
Abstract
Biobanking research seeks to improve the diversity, availability, and quality of human specimens critical for translational research, including biospecimen collections from disadvantaged minorities. American rural whites are seldom represented in such initiatives as geographic isolation makes obtaining informed consent challenging. We report a case series of 83 newly diagnosed cancer patients, attending a rural community medical center, who consented to participate in cancer research. To enable pooling with population studies, we created a BioGeoBank using 2007 NCI and ISBER Best Practices, after a protocol approval by Eastern Maine Medical Center (EMMC) IRB and OHP HRPO. Informed consent forms were at Flesch-Kincaid 8th Grade reading level, supplemented by NCI educational brochures. Of 108 patients identified, 85 were eligible. Of these, 83 patients (49 lung cancer, 21 breast cancer, and 13 other cancers) consented to donate data, blood, and tissue specimens for future research, and maintained eligibility. Two years later, we executed a legacy protocol to transfer specimens to NCI's biorepository. Of the 69 surviving patients, 9 patients could not be contacted. All those contacted (60) agreed to provide additional data on environmental risks, and consented to specimen transfer. Self-organizing map analyses showed no evidence that age, education, income, familial susceptibility, or lifestyle factors were associated with consent to donate data or biospecimens. Cancer cases reported 1–3 co-morbid chronic diseases (mostly cardiovascular), near lifetime smoking and/or alcohol consumption; familial cancer risks, and many had a prior cancer history. Anecdotally, willingness to consent was based on altruistic hopes that research would generate knowledge to reduce cancer incidence. Our study shows that cancer patients from disadvantaged white rural communities with health disparities associated with geographic isolation are motivated to consent to participate and support biobank research.
Introduction
To help address this need, we created a new biospecimen and data collection bank, the BioGeoBank, to support environmental cancer research relevant to rural populations with health and cancer disparities. The BioGeoBank linked residual surgical tissue specimens of rural patients with cancer in Maine, with clinical and behavioral data, and environmental geocoded information. Maine, the northernmost Appalachian mountain state, is predominantly rural, with among the lowest recruitment of cancer patients and elderly subjects in the US. 13 Because few studies have reported on recruitment and consent of rural patients with health disparities for biobank research, we recruited newly diagnosed cancer patients at a rural community tertiary medical center, to investigate their willingness to consent to data and biospecimen collection for research. We found that, despite their geographic isolation, patients with cancers and other co-morbidities consented to biobank research, and selected opt-in/opt-out choices of what to donate. Multivariate analysis of cases by a self-organizing map showed no significant associations among advanced age, education, income, tobacco or alcohol exposure, the number of family relatives with cancer, or travel distance, and willingness to participate in biobanking for cancer research.
Methods
To facilitate screening, patient recruitment and specimen and data collection for the BioGeoBank, collaborations were established with EMMC and Saint Joseph's Hospital (SJH) surgeons, CancerCare of Maine, and Dahl Chase Pathology Associates (DCPA), a pathology service, based at EMMC. Regulatory approval was obtained and updated annually by EMMC IRB and the Office of Research Protection (ORP) Human Research Protection Office (HRPO). Assent and consent forms were approved; one adolescent participated in the study. The protocol excluded (1) incapacitated individuals unable to provide informed consent if no legally authorized representative (LAR) was available or if the LAR denied participation, and (2) specimens and data that failed to meet quality control standards. Vital status for BioGeoBank participants is transferred on an annual basis from the EMMC Cancer Registry to the BioGeoBank.
Clinical biobank staff screened EMMC patients whose cancer diagnosis required tumor resection as the first stage of treatment, and identified 108 candidates. Surgeons, mostly in EMMC Respiratory Medicine or in EMMC Breast and Osteoporosis Center which operates at SJH, informed potentially eligible patients of the study. Interested participants contacted study staff. Patients agreeing to participate were consented at their next clinic visit; alternate provisions were made when this was not possible. BioGeoBank staff explained the study; provided education materials that included a description of the study protocol, an informed consent form (Table 1), and a NCI educational brochure on biobanking; and answered questions either on site or by telephone. Participants approved blood collection at the time of data collection or prior to surgery, and specimen collection during surgery. A study nurse coordinated the patient's appointment to sign informed consent forms prior to surgery, and notified the clinical lab to harvest up to 40 mL additional blood, after collection of diagnostic samples.
