
Abstract
While the development of large scale biobanks continues, ethics and policy challenges persist. Debate surrounds key issues such as giving and withdrawing consent, incidental findings and return of results, and ownership and control of tissue samples. Studies of public perception have demonstrated a lack of consensus on these issues, particularly in different jurisdictions. We conducted a telephone survey of members of the public in Alberta, Canada. The survey addressed the aforementioned issues, but also explored public trust in the individuals and institutions involved in biobanking research. Results show that the Alberta public is fairly consistent in their responses and that those who preferred a broad consent model were also less likely to desire continuing control and a right to withdraw samples. The study raises questions about the role of public perceptions and opinions, particularly in the absence of consensus.
Introduction
Much has been written on the many ethical and legal challenges associated with large-scale biobanking,5–7 which have emerged as one of the most debated and intractable research ethics dilemmas of recent times. Despite the production of innumerable policy reports8,9 and the adoption of various approaches to oversight and governance,3,10,11 controversies have endured around issues of consent, privacy, and the control and ownership of tissue samples.
In the hope of informing policy development, a good deal of research has been done on public and patient perspectives. 12 Many of these studies have explored specific aspects of the biobanking controversy, particularly issues related to consent,13–15 and to date, they have shown wide variation in perceptions and views on ethical and policy issues such as consent,14–16 ownership of and control over banked samples,17,18 and disclosure of incidental findings.13,19
Few of these studies, however, have looked at the broad range of ethical and policy issues within the same survey instrument, especially in Canada (see, however, Pullman et al. 20 ). This study sought to gain insight into the perspectives of Albertans on key ethical issues in biobanking research. Given the lack of Canadian data directly on point, the unique aspects of the Canadian research environment (including a citizenry that is strongly supportive of both public health research 21 and the public healthcare system), and the continued national and regional investment in biobanking, a survey of this nature is timely and, it is hoped, will help inform the Canadian dialogue on how to best address these challenging issues. In addition, the survey is the first Canadian study to explore a broad range of biobanking issues within the same survey instrument, allowing an opportunity to both explore correlations between perspectives and to compare Canadian perspectives with results from other jurisdictions.
Methods
Alberta residents were surveyed regarding their perceptions of key issues in biobanking initiatives. The telephone survey was conducted by the Population Research Laboratory (PRL) at the University of Alberta in Edmonton, Canada. Survey participants were contacted using a Random-Digit Dialing (RDD) approach to ensure that respondents had an equal chance to be contacted whether their household was listed in a telephone directory. The total number of eligible phone numbers dialed was 8724. A phone number was considered ineligible if it was not assigned to a residence, if it was not in service, or no contact was made within 10 attempts. The final sample of 1201 respondents consisted of 600 females and 601 males aged 18 or older. Participants were from both urban and rural areas of Alberta and were distributed as follows: Metropolitan Calgary (n=401), Metropolitan Edmonton (n=400), and the remainder of the province (n=400). The majority of participants have completed post-secondary education (Calgary: 83.7%; Edmonton: 74.5%; remainder of province: 67.3%). Data collection took place between May 31, 2011 and July 4, 2011. The survey response rate was calculated at 24.3%.
Prior to data collection, the survey was pre-tested by trained interviewers with 20 household respondents in Alberta from May 9 to May 11, 2011. The purpose of the pretest was to check the question wording, question order, response categories, interviewer instructions, and length of interview. Interviewers' comments and frequency distributions were reviewed before modifications were made to the survey instrument by PRL. The survey consisted of two sections. The first section was designed to elicit demographic information such as employment, religion, ethnic background, and place of birth, and the second section elicited participant opinions regarding key issues in biobanking. The average length of the survey interview was 32 minutes. The University of Alberta's Arts, Science and Law Research Ethics Board (ASL REB) reviewed and approved survey questions and data collection protocols.
Respondents were asked a series of questions regarding their views of consent, withdrawal, anonymization of samples, ownership and control, incidental findings, and trust in biobanking science and practices. At the beginning of each survey interview, respondents were provided the following brief explanation of biobanking: “For lots of different health studies, researchers collect biological samples, such as blood, tissue and urine, and health information, such as family medical history and genetic information. When these are collected, usually with consent, they are often stored for future medical research, which may not be known at the time of a collection.”
After survey data was collected, results were transformed into numeric responses. Data were then tabulated and analyzed using IBM SPSS for Windows. Pearson's Chi-squared test was used to determine significance (p=0.05).
