
Abstract
Human biological specimens are important for translational research programs such as the Canadian Ovarian Experimental Unified Resource (COEUR) funded by the Terry Fox Research Institute. Sample quality is an important consideration, as it directly impacts the quality of ensuing research. The aim of the present study was to determine the quality of tissues collected from different sites contributing to the COEUR cohort. Samples from high-grade serous ovarian tumors (fresh frozen and corresponding paraffin-embedded tissues) were provided by nine participating Canadian biobanks. All samples were shipped to a central site using a Standard Operating Protocol (SOP). DNA and RNA extraction was conducted by the quality control division of the Canadian Tumor Repository Network (CTRNet). DNA quality was determined by ß-globin gene PCR amplification, and RNA quality by the RNA integrity number (RIN), as measured by the Agilent BioAnalyzer. DNA of acceptable quality had at least three bands of ß-globin amplified from DNA (n=115/135), and a RIN number ≥7 was considered very good for RNA (n=80/135). Sample preparation and storage time had little effect on RNA or DNA quality. Protein expression was assessed on tissue microarray by immunohistochemistry with antibodies against p53, WT1, E-cadherin, CK-7, and Ki67 from formalin fixed-paraffin embedded (FFPE) tissues. As seen with a nonhierarchical clustering statistical method, there was no significant difference in immunostaining of paraffin tissues among specimens from different biobanks. Interestingly, patients with worse outcome were highly positive for p53 and weak for WT1. In conclusion, while there was no common SOP for retrospectively collected material across Canadian biobanks, these results indicate that specimens collected at these multiple sites are of comparable quality, and can serve as an adequate resource to create a national cohort for the validation of molecular biomarkers in ovarian cancer.
Introduction
The ovarian cancer community in Canada, which is vibrant and collegial, is interested in pursuing a large-scale biomarker program at a cooperative level. During the 4th Canadian Ovarian Cancer Research Conference (May 4th–7th, 2008; Montreal, QC), the community outlined the initial plan of a Canadian Ovarian Cancer Research Consortium (COCRC). “A Trans-Canadian Platform for the Development of Biomarker Driven Subtype Specific Management of Ovarian Carcinoma” was created in November 2008. In January 2009, members of the Canadian ovarian cancer community were invited to participate in the pan-Canadian Biomarker project funded by the Terry Fox Research Institute (TFRI, see www.tfri.ca/terryfox). Researchers were provided the executive summary of the proposal, as well as a work plan to address all facets of the proposed project. To become collaborators, COCRC members had to agree that all biospecimens would be openly shared within the COCRC, and the ultimate decision for access to the resource would be through a project management committee. This was central to the proposal, as biospecimens within the Canadian Ovarian Experimental United Resource (COEUR) would be exclusively reserved for the TFRI-funded program.
The Canadian consortium proposed to develop a pan-Canadian discovery and validation platform for biomarker research, and to use this biomarker platform to develop a molecular-pathology classification system for ovarian cancer integrated into clinical nomograms (decision making algorithms) for rational clinical management. Finally, the aim of the Canadian consortium is to integrate this correlative, preclinical initiative with prospective clinical trials in order to expedite the translation of research findings into clinical practice.
To ensure the success of the pan-Canadian ovarian cancer biomarker program, a series of actions was completed during the first year of the program that permitted it to be fully operational. Since the primary focus is on the correct pathological classification of specimens, coupled with clinical outcomes to identify samples belonging to both responders and nonresponders of first line therapy, an environmental scan of existing biobanks was conducted to identify samples to be reserved for the TFRI COEUR and to determine the means by which appropriate quality specimens and clinical data could be retrieved. Since the quality of research samples is critical to the success of the program, member biobanks were audited to ensure the quality of research materials using metrics relevant to anticipated future research assays. As a retrospective cohort of biobanked samples will be used, defining the level and variance in quality of existing materials is critical. As a first step, a test cohort of 135 high-grade serous ovarian carcinomas (HGSC) was assembled from samples obtained from each of the contributing biobanks. The quality assessment done in the preparatory phase of the repository collection is reported here.