Because travel distances and/or the cost or means of transportation were obstacles hurdles for some patients, the letter of enrollment provided after patients consented offered the option of working with BioGeoBank staff at the hospital, by telephone, or at home to complete data collection. Questionnaires 1, 2, and 3 in the original study (Table 2) required about 30–60 minutes to complete. The fourth questionnaire (Table 2), administered when we re-contacted cases after 2 years, was completed in less than 30 minutes. We used NCI Cancer Bioinformatics Grid (caBIG) bronze-level certified Clinical Research Management Systems (CRMS) software (Medical Decision Logix, Inc., Baltimore, MD), to develop questionnaires, protocol, and data templates, and to capture questionnaire and specimen information. To ensure that Protected Health Information was securely exchanged within and between HIPAA-compliant entities, the software package used Transport Layer Security, a cryptographic protocol that provides security and data integrity for communication over Transfer Control Protocol/Internet Protocol.
Procedures, annotations, and access to specimens conformed to ISBER Best Practices 14 to facilitate pooling with population studies. Biospecimens were bar-coded with unique numbers and linked to clinical, pathological, environmental, and geocoded data in CRMS. The BioGeoBank barcode replaced the patient identification at the time of specimen receipt by the pathologist. Following surgical resection of the tumor, tissue samples were delivered to DCPA within 15 min for EMMC cases, and within 40 min for SJH cases. To be eligible for archiving, tumor tissue remaining after removal of diagnostic pathology specimens had to be at least 0.5 cm3. After a 2-week hold required for diagnostic pathology, formalin fixed, paraffin-embedded (FFPE) specimens were transferred to BioGeoBank laboratory storage at room temperature. Blood was processed as whole blood, white cells, plasma, and serum aliquots; derived specimens were stored in cryogenic freezers (Custom Biogenic Systems, CBS, Romeo, MI). Blood that was processed for RNA analyses was stored in a designated −80 Revco freezer.
After 2 years of operation, our parent company closed the research laboratory due to financial exigencies, resulting in the loss of processing and storage equipment for banked specimens. Because our protocol named the location of storage, the IRB required us to contact cases to obtain approval to transfer specimens to NIH NCI Tissue Repository. Our ongoing quality control showed a need to collect data not in the original protocol as well as missing data. The IRB approved the protocol revisions. The study coordinator re-contacted surviving patients to request consent to collect additional data and approve specimen disposition. Complying with our Legacy Plan SOP, we executed a formal Materials Transfer Agreement with the NCI Tissue Repository such that the Repository accepted custodianship of the physical specimens as a de-identified collection, while the Institute, now a virtual organization, retained custodianship of all BioGeoBank data.
To understand relationships underlying the phenotype of consenting cases, we used descriptive statistics and a self-organizing map (SOM). A originally developed by Kohonen, 1 is an unsupervised neural network that generalizes principal components analysis (PCA) to analyze multi-dimensional datasets. A neuron, or node, is a d-dimensional weight vector, [m1, m2…… md], where each mi is an input vector. By associating a distance function with weight vectors, similar neurons are iteratively moved closer in the global space, and dissimilar neurons are naturally separated. When training is complete, the global space represents both quantitative and topological or connectivity relationships among neurons. We selected age, education, and income as “social status nodes” and marriages, the number of family relatives with cancer, tobacco and alcohol exposures, and Body Mass Index (BMI) at 18 and time of current diagnosis as “stressor/risk nodes”, and used the SOM outcomes to determine if consent status clusters by phenotype. Consent status was defined on the basis of opt-in choices for data, blood, and tissue donations.
Results
Of 108 participants consented, 85 met eligibility criteria; of these, 83 (98%) white men and women consented to participate in biobank research (Table 3). Of those who did not participate, 4 did not meet eligibility criteria (1 case had received neoadjuvant therapy, and 3 died prior to entering the study); and 19 cases failed to maintain eligibility (8 patients died after study entry but before providing biospecimen and data, while Pathology excluded 11 consented cases because cancer diagnosis was not confirmed) (Table 3). Because of limited public transport, many patients arranged private transport to drive up to 150 miles to the medical center for surgery (Fig. 1). When informed consent was not integrated into an office visit, patients living at a distance required a more flexible process to participate. We addressed this by successfully offering telephone interviews, home visits, or Internet options, according to patient preferences. Once enrolled, patients showed little interest in how specimens and data were used, and were surprised that we needed to re-contact them for actions not originally described. Two years later, we contacted participants to ask consent to complete an additional questionnaire and to transfer banked specimens to NCI Cancer Tissue Repository. In the interim, 23% had died. Among the 69 survivors, 60 (87%) responded by phone or mail, and consented to our request (Table 3). Patients remained cooperative and willing to participate. The latest vitality update in 2012 showed 40% of the original case series had died (Table 3).

