
Abstract
Over the past 5 years, using European and North American biobanks as models, the grass-roots establishment of independently operating biobanks has occurred virtually simultaneously in large Israeli teaching hospitals. The process of establishing a national biorepository network in Israel has progressed slowly, sustained mainly by a few proponents working together on a personal level. Slow progress has been due to limited funding and the lack of a legal framework specific to biobanking activities. Recently, due to increasing pressure from the scientific community, the government has earmarked funds for a national biorepository network, and the structure is now being established. In forming a network, Israel's biobanks face certain difficulties, particularly lack of support. Additional challenges include harmonization of standard operating procedures, database centralization, and use of a common informed consent form. In this article, we highlight some of the issues faced by Israel's biobank managers in establishing and sustaining a functional biobank network, information that could provide guidance for other small countries with limited resources.
Introduction
I
The idea behind the establishment of a network of biobanks for medical research in Israel is not new. With interest in studying common diseases and the Ashkenazi population in Israel, IDGene Pharmaceuticals Ltd., took the first steps to establish a biobank for epidemiologic studies. Funding difficulties forced the company to halt activities in 2005. The impetus for a biorepository network in academic institutions in Israel did not come until 2008 when large teaching hospitals started to form independently-run institutional biobanks, which became aware of each other largely by word of mouth. Network establishment has been a slow process, with many challenges. The altruistic, collaborative attitude necessary for a network biorepository to succeed runs contrary to a longstanding competitive tradition, and this has impeded progress. The cooperative efforts of the institutional biobank managers, spearheaded by leaders in the scientific community, most notably Nobel laureate Aaron Ciechanover, led to a concerted effort to convince government officials to fund a national biobank infrastructure as part of its support for biomedical research. A 10-year, phased plan to create a fully-functional, six-hospital network for biomarker discovery that is depicted by a simple arrow diagram was used in early discussions with government officials (Fig. 1). However, the course of events did not entirely follow the original plan envisioned. In this article, we describe the steps taken in various areas to advance the establishment and sustainability of a functional biorepository network in Israel.

Initial 10-year plan of operation for a biobank network.
Challenges and Progress
Funding and structure
Phase One: Stand-alone, hospital-integrated biobanks
During the first 2–3 years of operation, the funding for biobanks in Israel's two most active biorepositories (at Sheba Medical Center and at Hadassah-Hebrew University Medical Center) has been through a combination of philanthropic donations, in-hospital support from research and development departments, and short-term grants. These two separate pilot projects began sample collection almost simultaneously at Hadassah-Hebrew University Medical Center in early 2008 and at Sheba Medical Center in late 2008.
At Hadassah-Hebrew University Medical Center, combined start-up funds of US$700,000 were allocated over 7 years; this covered salaries for one full-time manager who functioned during the preparatory phase between 2005 and late 2006, one full-time technician (who also served as patient coordinator), a part-time data manager whose office space required construction, one small liquid nitrogen tank, a computer, consumable equipment, a promotional brochure, and a request for proposals from software companies. After two years of preparation during 2005 and 2006, it was decided that the managerial salary cost was too high, and this function was turned over to a full-time pathologist already working within the Department of Pathology. The manager, who was paid two extra “on-call” duties per month for one year, has remained as manager on a voluntary basis since 2008. It is recognized that this arrangement would be unsustainable in most medical centers. Certain expenses (listed as “other” in Table 1), are viewed as investments for the future, including the production of a promotional brochure for potential funders, a request for proposals for a software application (later shared with Sheba and Rambam Medical Centers), and host expenses for meetings including those for the Marble Arch International Working Group, held in Jerusalem, in November 2010,
FT, full time; PT, part time; RFP, request for proposals for software application; K, thousand.
At Sheba Medical Center, start-up funds (US$700,000 for 5 years) were separated into two stages. In the first, US$250,000 were allocated to cover the purchase of freezing equipment, consumables, and salaries. For the first 18 months, a full-time manager was responsible for institutional review board (IRB) applications, patient recruitment, blood sample processing, and data management. A pathologist worked half-time in the operating room to procure tissue specimens. In the second stage (3.5 years), an additional US$450,000 were allocated to cover salaries (full-time manager, full-time pathologist, part-time technician, and full-time coordinator), consumables, and the first biobanking conference in Israel (Table 1).