Survey Context
At the heart of many of the biobanking policy challenges are questions of consent and control. One of the most contentious issues is whether researchers can obtain legal and ethically appropriate consent on the basis of a broad, one-time consent to all potential future research uses of a banked sample, or whether specific consent must be sought from participants for each proposed use of banked samples. While most biobanks have adopted the broad consent strategy, 22 some commentators believe existing norms demand some form of specific consent.23,24 Similarly, there are enduring questions about who owns and controls tissue samples and whether incidental findings need to be returned to research participants. Indeed, these issues have led to litigation25–28 and intense academic debate.5,29
Many studies have been conducted to attempt to gauge public perceptions of biobank research and to ascertain the views of potential and actual research participants around consent and related issues.30,31 Such research can provide a sense of the acceptability and potential success of various approaches to biobanking. It can also help highlight possible areas of tension and triggers of public controversy.
In addition, understanding public perceptions is important to efforts to harmonize biobanking policy. As noted, many countries have sought to implement large-scale biobanks. And, given that banked samples and data are shared internationally, there is a desire for harmonized research ethics policies 32 —a reality that has led to projects that have strived to develop, inter alia, standard terminology and model consent forms and access rules. 33 Despite these efforts, much uncertainty and variability remain. 34
It is within this context that we crafted our survey questions. Informed by existing literature 5 and a survey of existing biobanking public perception research, 12 we sought to gain insight into the perceptions of Albertans on a wide range of contentious biobanking issues.
Results
Consent
Results from this survey of the Alberta public indicated that the majority of Albertans prefer to be asked permission to use their samples only once (51.8%). Yet a sizeable number also prefer to be asked permission each time a sample is used (18.0%), or would like to be provided options for when a sample can or cannot be used (30.2%).
Participants also stated their agreement to a series of statements regarding how they feel about different aspects of consent. Responses to these statements are detailed in Table 1.
Withdrawal and anonymization
Survey participants responded to questions regarding withdrawal and anonymization of samples. Respondents were provided the following description of the differences between anonymized and de-identified samples:
“An anonymized sample is when there is no way to trace it back to the donor. A de-identified sample is when researchers do not readily know who the sample belongs to, but it can be traced back to the research participant. Anonymized samples may best protect a research participant's privacy, but once a sample is anonymized it is impossible for him or her to withdraw their sample.”
71.2% of respondents thought they should have a right to withdraw their consent and sample at any time. Yet when asked whether it was more important to them to be able to have their samples de-identified and the ability to withdraw, or to have their samples anonymized, only 58.4% of respondents thought it was more important to have their samples de-identified with the right to withdraw, as opposed to 41.6% who thought it was more important to have a sample anonymized.
Ownership and control
When asked about who owns samples, many respondents indicated that they thought the institution where the research was being conducted owned the samples (44.3%). However, 25.7% of respondents thought that they owned their samples, 23.1% thought that the researcher who was conducting the research owned the samples, and 6.9% of respondents thought some other research funder owned the samples. Despite this varied perception of ownership, 53.0% of all respondents still thought they had a continuing right to decide what is done with their sample.
Incidental findings and disclosure of risk
When asked what researchers should do when they discover information related to an individual's health, the majority of respondents thought researchers should tell both the participant and the participant's doctor (53.4%). Some respondents (18.6%) indicated that a researcher should tell only the participant, 17.7% said their doctor should be told, and 10.2% said the researcher should do nothing with the information. Respondents were questioned further about their perceptions of incidental findings and disclosure of risk (Table 2).
Trust
Finally, public trust in the different individuals involved in biomedical research may affect potential research participants' opinions on the foregoing issues. Survey respondents were asked about their level of trust in a variety of individuals and institutions to care for and use confidential health information (Table 3). Not surprisingly, the insurance and for-profit industries were the least trusted, whereas doctors and hospitals were the most trusted.
Correlations between perceptions
Responses were analyzed for significant differences between categories. Our results indicated a large number of significant differences in the perceptions of these issues, both demographically and within the issues themselves. Given the results of prior studies, these differences were not unexpected. Interestingly, however, the results also demonstrate remarkable consistency in participants' views. Using terminology used by Simon et al., 35 the groups can be viewed as consistent in that those who preferred specific consent also tended to desire a significant level of continuing control over their samples, and to a lesser degree, exhibited less trust in research institutions.
There were a number of differences between demographic categories. Men showed more trust in the research process and individuals involved in biobanking research (sig.=0.000 to 0.034). Level of education played a role in consent preferences. The less education, the more likely that respondents would prefer specific consent, and the more education the more likely that respondents would prefer broad consent (sig.=0.016). In terms of ownership, the less education a respondent had received, the more likely they were to believe they owned their samples, but the more education that respondents had, the more likely they were to think the institution conducting the research owned the samples (sig.=0.000).