Map of Maine to illustrate geographic isolation and distance from the single interstate highway and Eastern Maine Medical Center (EMMC: red star) cases had to travel from their residential zip code (concentric circles are 25 miles apart). Brown: Appalachian mountains; Gray lines: county boundaries; Blue bubbles represent zip codes of cases, with the size of the bubble representing the number of cases from that zip code; Red line: Interstate 95, the only major federal highway in Maine. Southern Maine's boundary ends at the Atlantic coast; southeast (straight) boundary of Maine map abuts New Hampshire; remaining Maine map boundaries represent the frontier with Canada.
Not eligible (Prior neo-adjuvant therapy: 1; Died prior to study entry: 3); **Failed to maintain eligibility (8 died after study entry before completion of questionnaires and/or tissue collection, and histopathology of resected tissues failed to confirm cancer in 11 cases).
Cases providing informed consent, data, and biospecimens included 18 men with lung cancer, 31 women with lung cancer, 21 women with breast cancer, and 7 men and 6 women diagnosed with other cancers. Cohorts ranged from 1917 to 1994. Of 83 consented cases, blood and tumor tissue biospecimens were obtained from 63, blood specimens only from 8, and tissue specimens only from 2 cases. Ten cases donated only data, due to physician decisions reserving specimens for diagnostic needs.
Characteristics, such as age, cohort, education, income, reported by others as deterrents to participation, did not appear to influence consent in this case series. Of consenting participants, 68% were aged 60 years or older (Fig. 2A). Lung cancer cases averaged 69 years of age (95% confidence interval (CI): 67, 72 years). Breast cancer cases were younger, averaging 58 years (95% CI: 54, 62 years). The 13 cases with other cancers averaged 57 years (95% CI: 44, 70 years). Cases had lived in Maine for 36–60 years. Of 83 cases, 47 (57%) had attended or completed high school (Fig. 2B). At incomes of $25,000 or less, approximately 25% of cases were living at or below the weighted average poverty threshold of the 2011 US Census for households of up to 4 people (Fig. 2C). Cases reported long-standing tobacco and/or alcohol (80%) exposures at much higher frequencies than state or US averages reported by CDC BFRSS (Table 4). All cases reported some form of health insurance; 41% reported Medicaid/Medicare coverage, 31% reported Medicare with private insurance supplementation, 27% reported private insurance, and 1 case was enrolled in the US Dept. Veterans Affairs program.
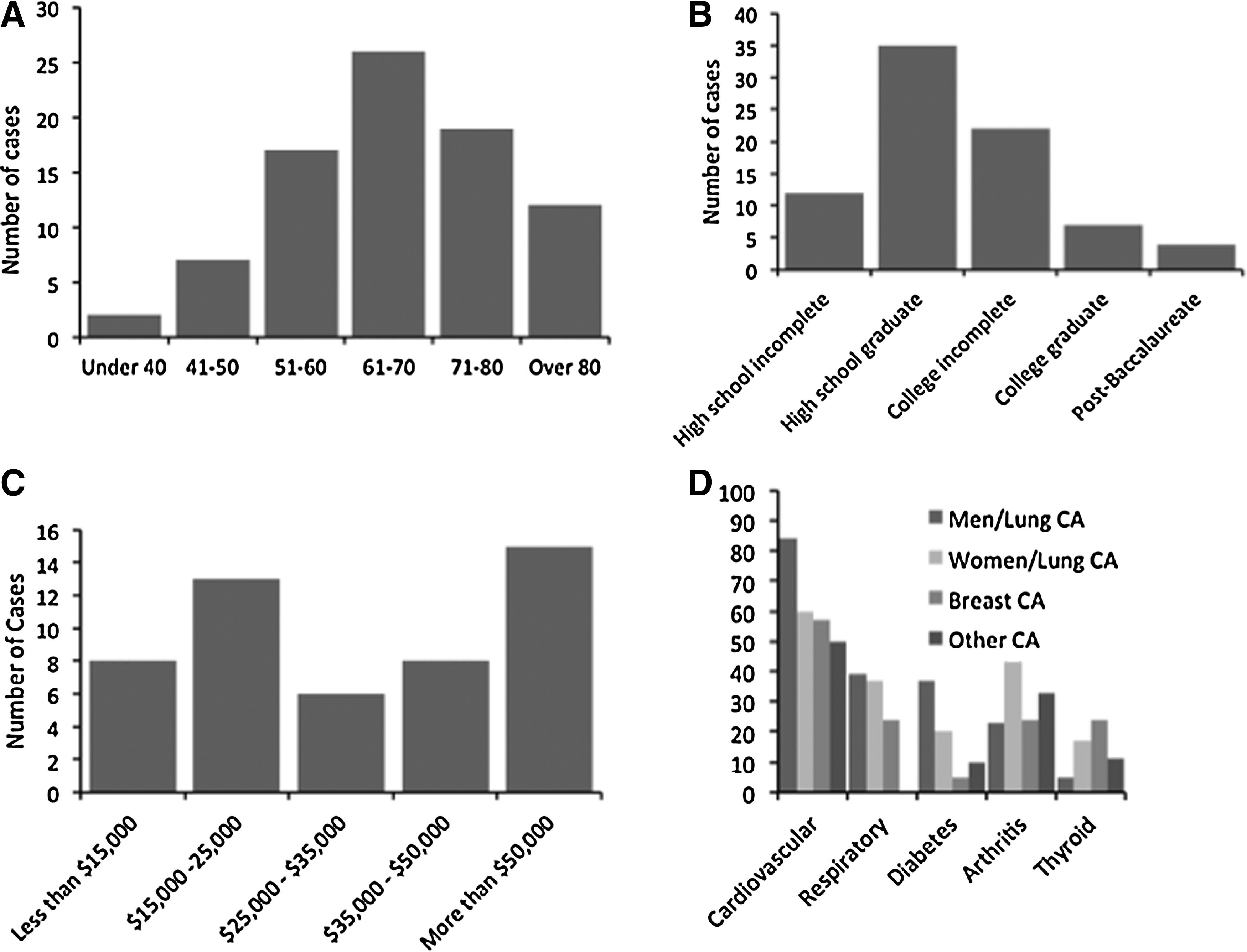
Frequency distribution of cancer patients to show age range