Material and Methods
Participating biobanks
To date, the network consists of nine independent Canadian biobanks from four Canadian provinces that are committed to facilitate joint studies by working towards similar policies and quality assurance with the support of CTRNet (Canadian Tumor Repository Network, www.ctrnet.ca). These biobanks have all received ethics approval by their local ethics committees. General SOPs for all major biobanking activities are available at the CTRNet website. Additionally, the central laboratory work done for the COEUR study was approved by the Research Center review board of the Center Hospitalier de l'Université de Montréal (CHUM). Tumor samples were collected and banked, following appropriate written consent from patients undergoing surgery. Descriptions of participating biobanks are provided in Table 1.
Specimen collection and storage
Specimens were collected by trained staff in each participating center. Resected specimens were immediately transported from the operating room to the pathology department, where a pathologist provided an appropriate specimen to the biobank staff for immediate processing. When possible, time of the resection in the operating room and time of tissue processing by the biobank staff were recorded. CTRNet recommends that frozen tissue samples be placed into an empty cryovial, sealed, and immediately submerged in liquid nitrogen for at least 30–60 sec. Samples are then stored long-term in −80°C/-150°C freezers or liquid nitrogen. Formalin fixed-paraffin embedded (FFPE) samples were collected directly from samples processed within hospital pathology departments. A random selection of 15 HGCS cases per center was requested by the central site (Hôpital Notre Dame, CRCHUM), which were shipped on dry ice in accordance with the COEUR SOPs that were developed in collaboration with CTRNet to ensure uniformity in shipping of specimens. For the present study, a minimum size of 9 mm3 was requested for frozen tissues. The inclusion criteria for FFPE samples was a minimum tumor tissue size of 4 mm2. Upon receipt, frozen tissues were immediately stored at −80°C and matching paraffin blocks were stored at room temperature in a secure locker. All histologic slides were reviewed to ensure presence of available tumor tissue. An overall summary description of the collected samples is provided in Table 2. A description of how the specimens were handled and stored in each biobank is provided in Table 3.
Samples were categorized by Stage according to FIGO classification.
Follow-up time is the time from the date of primary resection of ovarian tumor until the event of death or last contact.
Sites are not listed in the same order as in Table 1.
All specimens were flash frozen and fixed with formalin buffer.
FT, frozen tissue; 4LN, liquid nitrogen.
RNA extraction and analysis
Total RNA was extracted from homogenized tumor tissue by a phenol-based extraction method with TRIzol
DNA extraction and analysis
Total DNA was extracted in accordance with CTRNet SOP# 8.2.004 and processed in accordance with SOP #5.1.002 (www.CTRNet.ca). Briefly, tissues were cut into small pieces with sterile scissors and incubated overnight at 55°C with 10 mM Tris pH 7.9, 2 mM EDTA pH 8, 40 mM NaCl, 0.8% SDS, and 0.4 mg/mL proteinase K. Tris-saturated phenol was then added and the solutions were mixed for 10 min on a rolling rack. Samples were centrifuged and DNA-containing supernatants were extracted with phenol, followed by phenol/chloroform/isoamyl alcohol (25:24:1) and chloroform/isoamyl alcohol (24:1), and then precipitated with 95% cold ethanol. The DNA pellets were resuspended in Tris/EDTA (TE) buffer and quantified. DNA quantification was assessed with the Nanodrop ND-1000 Spectrophotometer. DNA concentrations were estimated from absorbance at 260 nm. The A260/A280 ratios were also measured. Values for the A260/A280 ratio normally ranged between 1.8 and 2.1. After quantification, DNA was diluted in TE buffer to a working concentration of 100 ng/μl.
ß-Globin PCR amplification
To assess DNA quality, four different length fragments of the housekeeping gene ß-globin were amplified. The maximum amplicon size positively correlates with DNA quality. PCR amplification was performed with 100 ng of tissue DNA using the EconoTaq DNA polymerase (Lucigen, Middleton, WI); the primers are shown in Table 4. PCR was performed using the following conditions: initial denaturation at 95°C for 3 min, followed by 40 cycles of denaturing at 95°C for 1 min, annealing at 55°C for 1 min, extension at 72°C for 1.5 min, and final extension at 72°C for 5 min. PCR products were analyzed on agarose gels.
bp, base pair.