A hematology biobank was established at Rambam Medical Center in 2011, using the in-house research laboratory infrastructure, hospital funding for one half-time technician, and grant support for a part-time manager and consumables. The hematology biobank has collected blood and bone marrow samples from 1200 donors with various hematological malignancies.
At Sourasky Medical Center in Tel Aviv, 12 small, previously established biorepositories in separate departments (2000 samples in total), were completely funded by research grants.
To summarize, hospital-based biobanking in Israel began as fragmented activities in various departments of large teaching hospitals such as Hadassah-Hebrew University Medical Center in Jerusalem and Sheba Medical Center in Ramat Gan. No formal analysis of demand was ever conducted within these centers. However, toward the mid 2000's, increasing demand from academic researchers and occasional inquiries by industry led to attempts to centralize biobanking efforts within each medical center through cooperation between oncology and pathology departments. This led to a somewhat more organized structure within each hospital, so that investigators both inside and outside the medical center were aware of whom to contact when they wished to acquire specimens for their projects. After several rounds of submission and revision, IRB applications to create centralized biobanks were approved, and thus biobanking began, on very limited funds, in the two hospitals; an additional two hospitals (Rambam and Sourasky Medical Centers) followed shortly thereafter.
Phase Two: Creating a national network
Over time, while separate biobanking activities were underway, a joint effort had been continuously ongoing to enlist government support. As it was apparent that without substantial financial support from the government, centralized, in-hospital biobanking would be unsustainable, and a national network would forever remain a dream, increasing pressure was placed on key individuals in the Office of the Chief Scientist of the Ministry of Health. In addition, in mid-to-late 2009, meetings began with an advisory committee with tremendous influence on where to place government funds for one large project annually (National Infrastructures Program). The advisory committee members included scientists, pharmaceutical industry representatives, and economists. Based on previous experience, an estimated budget of US$16M USD over 10 years was presented. After completing its own analysis, the committee recommended that funds be set aside for a national biobanking network. Thus, the joint efforts of competing institutions culminated in a major breakthrough.
In January, 2012, Israel's Ministry of Industry, Trade, and Employment, in conjunction with the Ministry of Health, issued a call for proposals for up to six collection centers to form a centrally-managed, national biobank to support cancer research. Four major medical centers, each with smaller affiliated hospitals were chosen: Sheba Medical Center in Ramat Gan, Hadassah-Hebrew University Medical Center in Jerusalem, Rambam Health Care Campus in Haifa, and Sourasky Medical Center in Tel Aviv; these centers will share approximately US$ 9–10 M over 3 to 5 years, to build a functional biorepository infrastructure. The new network (Fig. 2) named MIDGAM (an acronym for the Hebrew word meaning “samples”), will have a board of directors to oversee central management. Central management will be responsible for quality management, maintenance of a central database, oversight of the collection centers, education and training, interaction with the public and the press, governance, and implementation of standard operating procedures across the network. A partially rotating scientific and ethical advisory board will function as a tissue allocation committee.