The self-organizing map showed several associations within the overall phenotype of those consenting to biobanking research (Fig. 3). Tobacco exposure and pack-years were associated, displaying the same increasing trend from bottom right to top left of the respective component planes (Fig. 3). Alcohol exposure is only partially associated with tobacco exposure, so that heavy tobacco users may or may not be heavy alcohol users. Higher income associated with completion of post-baccalaureate education. Self-reported BMI at diagnosis was not associated with self-reported BMI at 18 years of age (Fig. 3). Of the 78 cases who reported BMI at the time of diagnosis, 29% men with lung cancer, 72% women with lung cancer, 74% women with breast cancer, and 54% men and women with other cancers reported overweight or obese BMI. An inverse association was suggested between number of first-degree relatives with cancer and education level achieved, as the component plane's values of the former increase from right to left, while the component plane's values of the latter increase from left to right. Evaluation of the labeled cells indicating the relative positions of neurons indicated that donation of data, blood, and tissue, DBT, does not trend with any of the input vectors (Fig. 3). This analysis showed that a subject appears equally likely to participate fully in the study, regardless of educational or financial attainment, tobacco or alcohol exposure, or age, number of marriages, or number of first-degree relatives with cancer.

The Self-Organizing Map presents quantitative and topological outcomes for each of the ten input vectors and the corresponding cell positions of the neurons, labeled according to donating data (D), blood (B), and/or tissue
Health was compromised by multiple co-morbidities in most cases (Fig. 2D). Of the 83 cases, 65% men and 81% women reported two or more co-morbidities, while 4% men and 0.05% women had no co-morbidity. The most common co-morbidities were cardiovascular disease (58 cases, 70%); chronic respiratory diseases (23 cases, 28%); diabetes (14 cases, 17%); arthritis (22 cases, 28%); and thyroid disease (11 cases, 13%) (Fig. 2D). Women with lung cancer reported the most co-morbidities per case (3.2±0.3), while women with breast cancer, who were 10–20 years younger, reported fewer co-morbidities (2.1±0.3). Cases reported widespread use of narcotics (41% of cases) up to 4 years prior to diagnosis, with longer duration of use in lung cancer cases compared to breast cancer cases (Table 4). Compromised health, as manifested by multiple co-morbidities and the use of narcotics, which can be debilitating, did not deter cases from providing consent to participate.