Tissue Microarray (TMA)
Following careful review of hematoxylin-eosin-stained slides, representative single cores (0.6 mm diameter) of each tissue sample were punched and arrayed in empty paraffin blocks. Tissue arrays, which were done in quadruplicate, were composed of 120 ovarian specimens per block. Fifteen cases were excluded because the tumor tissue size in the FFPE block was too small for four punches. The TMAs were then sectioned at 4 μm, stained with hematoxylin-eosin, and reviewed by a pathologist to confirm tumor content.
Immunohistochemistry (IHC)
The TMA slides were stained using the BenchMark XT automated stainer (Ventana Medical System Inc.). The antibodies used were anti-p53 (clone DO-1, Santa Cruz Biotechnology, Inc.), anti-WT1 (clone 6FH2, DAKO), anti-cytokeratin 7 (clone OV-TL12/30, NeoMarker), anti-Ki67 (clone SP-6, NeoMarker), and anti-E-cadherin (clone G10, Santa Cruz Biotechnology, Inc.). Antigen retrieval was carried out with Cell Conditioning 2 (VMSI; #950–123, Ventana Medical System) for anti-p53 and with Cell Conditioning 1 (VMSI; #950-124, Ventana Medical System) for all other antibodies. Prediluted antibodies were automatically dispensed, and the slides were incubated at 37°C for 30 min with the UltraView DAB detection kit (VMSI; #760–091, Ventana Medical System). Slides were counterstained with hematoxylin (VMSI; #760–2021, Ventana Medical System).
Staining quantification
TMA slides were scanned and converted into digital slides. Epithelial zones were scored according to the % of epithelial area stained. Each array was independently analyzed in a blind study by two independent observers. Inter-rating correlation was >75%. When strong differences in scoring between the two observers occurred, the core was re-evaluated to reach a consensus score.
Statistical analyses
The Pearson correlation test (two-tailed) was used to estimate the correlation coefficients. A Kruskall-Wallis test was used to estimate differences among the biobanks. The Mann-Whitney U test was used to evaluate the differences between one biobank and the others. All statistical analyses were done using Statistical Package for the Social Sciences software version 11.0 (SPSS, Inc.), and statistical significance was set at p<0.05. Hierarchical clustering analysis was carried out using Genespring™ software (Silicone Genetics) and a distance branch of 0.01 with a Pearson correlation as a similarity metric. Association between hierarchical cluster and disease recurrence interval was estimated using the Kaplan-Meier analysis and the log-rank test.
Results
DNA quality control
To evaluate the quality of the specimens collected for the COEUR repository and shipped to the central site, the quality of both DNA and RNA extracted from a set of HGSC frozen specimens was assessed. Each of the nine participating biobanks shipped 15 frozen specimens, and DNA and RNA extraction was performed on all 135 resulting specimens. The storage method, storage medium, processing time (time interval from surgical harvesting to storage in medium), and storage time in each site were recorded. One site provided specimens frozen in OCT medium (n=15, site #2), a second site provided some specimens stored in RNALater® solution (n=11, site #6), and the remaining sites provided specimens (n=109) that were flash frozen and stored at −80°C, −150° C, or in liquid nitrogen (see Tables 2 and 3). Since age has been reported as a factor affecting molecular quality, the effect of storage time on DNA/RNA integrity and immunohistochemistry staining was also evaluated. Most specimens were stored within 30 min after tissue resection (n=86, 83%), and were kept stored for more than 2 years prior to DNA and RNA extraction (n=64, 62%). After receipt of all frozen tissue specimens at the central site, samples were divided into two pieces for independent DNA and RNA extraction.
