
Abstract
As survival rates from childhood cancer increase, fertility preservation is becoming increasingly important. Alkylating agents and whole body irradiation, common treatments in childhood cancer, have detrimental effects on follicle viability in females. Currently, ovarian tissue cryopreservation (OTC) is the only option for fertility preservation available to preadolescent females. Ovarian tissue can be harvested for cryopreservation laparoscopically without delaying cancer treatment. Although OTC is an experimental and rapidly evolving area of research, it has shown success in humans, with several live births reported thus far. Therefore, an analysis of OTC and its suitability for preadolescent females is appropriate at this time. Future research directions will allow OTC to transition from an experimental method with limited availability to a viable option for preadolescent cancer patients. As research progresses, physicians must be aware of the current state of OTC, as well as ethical concerns, risks, and benefits of OTC as a fertility preserving option.
Introduction
Fertility preservation strategies should be discussed with any patient who is likely to have impaired fertility as a result of his or her treatment. Currently, the most established method for fertility preservation in females is embryo cryopreservation. Experimental methods include oocyte cryopreservation and ovarian tissue cryopreservation (OTC). OTC is the only method available to prepubescent females, as other methods require hormonal stimulation of the ovaries for ovulation and oocyte retrieval. 2 Furthermore, because there is no need for hormonal stimulation, OTC can be carried out without any delay in cancer treatment, minimizing risk to the patient. After treatment, patients who wish to become pregnant may then undergo tissue reimplantation and natural conception or in vitro fertilization. OTC presents an exciting new option for fertility preservation, particularly for prepubescent girls, and merits further research and greater awareness among physicians.
Mechanisms of Infertility After Cancer Treatment
Whole-body irradiation (WBI) is a frequently used anti-cancer therapy that has been implicated by multiple studies in damage to reproductive organs, as evidenced by statistically relevant increased rates in ovarian and pubertal failure or insufficiency, resulting in the delay or prevention of menarche and/or aberrant hormone levels.3–5 In addition to radiotherapy, a class of gonadotoxic chemotherapeutic treatments commonly administered to children with malignancies is alkylating agents, with cyclophosphamide (CPA) as a prime example.3,6 CPA is a valuable cancer treatment because it is highly specific for cancer cells, allowing for lower dosages and reducing overall toxicity. However, CPA appears to be specifically gonadotoxic, with dysfunction occurring with greater frequency in gonadal development than in other growth patterns.7–9 In females, alkylating agents including CPA significantly increase the risk of developing ovarian failure, 10 particularly compared to other chemotherapeutic agents. 6 Thus, there is an established correlation between infertility and treatment regimens most commonly employed against malignancies in preadolescents, 3 underscoring the need for safe, readily available, and well-established fertility preserving methods for these patients.
Feasibility of Ovarian Tissue Harvesting in Preadolescent Females
Ovarian tissue harvesting is a safe and minimally invasive procedure for preadolescent females. Successful ovarian tissue harvesting has been reported in a population of 47 prepubertal females (mean age of 5 years, range of 10 months to 15 years). 11 All had uneventful intraoperative and postoperative courses. In this cohort, histological evaluation of harvested ovarian tissue showed a strong inverse correlation (p<0.005) between follicle density and patient age, suggesting that the probability of restoring fertility using OTC may be higher in preadolescent females as compared with older women. 11 In another study, there was a significant inverse correlation between follicular density and age (r=−0.48, p<0.001) in 21 samples of ovarian cortical tissue, 17 from patients undergoing OTC, and 4 from donated ovarian biopsies. However, in 6 patients who had already received chemotherapy prior to retrieval of tissue, there was no correlation with age. 12 This underscores the need to offer OTC early in the course of treatment for cancer, before the gonadotoxic effects have a chance to harm the follicular pool. A larger sample of 23 patients whose ovaries were cryopreserved after chemotherapy also found this correlation, as well as a larger number of viable, non-apoptotic follicles in younger patients (age ≤20 years) after treatment in comparison to women>30 years of age. 13