Employment status did not appear to impact willingness to consent. We investigated industries and occupations, but no consistent patterns were observed for either men or women that might explain their willingness to consent to participate in biobank research.
In this case series, we found no bias, aside from a high frequency of cancer within families, that characterized participants in their willingness to consent to biobank research that requested biospecimens, clinical data, and extensive questionnaires. Anecdotally, participants told us that family cancer history rates and their own prior history of cancer prompted their willingness to participate in research.
Discussion
Because genetic ancestry and epigenetics research are revealing the importance of contributions of diverse human populations, especially those with health disparities, biobanking has a key role to play by providing high quality biospecimens with robust phenotypic data.12,15–17 Few cancer research studies discuss the practical recruitment and consent of individuals to participate in biobanking, especially of patients from rural regions with health and cancer disparities. Poverty, lack of educational attainment, distance to the health clinic, and geographic inaccessibility have all been suggested as potential barriers to recruiting humans with health disparities.18,19 The Southern Community Cohort Study, whose enrollment of 73,700 adults with health disparities included 70% African Americans, reported 90% agreed to participate in biobanking. 19 Our case series extends these findings in rural Whites, and provides additional information. In a rural state with cancer and health disparities related to geographic isolation, poverty, and access to care, White patients newly diagnosed with cancer participated in biobanking research, and were willing to be contacted on multiple occasions, irrespective of distance from the medical center, advanced age, education, and income, family history of cancer, and a history of prior cancers, or number of first-degree relatives with cancer.
The NCI Iowa Agricultural Study of rural farming communities reported that 16,535 farmers, representing 77% of total eligible candidates, consented to the study but only 50% completed take-home surveys.20.21 A small subset also donated specimens for cancer risk research, but the percent consenting was not reported. 22 The willingness of humans who live in rural, less farming-dominated regions of the US, to participate in biobanking and cancer research has not been characterized. Like Maine, central Appalachia has a distinctive culture of independence, resilience, and determination, and residents have concerns about environmentally-related cancer risks. 6 Compared to our more limited Maine dataset, population research studies in central Appalachia on rural whites with high cancer rates, high tobacco and alcohol use23,24 showed lower educational attainment and more widespread poverty.
Based on CDC SEER cancer statistics, Maine has consistently been among the 8 states with the highest lung cancer rates in the US. Because many of our cases reported living in Maine for more than 75% of their lives prior to diagnosis, we speculate that awareness of the high rate of cancer in Maine may also contribute to their decision to participate in cancer research biobanking.
Scientific literature speculates that personal, familial, and social altruism in older cancer patients are likely interdependent reasons for giving informed consent and participating in research. 25 Yet, in a study of reasons underlying donating cancer tissue in New South Wales, Australia, altruism and social exchange only partially explained participants' reasons for donating tissues. 26 Authors speculated that psychological rewards may underlie willingness to participate in biobanking research, as tumor tissue normally discarded during surgery acquires value when used in cancer research. 26 A Netherlands study specifically addressing informed consent procedures for follow-up and patient preferences reported that, while 99% of 264 cancer patients provided informed consent for biospecimen research, 59% preferred to have an opt-out option where they did not need to be further informed of the fate of their donated tissues or of additional studies that included their banked specimens.27,28 Studies specifically investigating patient preferences recommend that, because a small minority feel strongly about re-contact, opt-in/opt out clauses should routinely be incorporated into consent documents.27–30 Of our 60 cancer survivors contacted for additional consent, only one opted out of consent to transfer specimens to a federal biobank.
In conclusion, we find that cancer patients from a rural region were willing to consent to participate in research; their decision held across time when re-contacted for consent to additional procedures, and there were no consistent associations between selected lifestyle behaviors, social status, stressors, or risk factors that described a phenotype of those consenting.
Footnotes
Acknowledgments
We gratefully acknowledge the help of clinical research staff at Eastern Maine Medical Center (EMMC) CancerCare of Maine who screened, recruited, and consented patients at the start of the study, allowing us to comply with EMMC requirements for patient screening. We thank EMMC surgeons in Respiratory Medicine and The Breast and Osteoporosis Clinic who helped in patient recruitment.
Disclosure Statement
This work was funded by US Army Medical Research and Materiel Command research contract USAMRMC No. 0704400, PI JM Hock, and done at the Maine Institute for Human Genetics and Health, Bangor, ME. The authors report no conflict of interest.