. 13 In practical terms, the returns of a clinical biobank are still predicted to outweigh the initial investment, as in the case of the National Cancer Institute's projections for the centralized cancer Human Biobank in the United States. 14
A Paucity of Evidence-Based Literature
There is little evidence-based literature for economic operating models for clinical biobanks, other than for cancer-related biobanks, where guidelines have been produced and adopted.15–17 Hence, it is difficult to formulate an overall picture of facilities currently in operation, other than the general idea that the host institution is usually responsible for the long-term survival. However, some empirical surveys have been conducted. Hirtzlin et al. surveyed European national biobanks, focusing on their organizational, economic, and ethical issues. 18 Cambon-Thomsen et al. selected European population-scale facilities 19 and Wichmann et al. described biobank funding. 20 The conclusions drawn from these studies were that biobanking does not generate profits and requires core funding. Very few biobanks registered an independent income stream, such as from charities or patients' groups, while some, such as the UK Biobank, are considered charities with a direct dependence on public funding. 21 In the majority of cases, sample distribution was considered to be an exchange or gift, rather than a purchase by a third party. Only about a third of the biobanks surveyed provided samples to a commercial third party, and only 3% reported an income from a private company. 20 This policy seems somewhat counter-productive, minimalizing the potential of biobanks to facilitate the development of new therapies. A precise analysis of the charge per unit of clinical sample was not possible, as prices varied widely amongst different archives both between, and within, European countries. The overall conclusion was that the issue of costing strategies for the long-term maintenance of biobanks has not been adequately addressed, even in the largest facilities.
Establishing a Biobionk Based on Local Needs
The IDB was established in 2006 with funding from the Guy's and St Thomas' Charity (2005–2009) and the National Institute of Health Research (NIHR: 2007–2015). The original charge was to establish ‘core’ clinical collections of samples from patients infected with human immunodeficiency virus, hepatitis B, and Staphyloccocus aureus. At the time the IDB was initiated, there were multiple biobanks in the UK dedicated to the collection of brains and cancer biopsies, but no equivalent facility for infectious diseases research. 22 Even within Europe, only three other facilities held stocks of publicly-accessible material for HIV research: the Spanish HIV Biobank, 23 Sapienza University in Italy, and Picardie biobanks. 24 The main goal of the IDB was to collect materials of significant value to researchers, the primary ‘customer base’, and one of the major stakeholders.