Timing of Ovarian Tissue Harvesting
The timing of ovarian tissue harvesting is an important consideration that has not been well defined. It may be argued that harvesting tissue after a first round of chemotherapy can reduce the incidence of metastasis in ovarian tissue. However, evidence of malignant cells has been found in ovarian tissue harvested from patients with chronic myeloid leukemia (CML) and acute lymphoblastic leukemia (ALL), even after multiple cycles of chemotherapy. Because even one round of chemotherapy can be deleterious to a patient's follicular pool and chemotherapy does not completely eliminate malignant cells in harvested tissue, it is recommended that OTC be performed before the initiation of chemotherapy whenever possible. 14 With good coordination between referring oncologists and the gynecologic team, OTC can be carried out prior to chemotherapy with minimal disruption to the primary treatment plan. 15
Ovarian Tissue Harvesting Procedure
Ovarian tissue harvesting for cryopreservation is generally performed laparoscopically, 11 either by harvesting an entire ovary or via ovarian cortical biopsy. 16 A biopsy is generally preferred, but in preadolescent patients it may be necessary to take the whole ovary in order to harvest enough tissue for cryopreservation. 2 Once ovarian tissue is harvested, it is most commonly processed into strips and then is ready for cryopreservation. A bacteriological swab of each piece of tissue is taken prior to freezing to assess contamination, and one slice is prepared for histological evaluation. 15
Cryopreservation of Ovarian Tissue
Slow-freezing and vitrification are two methods used for cryopreservation of ovarian tissue, varying primarily in the rate of cooling of the tissue samples and the concentration of cryoprotectant. Another major difference between slow-freezing and vitrification is the concentration of cryoprotectives. In a comparison of slow-frozen and vitrified ovarian tissue, there was no difference in follicle viability, vacuole formation, and mitochondrial damage between the two methods. However, better embryological development after in vitro fertilization was observed in slow-frozen tissue. 17
Another difference between slow-frozen and vitrified tissue is that vitrified samples contain fewer primordial follicles and produce less anti-Mullerian hormone (AMH) than slow-frozen samples when using a particular freezing method. AMH production from slow-frozen samples was comparable to that of fresh tissue. 18 Because AMH is an indicator of fertility and egg supply, this would suggest superiority of the slow-freezing method in preserving ovarian tissue, at least with this specific freezing protocol. However, one study showed that the mouse pup birth rate using vitrified tissue was similar to that of fresh tissue, suggesting that vitrification may not have an overall adverse effect on oocyte quality or pup production rate. 19
Slow-frozen and vitrified samples both produced significantly less estradiol than fresh tissues. As AMH and estradiol are both produced by granulosa cells and AMH production was preserved in slow-freezing, the lower levels of estradiol more likely result from the inhibition of aromatase activity during freezing rather than damage to granulosa cells. 18
Histologic and Molecular Evaluation of Ovarian Tissue
Histological evaluation of ovarian tissue harvested for OTC is used to assess follicular density and to screen for evidence of disease within the ovary. However, it may not identify minimal residual disease in tissue, particularly in the case of leukemias, which are a common cause of malignancy in young patients. In one investigation of 6 patients with chronic myeloid leukemia (CML) and 12 with acute lymphoblastic leukemia (ALL), histological evaluation did not identify any malignant cells, while reverse-transcription PCR (RT-PCR) showed positive markers in 2 of 6 CML patients and 7 of 10 ALL patients with available molecular markers. 14 Thus, both molecular and histological evaluation of ovarian tissue is essential to identify any residual disease.