DNA was analyzed by the 260/280nm ratio and by PCR amplification of 4 fragments derived from the ß-globin gene (Fig. 1A and 1B). With the exception of one sample, DNA samples had a 260/280nm ratio ranging between 1.8 and 2.0. One sample showed a ratio of 2.09 (Fig. 1C), suggesting contamination during the phenol extraction. Following ß-globin amplification, the integrity of DNA was scored according to the number of amplified bands of increasing size from 1 to 4 (Fig. 1B). As seen in Figure 1D, 85.8% (n=115) of extracted DNA samples were of good quality with at least three amplified ß-globin bands of increasing size. Processing time from surgical resection to the biobanks had little effect on DNA integrity. Specimens processed within 30 min (81%) had at least three ß-globin gene bands, against 92% for specimens processed in more than 30 min (p=0.07). Similarly, time of storage had no significant effect on DNA integrity (p=0.16, Fig. 1E). The method of specimen storage either in OCT or in RNALater medium did not affect the quality of extracted DNA, although the temperature of storage did (data not shown). We noticed a higher number of samples with only one amplified ß-globin band in specimens stored at −80°C (n=14/69) compared to specimens stored at −150°C (n=1/19) or in liquid nitrogen (n=1/46) (p=0.001 Kruskal-Wallis test).

Integrity of DNA and RNA derived from epithelial ovarian cancer frozen tissues.
While some variation was observed in the number of samples with good quality DNA from different sites, there was no statistically significant difference in the 260/280 nm ratios (Fig. 1C, p=0.593, Kruskal-Wallis test). However, the PCR amplification of ß-globin gene fragments was globally less efficient for specimens from site #1 (Fig. 1F, p<0.001 Mann-Whitney test) because of a lower proportion of specimens from which four fragments could be amplified and higher proportion from which three fragments could be amplified. The number of poor DNA samples with one or two amplified fragments was not different from one site to another (p=0.114, Kruskall Wallis test).
Altogether these results show that there was no major difference in quality of DNA extracted from specimens collected at different biobanks.
RNA quality control
RNA quality was evaluated by examining ratios of ribosomal 28S/18S RNA and RIN values obtained by gel electrophoresis (Fig. 2A and 2B). Analysis of the ribosomal 28S/18S RNA ratios showed that 82% of extracted RNA (n=112 out of 134) had ratios above 1, and 63% of those (n=85) had ratios between 1.5 and 2 (Fig. 3A). The average RIN value of the 135 samples was 7 (range 2.4–9.5). Sixty percent of RNA samples (n=80) had RIN values of 7 or more, 31% (n=41) had RIN values between 4 and 7, and only 10% (n=13) had poor RIN values below 4 (Fig. 3B); a RIN value was not obtained for one sample. There was no correlation between RNA and DNA integrity (p=0.25, Pearson's test). There were only two specimens with low RIN values and less than 3 amplified ß-globin bands.

RNA integrity analysis method.

RNA integrity results from frozen HGSC specimens.
Next, the effect of storage time on the ratio of ribosomal 28S/18S RNA and on RIN values was assessed. As seen in Figure 3C, a trend toward a higher 28S/18S ratio was observed for specimens stored for 6 months or more when compared to those stored less than 6 months (p=0.057, t-test). Similarly, when RIN values were compared between these sets of samples, the difference in integrity was statistically significant (p<0.001, Mann-Whitney U test) (Fig. 3D). Due to the relatively low number of specimens stored for the shortest period of time (n=16), this result needs to be confirmed on a larger set of specimens. We also considered the processing time interval between surgery and storage (<30 min vs.>30 min) and did not observe differences in the 28S/18S RNA ratios or RIN values (p=0.67 t-test; data not shown). There were also no differences observed for specimens stored in OCT or RNALater® compared to flash frozen specimens, although the low number of specimens in each group (n=11 for OCT specimens) precluded rigorous statistical analysis. Similarly, we did not notice any effect of temperature storage on RNA quality (p=0.238 Kruskal-Wallis test).