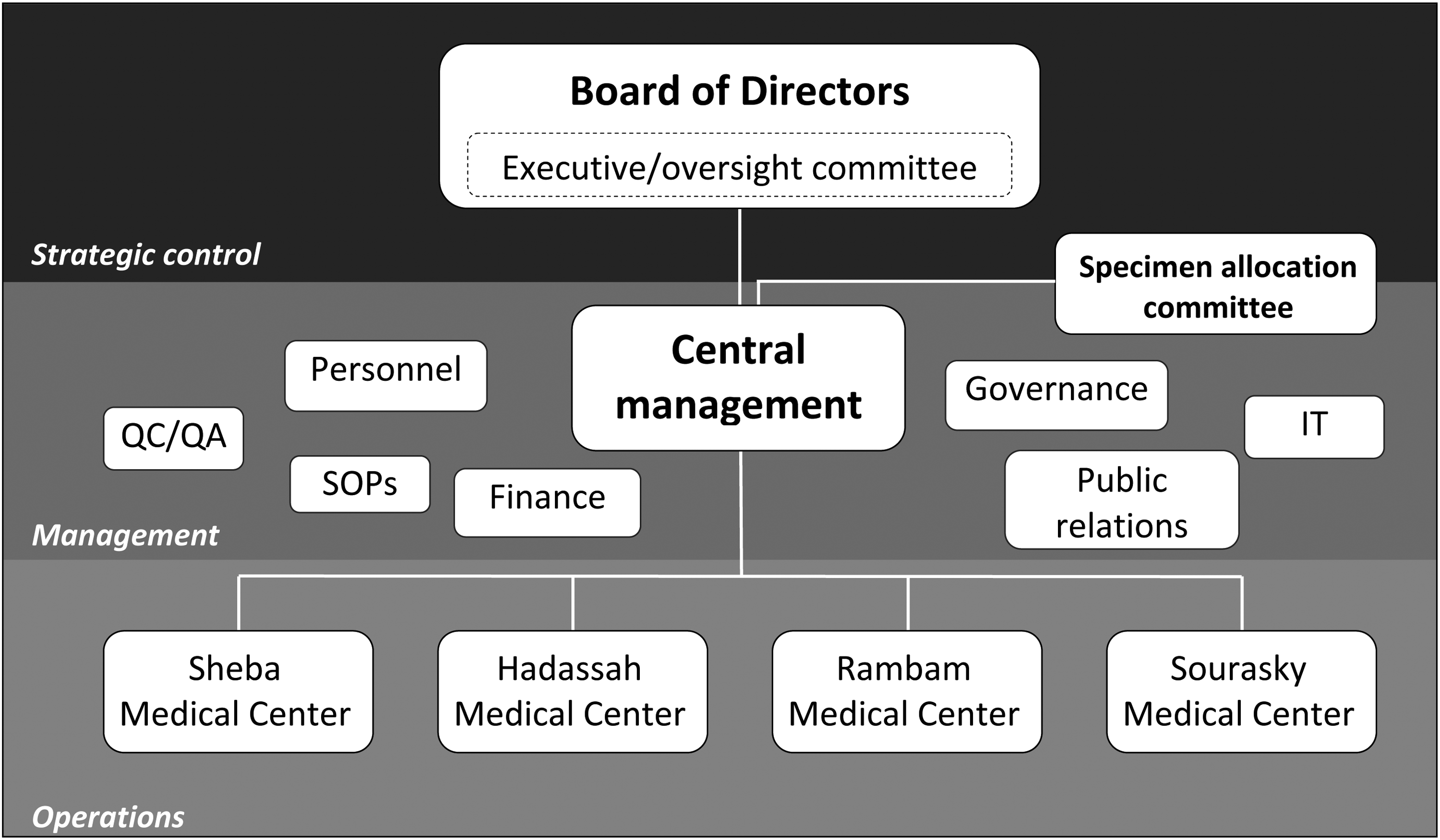
Overall structure of the Israel Collaborative Bioresource for Research & Development (MIDGAM).
As this sum is low compared to that invested in biobanking by some European governments, the available funds will have to be allocated carefully (Table 2). Table 3 shows a 5-year estimate of the cost of equipment and consumables for a center collecting specimens from 1000 patients per year. While the estimated cost is approximately US$750,000 over 5 years, the allocation is approximately US$320,000 (US$270,000 for equipment plus consumables, and approximately US$50,000 to cover software application implementation, and quality management measures), creating a shortfall in equipment funding. Since the centers already have some basic equipment, consumables, and most importantly, momentum, this shortfall is less burdensome than for a center which would be starting from scratch.
General manager allocated full time for the first 2 years, half time for the next 3 years.
Each site is expected to partner with one smaller collection site.