Orthotopic and Heterotopic Transplantation of Ovarian Follicles
Thawing procedures differ depending on the method of cryopreservation, as well as on the composition of the cryoprotectant solution used during freezing. 20 After thawing, the tissue can be transplanted orthotopically or heterotopically. Orthotopic transplantation is the grafting of tissue back to the pelvic area, with the goal of restoring normal ovarian function. 21 This is followed by either natural conception or oocyte collection for in vitro fertilization and embryo implantation. Heterotopic transplantation involves grafting of tissue subcutaneously to another site on the body, followed by oocyte retrieval, in vitro fertilization, and embryo implantation. So far, only orthotopic transplantation has resulted in live births.3,22
One report evaluated the characteristics of follicular development following ovarian tissue transplantation to orthotopic and heterotopic sites within the same patient. Orthotopic transplantation occurred at ovarian and peritoneal sites, while heterotopic transplantation occurred in an abdominal subcutaneous site. All three sites of transplant showed follicular development, with the ovarian site showing the greatest follicular development. Local environment and vascularization of the ovary may be involved in the increased follicular development at the ovarian site. 22
In Oktay et al., 23 ovarian tissue was heterotopically grafted in a subcutaneous abdominal site, and oocytes were retrieved starting at 85 days after implantation and periodically over the next 8 months. Of the 20 retrieved oocytes, eight were suitable for in vitro fertilization. From those eight, one developed into a four-cell stage embryo, suggesting the feasibility of heterotopic grafting of ovarian tissue. However, the embryo did not progress past the four-cell stage. A comparison of oocytes from heterotopic and orthotopic transplant sites showed smaller, lower quality oocytes from heterotopically transplanted tissue. Differences in temperature and blood flow to orthotopic and heterotopic sites may cause the disparity in oocyte quality. 23
In Vitro Growth and Maturation of Human Follicles
In vitro growth and maturation (IVGM) of human follicles isolated from ovarian tissue is an active area of research. While pregnancy resulting from IVGM of follicles in humans has not yet been demonstrated, the work of several groups shows promise for this technique. One of the challenges of culturing pre-antral follicles is maintaining physical contact and the metabolic link between an oocyte and its associated granulosa cells. This is critical to the proper, coordinated growth and differentiation of somatic and germ cells. 24 One group demonstrated coordinated growth of human secondary follicles isolated from fresh ovarian tissue in a 3D culture system, also indicating that the major steps of human follicle development were maintained. 25 Furthermore, the size of the oocytes in the cultured follicles was the same as that of meiotically competent oocytes aspirated from in vivo human antral follicles, indicating that these oocytes could potentially continue into meiosis II. Another group has demonstrated that small pre-antral follicles from frozen-thawed human ovarian tissue can survive and develop on a calcium alginate matrix after enzymatic isolation and in vitro culture, indicating that methods that work for fresh tissue will work similarly for frozen tissue. In this study, after seven days of culture, 90% of follicles had living oocyte and granulosa cells, and all follicles had increased in size. 24
Recently, the successful production of healthy mouse pups has resulted from in vitro follicle culture of both fresh and vitrified adult mouse ovarian tissue. 26 While this research is in its early stages, it is nevertheless encouraging that IVGM of human ovarian follicles will one day be feasible for cryopreserved ovarian tissue, eliminating the risk of reimplanting malignant cells and the need for multiple surgeries inherent in both orthotopic and heterotopic transplantation techniques.
Live Births
Lee et al. reported the first live birth in a primate through the use of ovarian tissue cryopreservation in 2004. 27 Later that year, the first live birth from orthotopic grafting of ovarian tissue occurred in a human. 28 Since the first human live birth, there have been a total of thirteen live births reported among 10 women. 16 These patients, aged 17 to 36 years at the time of OTC, had diagnoses of Hodgkin's and non-Hodgkin's lymphoma, breast cancer, sickle cell anemia, microscopic polyangiitis, Ewing's sarcoma, and a neuroectodermal tumor with metastases. All patients required treatments that threatened future fertility, and four had received chemotherapy prior to OTC. 16
Restoration of ovarian function after reimplantation, or the development of a follicle with each cycle—indicated by a rise in estradiol and a decrease in luteinizing hormone—occurred 3.5 to 6.5 months after tissue reimplantation, although this timeframe would include the time required for the first primordial follicles to mature. The time between tissue implantation and onset of pregnancy ranged from 6 to 11 months. Women who received chemotherapy prior to ovarian tissue harvesting had a longer interval between tissue reimplantation and restoration of ovarian function and a shorter duration of restored ovarian activity. Because the histology of harvested ovarian tissue from these women revealed many primordial follicles, it is likely that the longer interval between tissue reimplantation and restoration of ovarian function was due to the negative effects of chemotherapy on vascularization. 16
Of the thirteen births, seven of the offspring were conceived naturally while the other six pregnancies occurred through in vitro fertilization. 16 In September 2008, for the first time, a woman gave birth to her second child after OTC, demonstrating that it is possible for previously infertile female patients to have multiple pregnancies and births with the help of OTC 29 (Tables 1 and 2).