When the quality of RNA samples was evaluated according to the site of specimen origin, we noticed a lower average ratio of ribosomal 28S/18S RNA for site #4 (p=0.002, U-Mann-Whitney test, Fig. 3E). Although the average RIN value was slightly lower for site #4 compared to the other sites (RIN=6.5±0.18, p=0.039, U-Mann-Whitney test) (Fig. 3F), when the number of samples with low or medium RIN values (<4 and 4 to 7, respectively) is considered, there was no significant difference for site #4. In contrast, we observed a significant difference in the RNA quality of samples from site #9, with a lower average RIN value (RIN=4.71±0.6) due to a significantly higher number of samples with low RIN values (p<0.001, U-Mann-Whitney test).
Immunohistochemistry staining on paraffin embedded tissues
Blocks of paraffin-embedded tissues were collected from the nine participating biobanks, for a total of 135 blocks. All tissue specimens were analyzed for morphology by hematoxylin and eosin staining to confirm that the sample contained sufficient tumor tissue for further analysis. One-hundred twenty blocks (91%) with enough tumor tissue for the construction of tissue microarrays with four representative cores per case were selected. Tissue microarrays were then examined by IHC for staining with biomarkers that could be used for ovarian cancer subtype diagnosis: WT1, cytokeratin 7, Ki67, p53, and E-cadherin. After review, eight specimens were excluded based on an erroneous assignment of tumor type: three clear cell carcinomas, four low-grade serous carcinomas, and one high-grade endometrioid carcinoma.
A total of 87.5% of all cases showed nuclear WT1 staining in more than 50% of tumor cell nuclei and staining was completely negative in only three samples (Fig. 4A). There were no differences in the expression of WT1 among the different sites (p=0.57, Kruskal-Wallis test).
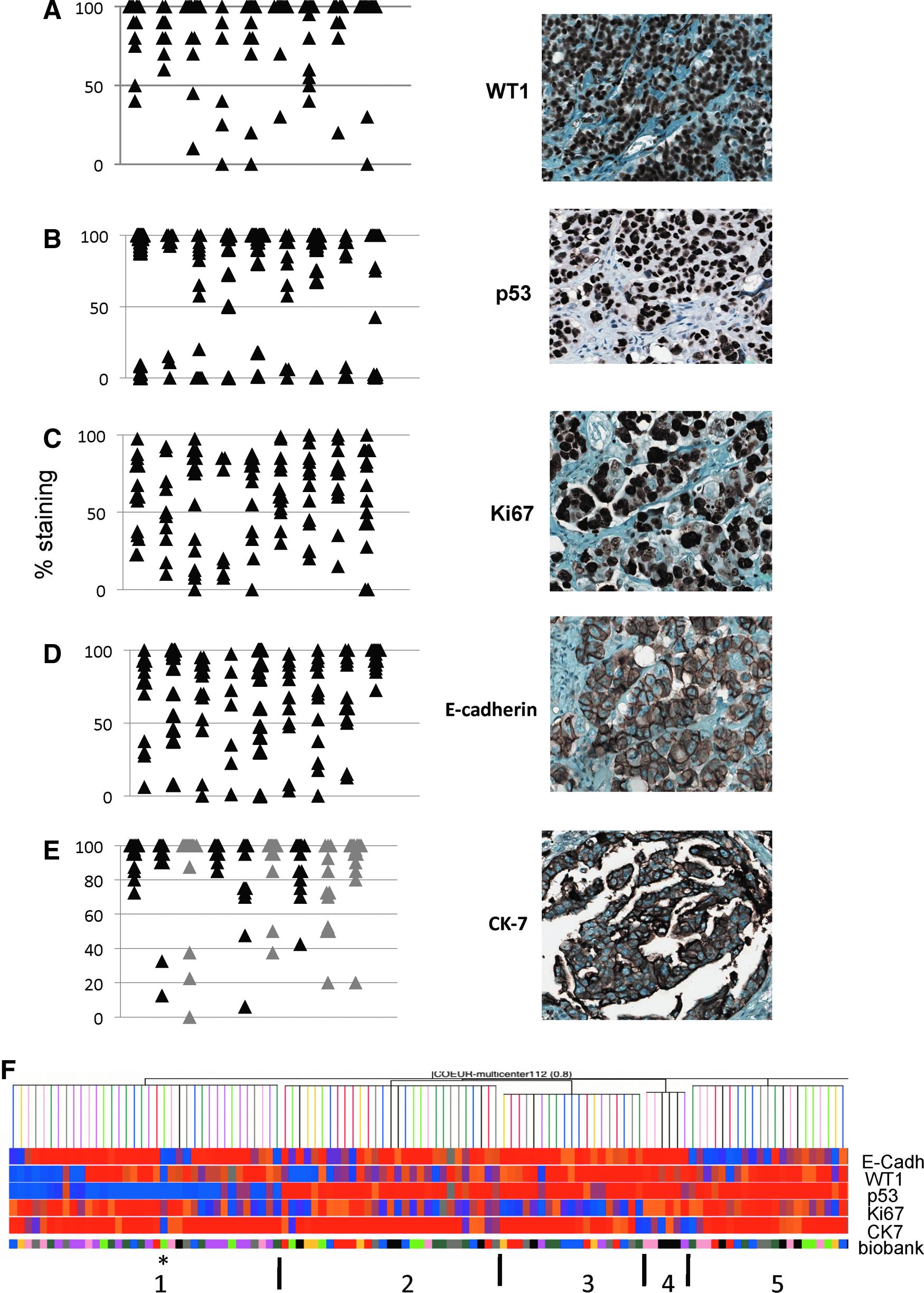
Immunohistochemistry results of TMA analysis with WT1, p53, Ki67, E-cadherin, and cytokeratin 7 (CK-7) stainings. Left panels show a graphical representation of the percentage of cells positively stained with antibodies; right panels show representative staining of positive cases:
Using a cut-off level of 50% of stained tumor cells as described elsewhere,6,7 we observed that 73% of cases were positive for p53 staining (Fig. 4B). There were no significant differences in the percent of nuclear p53 positive cores among the different biobanks (p=0.07, Kruskal-Wallis).