For the IDB, the requirement for clinical samples was initially determined by an ‘in house’ survey of researchers and clinicians, and by consideration of the most significant infectious disease problems of the local community (e.g., which has significantly higher rates of human immunodeficiency virus and hepatitis B infections than the rest of the UK) 25 . The sole aim of the IDB was to facilitate translational research. In contrast, many pathology departments have attempted to rebrand their collections as biobanks to attract research funding. The problem with this approach is that the types of samples preserved in these collections do not always coincide with the requirements of researchers (e.g., materials suitable for molecular biology studies).
Early on, it was established that the IDB would not be a genebank, but rather ‘future-proof’ itself by archiving a broad range of clinical materials (e.g., live lymphocytes, RNA, DNA, plasma, serum) that would enable a wide range of proteomic and genomic studies. These materials would be collected using established Standard Operating Procedures (UNE-EN-ISO 9001:2000) to enable inter-biobanking networking, and the business flow would be similar to that used in the pharmaceutical industry. 26
Generating Additional Funds
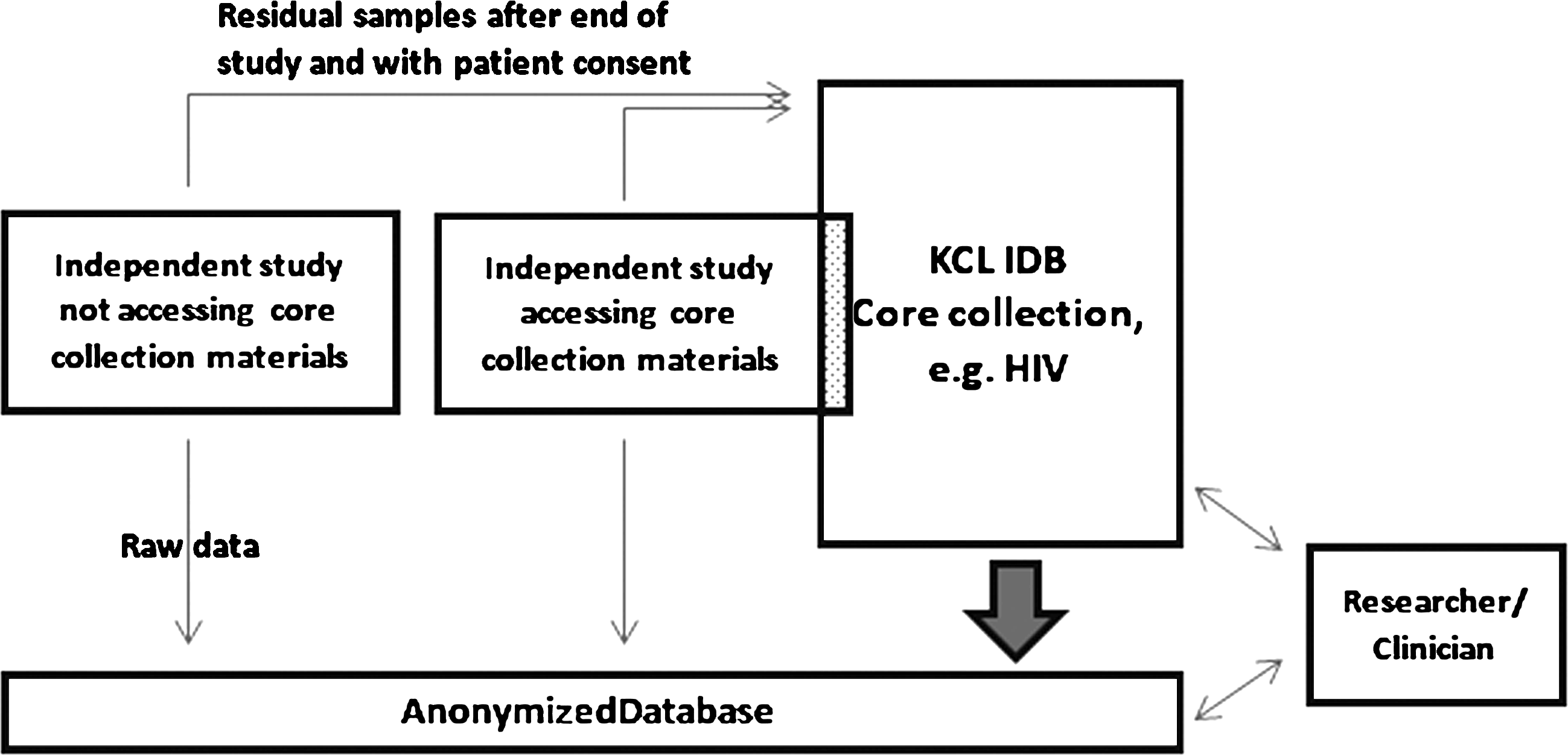
The current economic model of the IDB is based on two facts: (i) that interest in retrospective collections would be low initially and the cost of generating and maintaining such a collection, high; and (ii) that the interest in focused, small or medium size (10–300 patients), prospective collections is constant and the operating costs for these is more predictable. Accordingly, operations have evolved into two distinct arms (Fig. 1). In addition to the core funding, three additional strategies to increase the IDB's funding stream have been developed.
1. Introduction of charges (either as direct cost/sample, technical time, or by donation of additional materials to the biobank's public archive). These costs can be added to individual grant applications by researchers wishing to access IDB samples. 2. Identification of ‘emerging markets' outside the original scope of the IDB. These have included researchers studying autoimmune/inflammatory conditions (e.g., patients with systemic lupus erythematosus and children with pre-multiple sclerosis syndrome). 3. Provision of contract services for clinical studies.
Representation of the IDB's operational model. Independent studies can be performed outside of the main tissue collection function of the IDB. These studies often have specific customized SOP and ethics protocol, which can include the option for the patient/donor samples to be added to the IDB after the end of the study. Samples obtained for the independent studies are ring-fenced and unavailable to other researchers/clinicians for the duration of that study.
