
Abstract
Currently, there are no surgical strategies to treat tracheal lesions longer than 7 cm. Such patients are not candidates for tracheal resection or end-to-end anastomosis and are thus left with only repeated palliative procedures to relieve their respiratory insufficiency. Experimental studies using cryopreserved trachea have produced contradictory results, limiting the clinical application of this technique. We evaluated caspase-3 expression and the histological integrity of canine tracheal cartilage cryopreserved using two different solutions, two temperatures, and varying lengths of storage time. Thirty canine tracheal segments of 5 rings were studied. Group 1: Control without cryopreservation. Groups 2 and 4: Cryopreserved in F12K media with 20% fetal bovine serum (FBS) at −70°C for 48 hours. Groups 3 and 5: Cryopreserved in 90% FBS at −70°C for 48 hours. Groups 4 and 5 were then stored for 15 days in liquid nitrogen. All of the segments were thawed, fixed in wax, and cut into rings. Three rings were selected for caspase-3 expression and histological evaluation. Staining of cartilage matrices was significantly modified in the tracheal segments of Group 5. The central region of the cartilage ring was more vulnerable to the effects of freezing than the edges. Under the same cryopreservation temperature and storage time, tracheal cartilage integrity is better preserved when F12K media is used. Caspase-3 expression is not related to cartilage injury from the cryopreservation process.
Introduction
The most common cryopreservation solutions used in experimental trachea preservation are Roswell Park Memorial Institute (RPMI)-1640, Dulbecco's Modified Eagle's Medium (DMEM), and Tissue Culture (TC)-199 combined with fetal bovine serum (FBS) and dimethyl sulfoxide (DMSO). 1 For clinical applications, 90% FBS is routinely used for human stem cell cryopreservation, 3 and Kaighn's Nutrient Mixture F-12 media (F12K) has been successfully used in tissue engineering, articular chondrocyte cryopreservation, and recently in tracheal cryopreservation. 4 Tracheal segments are cryopreserved between −80°C and −100°C and then stored in liquid nitrogen. However, long storage times exert a deleterious effect on the cartilage. 5 Articular cartilage injuries do not heal, and large defects result in osteoarthritis. Osteochondral transplantation is an effective treatment for long, large defects, but its use is limited by the inability to store cartilage for long periods of time. 6 Different cryopreservation solutions, cryoprotectant media, and thawing conditions have been evaluated. 7 The freezing and thawing process results in increased cellular death by apoptosis and necrosis. In mammals, there are two pathways to the start of apoptosis, converging in caspase-3 activation, which acts as the primary inducer of cell death. 8 Caspase-3 is implicated in tissue damage due to ischemia 9 and reperfusion, 10 orotracheal cannulation due to the tidal volume effect, 11 and the freezing and thawing processes inherent in the cryopreservation of different tissues and cells. 12 Thus, we chose to study caspase-3 expression in the remaining viable cartilage cells of cryopreserved tracheal segments. The aim of this work is to evaluate microscopic changes in tracheal cartilage preserved under four different cryopreservation protocols, using different cryopreservation solutions, storage times, and temperatures.