Possible demonstrations of transplanted ovarian tissue viability include estradiol production (ED); increased AMH production (AMH); decreased FSH/LH production due to ovarian regulation (PH); or presence of follicles (FO), oocytes (OO), granulosa cells (GC), or stroma cells (SC).
Review article - some data may be double-reported in table.
Ten cases of orthotopic transplantation reported - all 10 showed decreased FSH levels and follicle development post-transplantation, while 8 reported increased estradiol levels and 4 reported increased AMH production.
Risks and Costs of Ovarian Tissue Cryopreservation
In two cohort studies of a total of 132 women receiving OTC, the procedure and postoperative course was uncomplicated for all women.11,15 The overall complication rate for laparoscopy in gynecology is 4.64 per thousand cases, and overall mortality rate is 3.33 per hundred thousand cases. 30 For laparoscopy in general, common complications include vascular injury, visceral injury, dehiscence and hernia, wound infection, port site metastasis, and extraperitoneal gas. There is also the risk of infection from contamination of tissue during preparation for freezing. Microbiological testing at the time of tissue harvesting and again prior to tissue transplantation can help reduce this risk. It may be advisable for all patients receiving transplanted ovarian tissue to undergo a course of prophylactic antibiotics to further minimize the risk of infection. 15
The risk of reintroducing malignant cells into a patient upon transplantation of ovarian tissue varies with the original malignancy. While data on the risk of reintroducing malignant cells with ovarian tissue autotransplantation are limited, none of the 10 women who have successfully given birth after OTC have experienced disease recurrence. 16 Presence of malignant cells in ovarian tissue depends on the type and stage of disease, and certain diseases such as leukemia carry a higher risk of disease transmission through ovarian tissue. Survivors of ALL and CML may be at risk for disease recurrence from reimplanted ovarian tissue even if molecular markers by RT-PCR analysis are negative, as patients in remission from CML and ALL can present with negative molecular results in blood and/or bone marrow, and still relapse. 14 Therefore, grafting of ovarian tissue in patients with ALL and CML cannot be recommended at this time. OTC may still be offered to these patients, as ongoing research on IVGM of ovarian tissue may eliminate the need to reimplant ovarian tissue in the near future.
The estimated cost of the surgical procedure for OTC is $12,000, excluding additional variable costs to store and reimplant the tissue. 31 Though the cost of freezing ovarian tissue is not firmly established, the annual cost of ovarian tissue storage may be similar to that of embryo storage, which costs approximately $350 to $500 per year. 32 The estimated costs of thawing, culture, fertilization, and embryo transfer, including one pregnancy blood test, add up to $3,162, and the medication costs for cycling can range from $2,000 to $4,000. 33 Currently, no state mandates insurance coverage of fertility preservation services, leaving patients and their families to pay for OTC themselves. However, in February 2011, California's state assembly member Anthony Portantino proposed a bill, AB 428, currently in committee, that would ensure health care coverage of fertility preservation services for iatrogenic infertility. 34
Value of Fertility to Patients and Ethics of Ovarian Tissue Cryopreservation
Early in a patient's diagnosis and at follow-up visits, a physician should discuss any risks, options, and alternatives regarding fertility treatments, so that infertility is less likely to become a concern in the future. At one center, the majority of adolescent cancer patients who faced medium and high infertility risks identified infertility as a concern. 35 Even after treatment ends, patients who become survivors express worry about infertility resulting from their therapy. In a survey of 400 long-term survivors of childhood cancer, the survivors reported a significantly higher degree of worry about their fertility in comparison to their counterparts who had no history of cancer. 36 The immediate and future concern that cancer patients have about infertility illustrates the importance of discussing fertility preservation options before cancer therapy begins. While the topic may be difficult to broach at the time of diagnosis, the physician should be aware of fertility concerns and remember that a patient may be highly motivated to pursue fertility preservation.