The new network will have characteristics of a number of biobank types. 3 First and foremost, it will be a partnership between institutions. Material will be stored in separate sites with a central coordinating hub for network administration. Information sheets and consent forms will be identical. Similar protocols are being developed for implementation across-the-network, and a central catalogue of samples will be maintained.
Since newly recruited patients will sign a consent form specific to the network, the historical collections will not be part of the new national network effort. However, the historical samples will be available for researchers upon specific request to the in-hospital biobank manager. Since the biobank is generally retrospective, there is some concern that collectors may be deterred. While we have recently experienced a slight drop in collection in the historical banks in anticipation of the formation of the new network, the addition of new, motivated collectors who were not previous collectors in the existing banks should ameliorate this problem. We expect different departments within each institution to view the biobank as both a contribution network as well as a “bring-and-share” network. The fee schedule for contributors, such as surgeons who also participate in research, will be adjusted accordingly. The network will also be partially a catalogue network, with a searchable database of samples for researchers. As pointed out by Shickle et al., 3 information technology (IT) compatibility remains an obstacle and is one of the first priorities so that data mining will be possible in the future. While return of data generated through sample use will be requested in the Israeli network, the mechanism for the receipt of these data has not been determined.
Since Israel has never before had a national biobank network, the participating historical banks and their managers are, in a sense, also creating an expertise network, particularly around ethics and governance. Recently a standardized informed consent form has been approved by the Ministry of Health, and the individual biobank managers are actively involved in establishing the procedures required for IRB applications for new biobanks. There is active promotion, and a desire to increase understanding of biobanking within and among the various hospital ethics committees in the hospitals involved in the network. Individuals involved in the national biobanking initiative are also actively involved in reviewing the recently proposed changes to Israel's Genetic Information Law, as well as the upcoming proposed changes to the Ministry of Health's regulations for research involving human subjects.
Despite the temporary financial relief over the next 3–5 years, hospital-based biobanks in Israel will continue to function on limited funds. The global economic crisis has affected Israel's financial resources for biomedical research. The sums invested in biomedical research in Israel have traditionally been low, and with severe economic cut-backs expected to take effect in 2013–2014, additional sources of funding will be scarce. Since most grants awarded for biomedical research in Israel range between $10,000–$100K USD, fees for service cannot be expected to serve as a viable cost-recovery option.
Sustainability, one of the main challenges of the new network, will require survival tactics such as focusing on project-driven collection, encouraging industrial–academic collaboration, promoting in-hospital visibility to hospital management and research and development departments, and building goodwill among hospital staff who are often asked to perform tasks outside their regular duties. Salaries are the major expense in biobanking (75%), and oftentimes one employee must fill several job descriptions. In times of acute financial strain, collecting formalin-fixed paraffin-embedded tissues and relevant data provides a cheaper, less labor-intensive alternative to cryopreservation, although this is a relatively high price to pay when the routine of collecting fresh tissue and blood samples is impaired.
While the government funding agreement is for a period of 3 to 5 years, the biobank network will be expected to sustain itself after this period. This is unlikely to be achieved while maintaining peak levels of activity. Under the Total Life Cycle Cost of Ownership model for long-term projects, 2 the steady-state phase of operation is only achieved after a period of 5 years. Since some basic equipment and in-hospital experience have accrued over the last 5 years of early activity, a steady state at the national level may be reached within 3 years. However, efforts to remain viable must remain focused on two areas:
1. Maximizing collection and distribution turnover. Within each hospital, the largest number of participating departments as possible must be recruited as contributors to the bank, and as many investigators as possible must be encouraged to use the collected materials. A significant public relations investment must be made to encourage collectors, users, and donors. This will reduce the number of aged, high-quality specimens with long-term follow-up. To minimize this problem, data collection for living donors will have to continue after specimens have been depleted. It may also be necessary to focus on prospective collection for specific projects for which the bank may receive a portion of the project's funding.