Material and Methods
The protocol was reviewed and approved by the Ethics Committee of the INER (Instituto Nacional de Enfermedades Respiratorias “Ismael Cosio Villegas”) and carried out under the Technical Specification for the Care and Use of Laboratory Animals of the Mexican Official Norm 13 and the Guide for the Care and Use of Laboratory Animals prepared by the U.S. National Institutes of Health. 14
Tracheas weighing between 15 and 20 kg were harvested from 6 healthy, mongrel dogs without regard to sex or age. Prior to surgery, solids were withheld for 24 h and fluids for 12 h. Initial anesthesia was induced by intravenous administration of 0.1 mg/kg xylazine hydrochloride (Bayer, Leverkusen, Germany) and 6 mg/kg propofol (PiSA, Jalisco, Mexico). Anesthesia was maintained using propofol (2 mg/kg/min), taking care to maintain spontaneous breathing to avoid orotracheal intubation. Anesthetized animals were placed in the supine position. The neck of each animal was shaved and prepared with a povidone-iodine solution (EQM, DF, Mexico). A vertical incision was made in the anterior face of the neck. The cervical trachea was exposed after separating the strap muscles and was thoroughly dissected. Before harvesting the entire trachea, euthanasia was carried out using an IV pentobarbital overdose and 1 mg KCl (PiSA). The surrounding tissue was dissected from the trachea on a cold mayo table, and the trachea was trimmed into 5-ring segments and rinsed with a 50% glucose solution (PiSA) with 5000 IU heparin (PiSA) and 0.1 ml/L of antibiotic-antimycotic solution (Sigma, St. Louis, MO). The tissues were randomly assigned to the control group or to one of the four cryopreservation groups. Two cryopreservation solutions were investigated: a) F12K media (Gibco, New York) and 20% FBS (Gibco) and b) 90% FBS (Gibco). DMSO (Sigma) was added to both solutions at a 10% concentration along with 0.1 mL of antimycotic-antibiotic solution (Sigma). Tracheas were transferred into cryogenic vials (Nalgene, NY) and cryopreserved at −70°C overnight using a high-density polyethylene vial holder with a controlled-rate freezer (Nalgene 5200 Cryo 1°C; Thermo Scientific Nalgene Mr. Frosty Freezing Containers). The next day, tracheas were transferred to liquid nitrogen (-196°C) and maintained there until analysis.
Study groups
Group 1 (n=6): Noncryopreserved control group. Tracheal segments were washed with a 50% glucose solution (G1: Control). Group 2 (n=6): Tracheal segments were cryopreserved in F12K media containing 20% FBS at −70°C for 48 h (G2: F12K). Group 3 (n=6): Tracheal segments were cryopreserved in 90% FBS at −70°C for 48 h (G3: FBS). Group 4 (n=6): Tracheal segments were cryopreserved in F12K media containing 20% FBS at −70°C for 48 h and then immediately stored in liquid nitrogen at −196°C for 15 days (G4: F12K+LN). Group 5 (n=6): Tracheal segments were cryopreserved in 90% FBS at −70°C for 48 h and then immediately stored in liquid nitrogen at −196°C for 15 days (G5: FBS+LN).
Histological and caspase-3 evaluations
Control Group (G1): After harvesting, tracheal segments were rinsed with a 50% glucose solution (PiSA) and fixed with 10% buffered formalin for 24 h. Cryopreserved groups: At the end of the cryopreservation time, tracheal segments were thawed to 37°C and fixed with 10% buffered formalin for 24 h. The 1st, 3rd, and 5th rings (proximal to distal) were taken and dehydrated in ascending grades of ethanol (Golden Bell, Jalisco, Mexico); cleared in xylol (Reasol, DF, Mexico); embedded and blocked in paraffin wax (McCormick Scientific, St. Louis, MO); cut into 2 μm- and 4 μm-thick sections, and mounted on glass slides with a rotating microtome (Reichert, New York).The tissues were then processed for histological evaluation with hematoxylin and eosin stain (Merck, Darmstadt, Germany), and for caspase-3 expression. Histological assessment included staining of the cartilage matrices and measurement of the percentage (average of three counts) of nucleated chondrocytes and degenerated cells in the central and one of the two extreme regions of the cartilage rings (chosen alternately at the time of assessment) (Fig. 1).

Caspase-3 expression in the cartilage was determined by immunohistochemistry using a polyclonal antibody [Caspase 3 (CPP32) Ab-4, Rabbit Polyclonal Antibody, Neo Markers, Lab Vision, Co. RB-1197-P, Kalamazoo, MI]; the biotin-avidin-peroxidase system (Vector, California), staining with amino ethyl carbazole (BioGenex, California), and double staining with hematoxylin (Vector, California). Negative and positive controls for caspase-3 expression were included in all tests. Caspase-3-positive chondrocytes were counted using an optical microscope (Carl Zeiss, Jena, Germany) and a manual cell counter (Fisher Scientific, Waltham, MA). The area of every tracheal cartilage ring was measured using an image digitizer (Image Pro Plus Version 4, Media Cybernetics, Georgia) to determine the cellular density of caspase-3-positive chondrocytes per mm2.