Most of the ethical issues regarding OTC for preadolescents surround the question of how an informed, joint decision can be made by both patient and parent. In a study of parents of pediatric cancer patients, only 29.9% of parents were satisfied with the amount of information provided about fertility preservation. 35 A child has the right to fertility preservation, acknowledged in bioethical literature as a “right in trust” or “right to an open future” which is to be saved until the child reaches adulthood when the child is capable of deciding. 37 A physician is responsible for informing the patient and her parents about potential psychological and physical health risks and benefits of fertility preservation procedures, both immediate and long-term. In addition to a consultation, the patient and her family should be provided with resources, such as pamphlets and referrals to fertility specialists, to make an educated choice.
An important consideration for the patient and her parents is that the risks of the tissue harvesting procedure must not outweigh the potential benefits, particularly because this is not a medically necessary procedure. Additionally, not every patient pursuing OTC will benefit from the procedure because they may not experience premature ovarian failure, regain fertility using the tissue, or survive their cancer treatment. 16 Physicians must be sensitive to the difficult decisions a patient and her parents face when presenting options for fertility preservation.
In most cases when a patient under 18 decides to proceed with OTC, she will sign an informed assent and a parent or legal guardian will sign an informed consent. However, in many states a minor may legally consent to receive reproductive care, which may include fertility preservation, without parental notification. Because of the conceptual complexities of OTC, it can be difficult to assess whether a child is fully aware of the consequences of undergoing this procedure. Therefore, it is critical for the physician to carefully assess the comprehension of the parent and the patient of any age, and determine whether both parent and child are emotionally, psychologically, and mentally competent to consent and assent.
Conclusion
OTC is a promising new method of fertility preservation for preadolescent female patients who require treatments that will threaten their fertility. While modern chemotherapeutic agents and radiation therapy have greatly increased survival rates from childhood cancer, these same treatments jeopardize survivors' reproductive capacity. OTC is a safe and effective method of fertility preservation for preadolescent females. However, it is not indicated in certain cancers because grafting of cryopreserved ovarian tissue still carries the risk of reimplanting malignancy. As OTC is still considered experimental, availability and awareness of the procedure is highly limited, and additional research is needed to make OTC a more established method of fertility preservation.
In a recent study of pediatric hematology–oncology healthcare providers, only half of them were knowledgeable about current research on female fertility preserving options, indicating a need for greater awareness. 1 The Oncofertility Consortium is an organization that provides current information about OTC that healthcare providers can use in their discussions with patients, such as which options may be best for a particular patient and where the nearest fertility centers are located. 38 Hospitals should establish interdisciplinary teams that are knowledgeable about OTC that can inform and guide patients, as well as facilitate better communication about OTC among medical personnel. Because infertility is a documented concern for young cancer patients and their families, physicians should be prepared to discuss the risk of infertility associated with cancer treatment and options for fertility preservation. Figure 1 provides a potential guideline.