Ki67 staining was highly heterogeneous across the entire cohort with an average expression of 66% (range 0 to 100%) of positive tumor tissues (Fig. 4C). No significant differences were observed among the different sites (p=0.80, Kruskal-Wallis test). A similar observation was made for the staining of E-cadherin, with an average of 70% of positive cells in the whole cohort (Fig. 4D). The heterogeneity of staining was observed in each set of specimens from the different biobanks, with the exception of specimens from site #9, where a more homogenous positive staining for E-cadherin was observed (range from 70% to 100%, p=0.011 Kruskal-Wallis).
There was no significant correlation between immunostaining results and the age of FFPE blocks (p>0. 05 in all cases, Pearson test). Only a weak trend toward a decrease of staining with age was noticed for expression of CK7 (r=−0.183, p=0.065, Pearson test). Similarly, there was no correlation among the different immunostaining observed with the exception of the two epithelial mesenchymal transition associated proteins, WT1 and E-cadherin, which correlated positively (p=0.028, r=0.21, Pearson's test).
We noticed only one specimen negative for E-cadherin, p53, CK7, WT1, and weak for Ki67 (indicated with a star on Fig. 4F). This result is likely due to an anomaly in the quality of this FFPE sample.
To assess whether some specimens were of a different quality for immunohistochemistry staining, we also performed a nonhierarchical clustering statistical analyses using staining results for the five biomarkers (Fig. 4F). We observed five different clusters of specimens. These clusters did not separate the samples by biobank site: Cluster #1 was obviously related to low p53 expression, whereas cluster #4 was related to low expression of CK7, and cluster #5 to low expresion of E-cadherin (Fig. 4F). While cluster #2 grouped specimens with low WT1 staining and high p53 staining, cluster #3 grouped specimens with low Ki67, high p53, high WT1, and high E-cadherin. Interestingly, the clustering was strongly associated with the progression status of patients (r=0.30, p=0.004 Pearson's test) with all patients in cluster #2 (n=20/20) exhibiting disease progression. Altogether these results show that there were no significant differences in immunostaining of paraffin tissues among specimens from different biobanks, and that the differences observed were most likely related to the clinical status of the patients from whom the specimens were obtained.