Statistical analysis
Statistical analysis was performed using SPSS 6.1 (SPSS, Inc., Chicago, IL). The ANOVA+Tukey and Spearman tests were used to compare the histological changes. A value of p<0.05 was considered statistically significant.
Results
Histological evaluation
The process of cryopreservation caused significant changes in the cartilage tissue from Groups 3 (FBS), 4 (F12K+LN), and 5 (FBS+LN). (Control group vs. Groups 3, 4, and 5: p<0.01, ANOVA+Tukey and Spearman). In Group 3 (FBS), the changes were observed in the matrices of isolated isogenous groups. In Group 4 (F12K+LN), the staining changes were found in several continuous isogenous groups proximal to the perichondrium, whereas in Group 5, the staining changes were found on the chondrocytes situated proximal and distal to the perichondrium (Fig. 2).
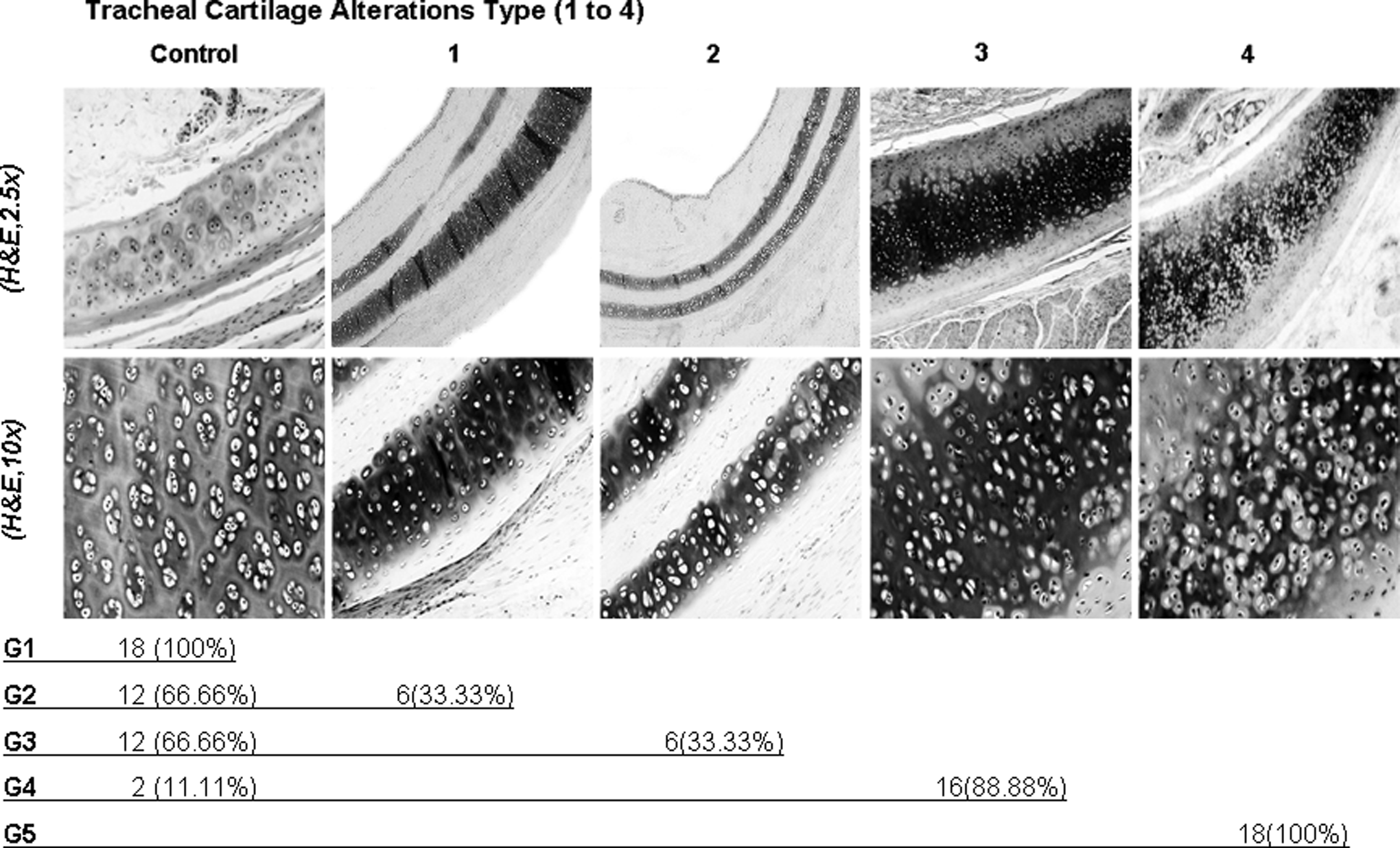
Type of alterations. Type 1: Normal without alterations; Type 2: Alterations proximal to one perichondrium; Type 3: Alterations proximal to both perichondriums; Type 4: Alterations on all the cartilage. Number and (percentage) of cartilage rings with staining alterations in the pericellular, territorial and interterritorial matrices. G1 (Control); G2 (F12K); G3 (FBS); G4 (F12K+LN); G5 (FBS+LN).
Cell degeneration
The mean percentage of normal or “unaltered” chondrocytes and degenerated cells obtained at the center and at both extremes of the cartilage rings are reported in Table 1. The tracheal segments of the control group showed the highest percentage of nucleated chondrocytes at the extremes of the cartilage ring, but this finding was not significantly different when compared to all cryopreservation groups.