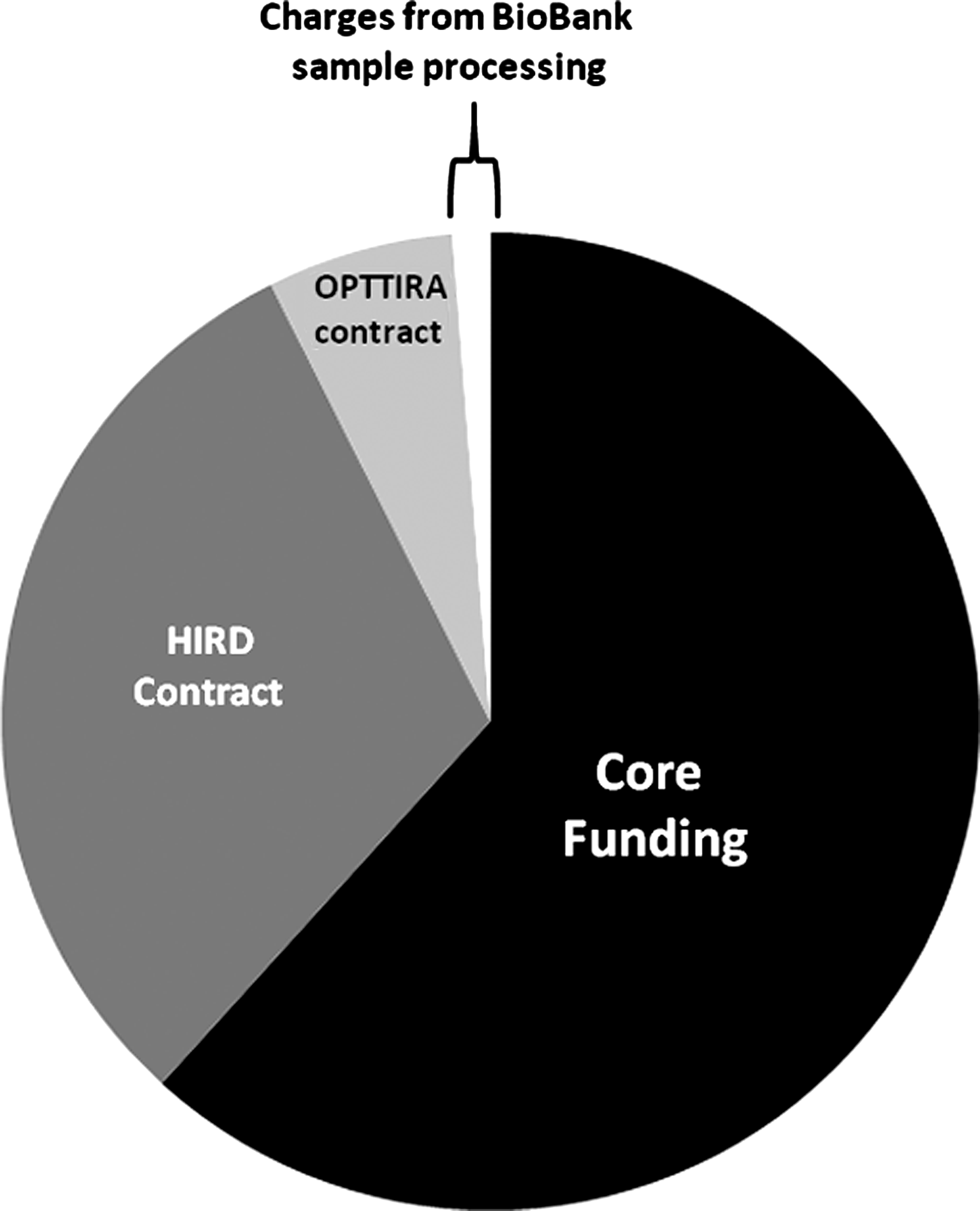
By far the most financially successful of these strategies to date has been that of offering contract services. In parallel with maintaining the routine collection of core samples, the IDB has provided contract services for an intervention study in rheumatology (OPTTIRA) and an H1N1 influenza vaccination study (the human immune response dynamics [HIRD] study). 27 In 2011, these two contract projects generated approximately $142,600 in income as compared to $4,750 charged to researchers for the preparation of IDB samples, contributing significantly to overall IDB income (Fig. 2).