Discussion
The aim of the present study was to determine the quality of tissues collected from different sites contributing to the COEUR cohort. No particular project or methology was considered at the time of collection of the original samples but a general goal to validate biomarkers in a large cohort was predefined. The main goal of the pilot phase of the project was to identify and ensure the quality of research materials. The results of this pilot study, which consisted of 15 samples per collection site representing a total of 135 cases, have confirmed that overall, good quality samples are being collected by participating sites. A total of 85% of extracted DNA exhibited acceptable quality for amplification of long fragments by PCR. As expected, there was more variation in acceptable RNA quality, with eight of nine sites having more than 80% of RNA samples of acceptable quality, as measured by RIN values. However, only 58% of RNA samples exhibited sufficient quality for more sensitive analysis (RIN>7). Only two sites provided specimens with less than 50% of RNA having acceptable RIN values. We could not identify a major handling parameter responsible for the lower RIN values. Other biobanks have reported on the quality of RNA obtained from prostate and pancreatic cancer tissues with RIN values >7 for 40% to 73% of derived RNAs.8,9 Even if all tissue types are not comparable due to their cellular content and other factors (eg, frequency of necrosis), our results show that cancer specimen collection across multiple centers should not create significant bias related to the quality of specimens or their derivatives.
The method of DNA and RNA extraction used here is simple and cost-effective, but may not be the most appropriate for all types of specimens. One parameter that was noted but not properly recorded, was the sample weight compared to the RNA integrity measured. It may likely be more difficult to extract good quality RNA from smaller samples. Tumor samples should be of a sufficient size to be processed for RNA using the Trizol reagent, and alternate methods of extraction should be employed when dealing with smaller samples (<10 mm3). A second parameter that is suspected to affect the quality of the specimens is the method of shipping, although each participating biobank followed the same specific SOPs. Either of these parameters may have caused the low quality of the RNA in the specimens from biobank #9. We did not observe any correlation between DNA and RNA integrity but suspect that DNA and RNA quality are sensitive to different handling or biobanking parameters. For example, one factor that was noted is the effect of storage temperature of biobanked tissues on DNA quality but not on RNA quality. While no significant effect was noticed on RNA quality, storage of tissues at −80°C was associated with lower DNA quality than tissues stored at −150°C or in liquid nitrogen.
Notably, we did not apply visual control of the frozen tumor specimens for cellularity. We think that a downstream measurement of DNA/RNA quality combined with a FFPE block from the same tumor area is a cost effective way for quality control. Less than 15% of samples were of insufficient DNA or RNA quality and/or did not have FFPE material for TMA construction. There was a substantial overlap (7%, n=9/135) in these cases, and those cases will be excluded from further analysis.
From our cohort of samples, DNA and RNA have been extracted from specimens stored for up to 9 years with satisfactory results (RIN value ≥7). We did not observe any negative effects on DNA, RNA, or immunostaining quality based on storage time. This observation has important implications for the future of COEUR activities, as our aim is to analyze specimens associated with clinical data, and a follow-up period of at least 2 years. However, it should be noted that our quality control assessment was limited to nucleic acid integrity and did not take into consideration changes in gene expression that may have occurred during tissue collection and processing. Indeed, external factors such as methodology of tissue collection, and methodology of tumor resection, including time of resection, may affect gene expression,3–5 although this factor has been reported to have little effect in ovarian cancer tissues.10–12
The result of a central pathology review of FFPE specimens showed a relatively low initial misclassification (5% of non-HGSC specimens). Considering the difficulty in the differential diagnosis of high-grade serous cell type from high-grade endometrioid cell type, this result was very encouraging.13–16 . Although the diagnosis of histological type is reproducible,15,17 there are challenges to discriminate HGSC from low-grade serous carcinomas and clear cell carcinomas in rare instances. 18 Knowing that clinical behavior of ovarian cancer patients is highly dependent on tumor subtype, an accurate diagnosis is necessary for more appropriate clinical patient management. This observation emphasizes the need for biomarkers in the accurate classification of epithelial ovarian cancers. 19
Satisfactory results were also obtained on tissue integrity by immunohistochemical analysis. A relatively high quality of tissue was noted with our panel of five biomarkers. Only one case was antigen deficient for four of five markers, and insufficient for protein detection by IHC. There was no correlation between staining pattern of tissues and age of FFPE blocks or participating site, with the exception of CK-7, but rather staining distribution correlates with the outcome of patients (p=0.0016, Log Rank).