(Control group vs. Groups 2–5, p>0.05, ANOVA). In all of the cryopreservation groups, the percentage of nucleated chondrocytes in the central region of the cartilage ring was significantly diminished due to the freezing effect (Cryopreservation groups 2–5 vs. control group, p<0.001, ANOVA) regardless of cryopreservation storage time, temperature, or cryopreservation solution. In all of the groups, the percentage of nucleated chondrocytes was significantly higher at the extremes of the cartilage ring than in the central region, and the percentage of cellular degeneration in the central region of the cartilage ring was significantly higher than at the extremes (p<0.001, ANOVA+Tukey) regardless of the position of the cartilage ring in the tracheal segment (1st, 3rd, or 5th) (p<0.05, ANOVA+Tukey).
p<0.001, ANOVA, degenerated cells vs. control group.
Caspase-3 expression
We observed that two segments in the control group (G1), one in Group 2 (F12K), and one in Group 3 (FBS), were positive for caspase-3 expression in the chondrocytes. The positive cellular density for caspase-3 expression in the 1st, 3rd, and 5th tracheal rings was not significantly different (p=0.926, ANOVA+Tukey). The mean positive cellular densities for caspase-3 in the cartilage [number of chondrocytes that expressed caspase-3/cartilage area (mm2)]±SE for the study groups were G1: 0.163±0.097, G2: 0.150±0.074, G3: 0.109±0.061, G4: 0.155±0.062, and G5: 0.000±0.000, indicating no significant difference (p=0.05, ANOVA+Tukey) (Fig. 3).