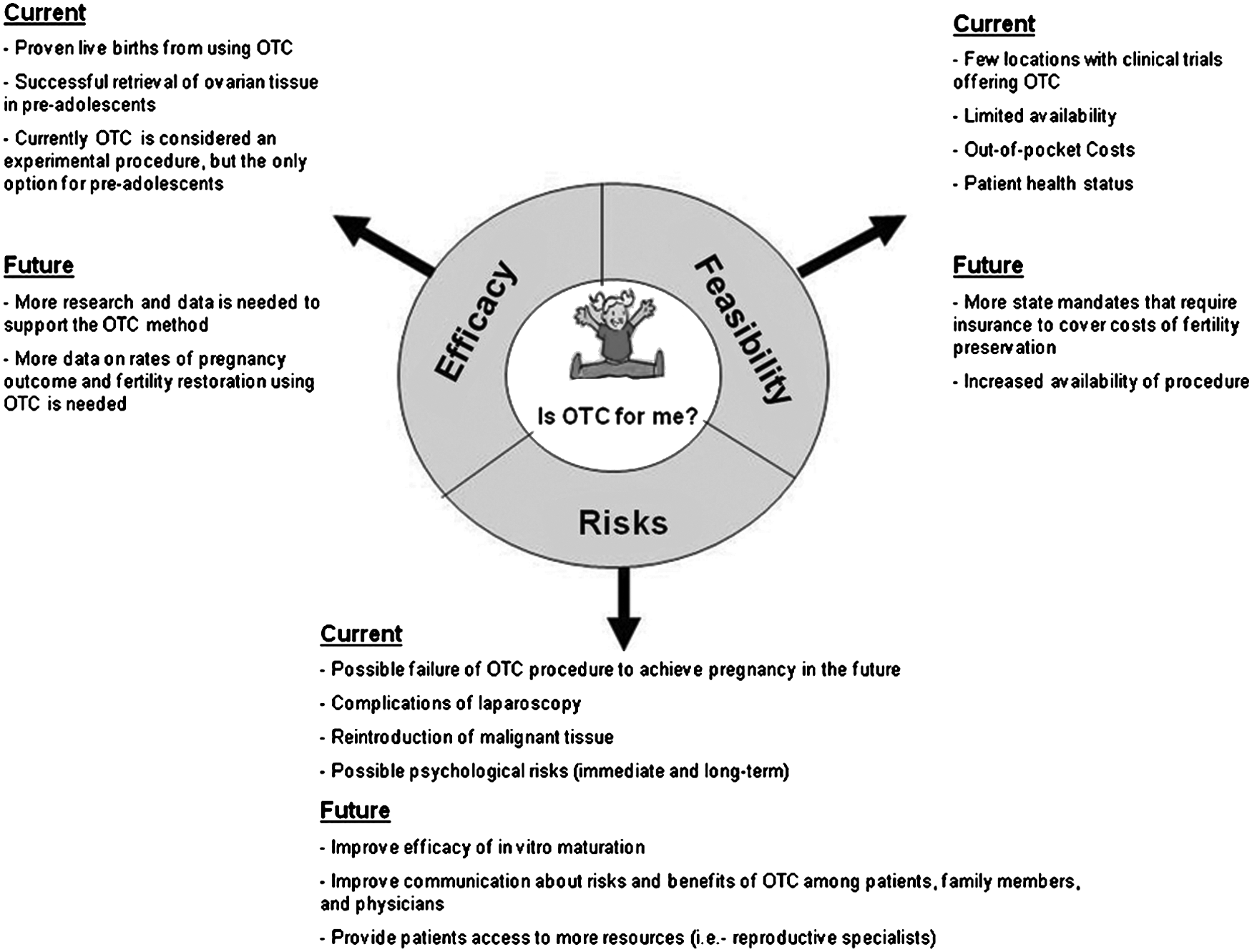
Efficacy, feasibility, and risks of ovarian tissue cryopreservation.
Research establishing IVGM of frozen-thawed human ovarian follicles is essential to the future of OTC. As a process that develops primordial follicles into mature follicles that are ready for in vitro fertilization, IVGM bypasses the step of reimplantation of ovarian tissue, thereby eliminating the risk of minimal residual disease transmission. By the time that preadolescent female patients are ready to have children, IVGM may well be an established option. Of course, a more ideal approach to fertility preservation would be to avoid iatrogenic infertility altogether. Until this becomes a reality, physicians should keep in mind the value of fertility preservation to pediatric cancer patients.
Footnotes
Acknowledgment
Special thanks is given to Michele Malloy of the Georgetown University Medical Center for her help in the preparation of this manuscript.
Author Disclosure Statement
No competing financial interests exist.