In terms of the key issues addressed in the survey, the respondents exhibited consistency between their views of consent, withdrawal, ownership, and continuing control. Respondents who indicated that they preferred specific consent tended to think that they had a right to withdraw their consent and samples at any time (sig.=0.000), that it was more important to have samples de-identified with a right to withdraw (sig.=0.001), that they owned their samples (sig.=0.000), and that they had a continuing right to decide what to do with their samples (sig.=0.000) (Fig. 1). In addition, respondents who preferred specific consent also tended to have less trust in university researchers funded by both government (sig.=0.000) and industry (sig.=0.001), disease-based foundations (sig.=0.004), hospitals (sig.=0.000) and doctors (sig.=0.000).
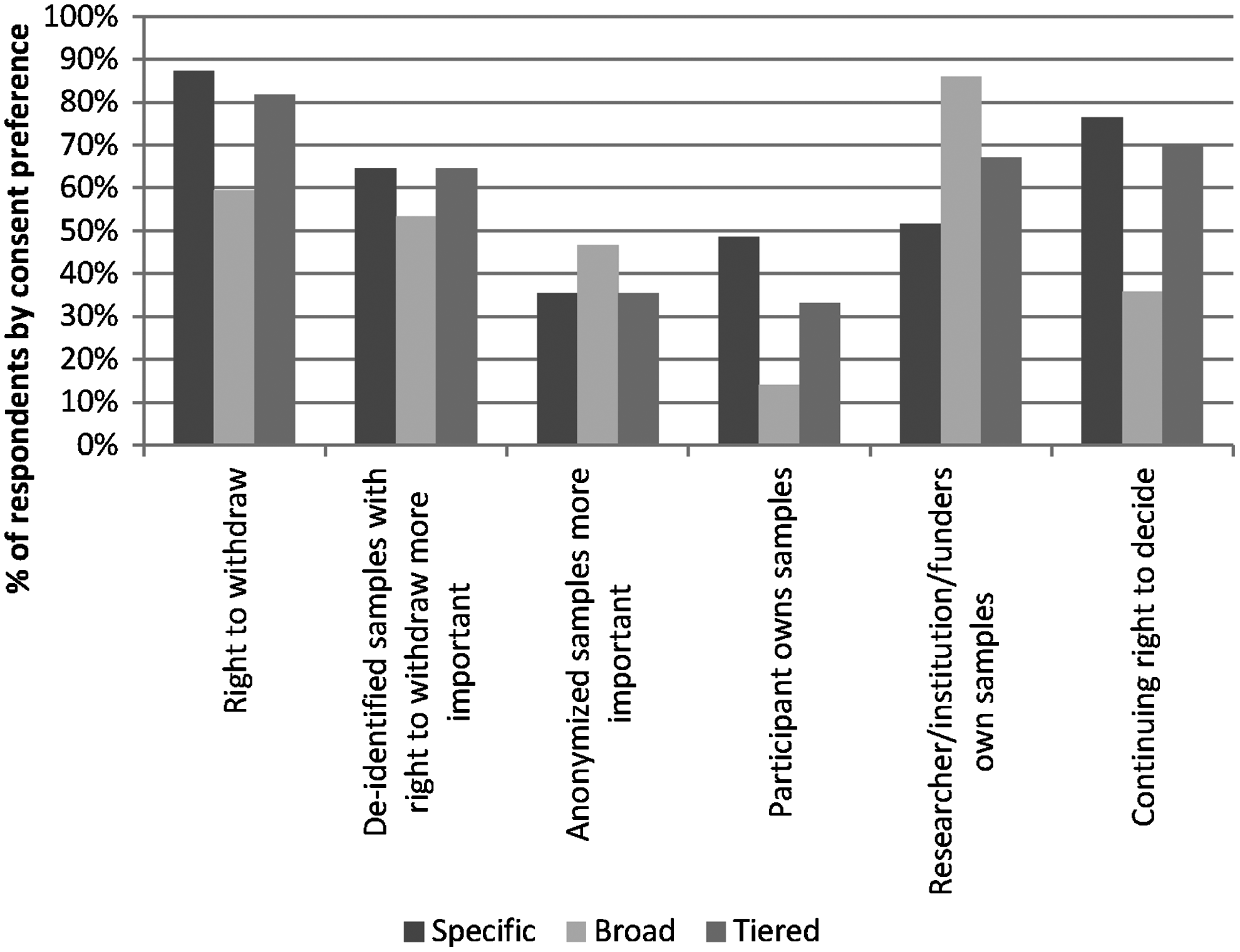
Comparison of public preferences for consent with other key biobanking issues.