Cryopreserved tracheal cartilage from Group 3 (FBS) kept at minus; 70°C for 48 h with positive immunoreactivity in the chondrocytes (arrows). Aminoethylcarbazole-hematoxylin staining under
Discussion
We evaluated the histological changes and caspase-3 expression in tracheal cartilage after cryopreservation at −70°C, using F12K or FBS media along with DMSO, with or without further liquid nitrogen storage. Our results show that tracheal cartilage storage in liquid nitrogen induces significant changes in the basophilic staining of the extracellular matrix. Hematoxylin acts as a basic dye with a positive charge density, binding to anions (sulfates, phosphates, and carboxylic groups) that are contained in the extracellular matrix of the cartilage, primarily to the sulfated glycosaminoglycans, which are part of the proteoglycans, hyaluronic groups, and chondroitin sulfate. The changes to the matrix staining in this study may be the result of alterations of the components that give the cartilage its consistency and may have the capacity to re-model the extracellular matrix of the cartilage, which results in cartilage degenerative changes. These changes are more severe when FBS is used as the cryopreservation media along with liquid nitrogen storage. While 90% FBS media has been successfully used to cryopreserve stem cells, 3 it appears to be useless in tracheal cartilage preservation. This discrepancy can be explained because there are no stem cells in the adult trachea, and we cryopreserved long tracheal segments (4–6 cm long). Similar findings have also been reported by Pegg et al., 15 although it is relatively straightforward to cryopreserve isolated living chondrocytes. At this time, there is no satisfactory method to preserve surgical grafts between the time of harvesting or manufacture and actual use. In contrast, the FBS concentration in the cryopreservation solution has an important role in cartilage preservation. The addition of FBS at a concentration between 10% and 30% of the F12K media promotes the growth of articular chondrocytes. 16 The osteochondral grafts preserved for 28 days at −4°C with nutrients supplemented with 10% FBS maintained proteoglycan synthesis and better viability compared to those in serum-free media. 17 Nevertheless, it has a negative effect, as the FBS seems to act as an immunogenic factor carrier.17,18 In this study, damage to the cartilage was observed after cryopreservation of tracheal segments in 90% FBS vs. F12K media. Although the cell cultures were supplemented with serum to support their attachment and proliferation, serum may be a potential source of foreign protein contamination that could cause a nonphysiological response in the chondrocytes when the tracheal segments are cryopreserved in a high concentration of FBS. The articular chondrocytes cultured in solutions with FBS showed a significant decrease in viability, proliferation, and cellular adhesion,18–20 as well as the loss of cartilage genic information. 18 The alterations of the chondrogenic markers and the expression of metalloproteinases as well as the cartilage matrix are not established; the articular chondrocytes cultured in solutions supplemented with autologous serum or FBS-free solutions show better preservation results.19–21
We also found that in all of the study groups, the best preserved chondrocytes (nucleated chondrocytes) are located in the extremes of the ring. The central region shows an increase in cellular degeneration, suggesting that the mechanisms of protection and penetration of the cryopreservation solution into the cartilage during the freezing process are not homogenous. It has been reported22,23 that during the process of freezing articular cartilage, the chondrocytes located in the superficial or deeper layers retain their normal structure, but those located in the intermediate layer are damaged. It appears that the chondrocytes located in the intermediate layer are more susceptible to the damage caused by the cryopreservation process, suggesting that there are biological and/or biophysical differences among the chondrocytes located in the different morphological zones or layers. The chondrocytes proximal to the surface show improved recovery after ice formation. 22 The addition of DMSO to the cryopreservation solution increases cartilage viability in the cells located in the superficial layer of the cartilage matrix, but not in the cells located in the central zones. 23 The cells and tissues can be preserved at low temperatures using cryoprotective agents to limit the harmful effects of ice crystals that can form during cooling processes, but the difficulties in tissue preservation have significantly limited the application of this technique. Cryopreservation of large tissues is hampered by a lack of knowledge of the permeation kinetics of cryoprotectant agents within these tissues.7,24 Successful cartilage cryopreservation is limited by the time required for cryoprotective agent (CPA) permeation into the matrix and high CPA toxicity. 