Sources of income of the IDB in 2011. Percentage income from: core funding from the NIHR (black); contract research (two studies HIRD and OPTTIRA: gray); and from sample preparation charges to researchers (white). Caveat emptor: in the preceding 5 years of operation (2006–2010), only core funding was obtained.
Given the success of this funding stream, the IDB has tendered and been approved as a contractor for: (i) the custodianship/storage of the SPARTAC HIV clinical trial samples for 10 years (2012–2022); (ii) a rheumatoid arthritis drug trial (TACERA: 2012–2014); and (iii) the CHERUB, an HIV eradication study that involves all NHS's NIHR BioMedical Research Centres in the United Kingdom (including those at King's College London, Imperial College London, University College London, Oxford University, and Cambridge University 2012–2017). This ‘contracting model’ is based on similar, customized operating models that have been established in other areas to fulfil the needs of small and medium enterprises. 28 This operating model allows for turnover of studies in a reasonable amount of time, generating additional income and providing ‘added value’ to our sample collections.
The contracting requirements are also susceptible to changes in the financial climate, making forecasting of future income from these sources difficult. To combat the vagaries of the market, the IDB is aggressively promoting its' activities by: (i) creating a large electronic ‘footprint’ through web sites (e.g., http://www.kcl.ac.uk/schools/medicine/research/diiid/centres/pii/biobank/index.html) and social media (‘Linked-in’ and ‘Facebook’); (ii) publishing peer-reviewed articles;22,29–32 (iii) providing presentations to researchers (>20 in the last 12 months); and (iv) making contributions to national and international meetings.
Ethical Considerations
All subjects donating samples to the core IDB collections sign ‘broad consent’, which clearly states that the donated samples will be made available to academic or commercial researchers for future use. This informed consent enables the IDB to provide samples which can be used for a wide variety of proteomic and genetic investigations.
When providing contract services, the IDB uses one of two types of ethical approvals. For studies that are exclusive to the individual study, any residual samples must be destroyed at the end of the investigation. For other contract studies, the subjects provide consent for use of their samples both for the specific study and for the use by the biobank in future studies (e.g., the HIRD study). The IDB favors the latter situation since it minimizes waste and enhances the IDB's collection. The actual terms of access to samples are agreed to by all parties prior to study initiation.
Conclusions
One of the main obstacles in the effectiveness of translational medical research is the fragmented nature of biobank Standard Operating Procedures within a publicly funded health system as they were set up locally to cater to the ad hoc needs of the main investor (e.g., the NHS trust) and often disbanded once the needs had been met or changed. 33 This resulted in two major and distinct effects: first, the insular nature of each biobank, 20 and second, direct competition of these biobanks for the same resources. The current proposal goes some way towards providing another outcome for publicly funded biobanks—increase income by providing contract services. Furthermore, this model can address multiple needs of different stakeholders and is flexible enough to allow local modifications to be made at minimal cost.
The IDB model that has evolved embraces a duality of operations and funding streams. A caveat to the conclusion is that contract-derived income for biobanks tends to be irregular and also takes a long time to establish (the IDB was established in 2006, and 2011 is the only year in which such additional funds have been generated). Consequently, this income stream alone is insufficient at present to sustain the IDB. While additional work and costs were involved in accepting contract work, overall, this model benefited the IDB and it did not impair the recruitment and processing of patients and samples for ‘core’ projects. While the observations made here are based on only one biobank, we believe that this model may be of interest to others, particularly those embedded in ‘research-rich’ environments with large numbers of clinical trials. A recently proposed alternative model is the Dutch collaborative biobank, whereby a central facility provides services for a number of small stakeholders for whom the investment necessary to establish a biobank would be prohibitive 34 (i.e., an exclusively contractual model). This model however does not fulfil the major aim of a biobank in terms of collecting specimens for public access. While no doubt multiple other economic models for biobanking will be derived, the ultimate aim is sustainability, a significant challenge in the current economic climate.
Footnotes
Acknowledgments
The IDB is grateful for funding from Guy's and St Thomas' Charity (2005–2009) and from the NHS's NIHR comprehensive Biomedical Research Centre at Guy's and St Thomas' NHS Trust. In addition, the participation of donors and the enthusiasm of the IDB staff are greatly appreciated.
Author Disclosure Statement
No competing financial interests exist.