The relationships between perceptions of ownership, control, and incidental findings also had significant differences. Respondents who did not believe they should have the right to withdraw, and those who preferred anonymized samples, were more likely to think that the institution conducting the research owned the samples (sig.=0.000). Respondents who believed they should have the right to withdraw, and those who preferred de-identified samples with the right to withdraw, were both more likely to want continuing control of their samples (sig.=0.000). Respondents who believed they should have the right to withdraw were more likely to want to learn about incidental findings (sig.=0.000).
Trust in the different individuals and institutions involved in biobanking research initiatives appeared to play a significant role in respondents' views of the key issues. For example, it seems that the less trust that a potential research participant has, the greater their desire for specific consent and a right to withdraw at any time, as well as a belief that they own their samples and have a continuing right to decide what happens to these samples. It is not possible to infer whether a lack of trust encourages people to want more control, or vice versa, but the results demonstrated that there is a connection.
Discussion
Our data again emphasizes the lack of consensus among the public about key biobanking research ethics questions. While we found that a reasonably high percentage of respondents stated a preference for a one-time, broad consent approach (51.8%), a significant minority (18%) preferred specific consent. Once we include those who stated a preference for being provided a list of options (30.2%), often termed tiered consent, we find a near even split between those that are comfortable with a broad consent approach and those that want more enduring control. This is similar to results from other surveys. 35
The implications of the diversity of views on these issues are complex. While consensus alone is not a solid foundation for policy development, its absence can make the task more difficult as policy makers attempt to craft rules that acknowledge different perspectives. Large variation in public opinion between jurisdictions may also complicate efforts toward harmonization on an international level. 12
The inclusion of a broad range of ethical and policy issues within our survey also allowed us to analyze perspectives on a variety of issues. We found participants to be remarkably consistent in their positions across a variety of domains. Those who prefer a specific consent model also appear to be less trusting and to prefer a level of control and ownership over their samples. This is in contrast to those who prefer a broad consent model who also appear to be more trusting and believe that control and ownership is in the hands of the researchers and institutions to whom their samples were provided.
Not surprisingly, trust appears to play a role in the degree to which the respondents preferred ongoing control, and in whether they would like to be asked permission for each new study. That said, it is difficult to tell whether there is a causal relationship here; in other words, whether the reduced trust causes the desire for increased control over one's samples. It is equally possible that the people who are more likely to want to control their samples and to be asked for specific consent are also more likely to distrust institutions and individuals who have access to confidential health information. This is an interesting question for future consideration. Does this latter position suggest views that may be deeply entrenched and therefore less likely to change over time? If so, it may make it more difficult to craft polices and public engagement strategies that can resolve the dilemma. The relationship between trust and public perceptions on issues like consent and control also highlights how fragile public opinion likely is. Past experience has taught us that even one high profile controversy can have a tremendous impact on perceptions.28,36
Insights into public perceptions of ethical issues in biobanking are valuable in assisting policy-makers as they attempt to understand various publics' preferences and concerns, and as they try to predict how the public will respond to specific policies. Perhaps the most remarkable feature of the public perception data that has been collected to date is the consistent finding that perceptions vary widely, both within and among different publics, and that no consensus exists on many of these issues.12,30,31,37
As with all survey approaches, this study has limitations. It is a survey of Albertans, and perspectives may vary across Canada. Also, we did not pose many trade-off questions that ask participants to weigh, for example, the value of scientific inquiry against other interests, such as consent (an approach effectively done in other relevant studies 20 ). We also acknowledge that the respondents' experiences with healthcare or biomedical research may also influence responses. This relationship was not addressed in the survey instrument and would provide an area for further research. Nevertheless, the results provide a meaningful contribution to the broader understanding and debate surrounding public perceptions of biobanking. And while the relevance of public perception data—one factor in the development of biobanking policy—to the policy-making enterprise is unsettled and uncertain,38,39 this information remains very valuable in highlighting the importance of certain issues over others, and in guiding policy debate and discussion.
Footnotes
Acknowledgments
We would like to thank the University of Alberta's Population Laboratory for their technical and research assistance in the survey data collection, as well as Amy Zarzeczny, Robyn Hyde-Lay, and Zubin Master and the Health Law and Science Policy Group for their assistance on all aspects of the project. We would also like to thank the Cancer Stem Cell Consortium, the CBCF Tumour Bank, and the Interdisciplinary Chronic Disease Collaboration for their generous funding support.
Author Disclosure Statement
The authors have no competing financial interests to declare.