25 Jomha et al. 24 evaluated the amount of cryoprotective agent within the matrix of dowels of porcine articular cartilage (10 mm diameter). They determined that the DMSO diffusion coefficient at three different temperatures (4°, 22°, and 37°C) was 2.4–6.2×10−6cm2/s, and the activation energy was 4.33 kcal/mol. 24 DMSO does penetrate into this tissue very rapidly. According to Jomha et al., 24 cryopreservation of the articular cartilage with a rapid-cooling technique and high concentrations of DMSO resulted in partial vitrification of the matrix and significantly less matrix disruption. It appears that successful cryopreservation of viability and function in articular cartilage will require high concentrations of cryoprotectants and rapid cooling. 26 Moreover, chondrocytes were shown to tolerate 10% or 20% DMSO and were not unusually susceptible to osmotic stress. An experiment in which the effects of freezing with 10% DMSO to −50°C were separated from the effects of the concomitant rise in solute concentration showed that the injury was associated with the formation of ice. Freeze substitution microscopy showed that large ice crystals were formed within the chondron, some within chondrocytes, even when the cooling rate was optimal for isolated chondrocytes. It is proposed that the nucleation and preferential growth of ice within the chondron (rather than the surrounding acellular matrix) is responsible for the very poor survival of the chondrocytes in situ using the current methods of cartilage cryopreservation. 15
Pegg et al. 27 reported that chondrocytes are not unusually susceptible to osmotic stress; in fact, they appear to be particularly resistant. It appears that the damage in the matrix is associated with the formation of ice, even at cooling rates that are optimal for cryopreservation of isolated chondrocytes. The current methods of cartilage cryopreservation involve the nucleation and growth of ice crystals within the chondrons rather than restriction of ice to the surroundings. Some tissues, such as the cartilage and cornea, carry an internal fixed negative charge, leading to a swelling pressure that is balanced by tensile stress in the tissue matrix. During the addition and removal of cryoprotectants, changes in osmotic pressure cause the tissue to deform. Because of the fixed charge and osmotic deformation, the permeation process in such tissues differs from ordinary diffusion processes. It has been shown that the friction between water and cryoprotectant has the greatest influence, but the fixed charge density is also important.28,29 For some tissues, the preservation of mechanical properties is critical; for others, it is not. These considerations are crucial for the design of preservation methods for specific tissues. Bone tendon and skin can provide useful grafts in the absence of living cells, which may be true for cardiac valves; the crucial requirement is that the mechanical properties remain intact. Simply freezing at approximately −80°C may be sufficient. In contrast, many cell systems and all metabolizing organs do require healthy cells to function. Cryopreservation is often an effective remedy for isolated cells (e.g., hemopoietic stem cells), but the damaging effects of ice formation are sufficient to rule out this approach for whole vascularized organs and for some tissues. The site of ice crystal formation is crucial. 30
In spite of the thawing time, normal tracheal tissue structure was maintained without any sign of cartilage fracture, and the airway remained permeable. Several research groups have found damaged trachea cartilage with cryopreservation temperatures between −60°C and −140°C, with and without liquid nitrogen storage, and they have concluded that the damage is the result of the storage time. 1 We found that with a cryopreservation storage time of 15 days, the histological changes of the tracheal cartilage are primarily the result of the cryopreservation solution and storage temperature but not the cryopreservation storage time. Pérez et al. 16 avoided the use of cryoadditives or liquid nitrogen storage for tracheal cryopreservation using rapid cooling and storage at −80°C for 2 weeks. They reported that the quality of cryopreserved tracheal cartilage was disappointing, similar to the quality obtained using conventional slow-freezing protocols. The chondrocytes reside within the cartilage matrix and maintain their structure. The cryopreservation of tracheal and articular cartilage could improve long-term transplantation outcomes if the cell and matrix integrity could be maintained. The extra-matrix ice plays an important role in cell damage during cryopreservation that results in significant cell loss. We previously reported that caspase-3 expression in the epithelium of the submucosa and in tracheal glands is decreased as a result of cryopreservation time and temperature, 4 but it was unchanged in the cartilaginous tissue. The use of FBS as a cryopreservation solution and liquid nitrogen storage of the trachea segments caused severe changes in the integrity of the matrices of the cartilage, independent of the effect of cryopreservation on caspase-3 expression.
Footnotes
Author Disclosure Statement
No competing financial interests exist.