WT1 is considered a marker of serous cell lineage. It is positive in 80% of serous tissues, usually negative in clear cell carcinomas and focally positive in some endometrioid tissues.6,12,20–22 Low WT1 expression has been associated with a poor outcome of serous patients.6,23 In our cohort, using the same cut-off value previously used by others,6,23 95% of tissues were positive for WT1, with very little variability among tissues from different biobanks, possibly indicating an increased sensitivity for our WT1 nuclear positive immunohistochemical protocol. A cut-off of 68% of WT1-positive nuclei was associated with disease recurrence (p=0.004, Log Rank), confirming a previously reported observation. 6
We observed 73% of cases positive for p53 nuclear signal, which is similar to a previous report (58% in 502 HGSC from multiple sources). 15 The staining of p53 was not associated with disease recurrence as previously reported by others in a high-grade serous cohort, 6 suggesting that the present cohort is representative of a larger cohort and has not been biased by the selection process. We noticed a more homogeneous staining of E-cadherin in specimens from site #9. A deeper analysis should be conducted to determine the parameter influencing this result. In view of a recent report, 24 we can speculate that time of fixation may be involved. Indeed, Khoury et al. 24 showed that delay of fixation of more than 2 h induces a reduction of E-cadherin staining, but this reduction is not observed for p53 or Ki67. While it is often difficult to collect information about fixation time in a retrospective cohort of specimens, the result obtained here indicates that this parameter should be recorded whenever possible. Despite differences in staining levels, we did however note that in this pooled cohort high expression of E-cadherin was associated with a better prognosis of patient (Log Rank=4.53, p=0.033), as previously reported by others.25–28
Altogether these results demonstrate the idea that construction of a large, homogeneous cohort from multiple centers is feasible if stringent entry controls are applied. The freezing and storage of ovarian cancer specimens in Canadian biobanks is now conducted following established SOPs developed by CTRNet to support biobanking activities and to provide good quality samples. However, there is significant variation in the details of pre-acquisition protocols for paraffin embedded-tissues used in different institutions, especially in pathology departments. The present study shows that, even when using a combination of collection and storage methods, good yields of high quality specimens can be obtained when appropriate protocols are followed. In addition we found that collection of specimens from several biobanks instead of from one site is time and cost effective and may allow collection of specimens with longer follow-up in a shorter period of time, facilitating predictive and prognostic studies. However, it remains possible that for a particular downstream biomarker assay, site-specific effects may be observed. The ability to analyze data by site, and to control for any site-specific bias, will be incorporated into all studies associated with the resource.
A review of the recent literature shows that quality control of specimens from multicenters is not reported and may not be assessed. However, our results suggest that this is an essential step to estimate the overall quality of the collection and the outcome that could be obtained. It is an essential prerequiste before initiating a research project to know the nature of the biological materials being accessed and whether this material is appropriate for the techniques employed during the research project.
Footnotes
Acknowledgments
We thank the Gynecology-Oncology and Pathology services of all participating centers for tumor procurement. We are also grateful to all COCRC and laboratory members for tissue processing and thoughtful discussions. Tumor banking was supported by each provincial organization described in ![]() . Clinical specimens from the province of Quebec were provided by the Banque de tissus et de données of the Réseau de recherche sur le cancer of the Fonds de recherche du Québec–Santé which is affiliated with the Canadian Tumour Repository Network. This work was supported by a grant from the Terry Fox Research Institute.
. Clinical specimens from the province of Quebec were provided by the Banque de tissus et de données of the Réseau de recherche sur le cancer of the Fonds de recherche du Québec–Santé which is affiliated with the Canadian Tumour Repository Network. This work was supported by a grant from the Terry Fox Research Institute.
Disclosure Statement
No competing financial interests exist.