2. Cost recovery measures. The minimum operating cost to keep the in-hospital biobank at Hadassah-Hebrew University Medical Center (650 beds) viable (albeit on a very “low-flame”), is approximately US$100,000 per year. In larger centers such as Sheba Medical Center (1800 beds) and Sourasky Medical Center (1300 beds), the cost is likely to be much higher. Although not optimal, charging end-users for services associated with biobanking as a cost-reimbursement strategy is both equitable and necessary. A public–private partnership is legal in Israel, and will most likely be necessary, with appropriate material transfer agreements in which costs to industry are much higher than costs to academic users and those from other not-for-profit organizations. Other potential sources of revenue 2 such as expert pathology services, extraction of customized data sets, and assistance with IRB applications for outside investigators will be explored.
Technical Issues and Considerations
Database
Like many biobanks early in their life cycle, we began using Excel spreadsheets to store data while deciding on common data elements and desired reports. In each hospital, patient data (identifiers, demographics, family history, past medical history, habits, medications, allergies, relevant biochemistry, and follow-up data) as well as specimen data (pre-analytical variables, pathology, and inventory), are currently stored. Investigator requests and projects data are stored separately since the files quickly grew to be too large and unmanageable. A request for proposals was circulated to several Israeli companies that vied for a contract to build a software application from scratch, at high cost, amidst an economic downturn which further limited biobanking budgets. Although this has not been a palatable situation, a similar situation limiting other small-country-based biobanks is likely. In Israel, the primary languages of communication are Hebrew and Arabic, and finding commercially available software to support non-Latin-based languages in addition to English has been a major challenge. In addition, local technical support has not been an option for North American and some European companies. However, in recent months, with increasing globalization of markets, software and technical support have become available, and they will be implemented in the coming months with government support. The application will most likely be acquired from a company outside of Israel, with Israeli clients in the biotechnology industry, which will allow some Hebrew to be inserted in some of the fields. The application can track both patient data and sample data, and be used to manage investigator projects. A minimum data set for all samples should be adopted before entry into the database.
Standard Operating Procedures (SOPs) and harmonization
To establish working models, the managers of stand-alone, hospital-based biobanks visited several biobanks in North America and Europe. The host biobanks were very generous in sharing their perspectives on biobank establishment and operation, as well as on specific issues such as informed consent, equipment, software, and personnel. While the biobanking community has guidelines and ideals regarding harmonization, it is still far from unified and there are many approaches to several of the technical aspects of biobanking. To avoid reinventing the wheel and adding further variability, SOPs and their formats were adopted from established banks and biorepository networks. However, since Israel's biobanks have been separate entities, the SOPs and their formats come from different sources, including primarily the Canadian Tumor Repository Network (CTRNet) 4 and MD Anderson Cancer Center, Houston, Texas. An effort is currently ongoing to harmonize the SOPs and their formats to be used by all biobanks in Israel.
Pathologists have been critical to the function of the institutional biobanks in Israel since their inception. The pathologists sample all tumors (except brain tumors, typically sampled by the neurosurgeon), and regularly perform quality control testing to confirm diagnoses, and quantify tumor content on samples requested by investigators. The cooperation of the pathologists is crucial for the success of the network. In November 2012, an update on the progress of the national biobanking network was presented at the meeting of the Israel Association for Pathologists, and was very well received.
Eventually, we envision an environment in which all medical institutions and pathology departments across Israel will either participate in the network, or form new networks. While a harmonized “network of networks” such as exists in Spain 5 may be beyond Israel's scope, we strive to emulate many of the positive aspects of open sharing of samples and data across the country. 6
Ethical, Legal and Social Considerations
International harmonization of biobanks will hopefully lead to increased international collaboration. What can and cannot be done with human biological samples depends on the legal and ethical framework for such activities within each country. In Israel, all research projects require IRB approval, with or without a waiver of informed consent. Informed consent for research of any kind involving human biological samples, is required for all specimens collected after the enactment of the Law of Genetic Information, 2000. 7 The essential elements, models of, and ethical issues surrounding informed consent have been discussed extensively elsewhere.8–10 Consent must be voluntary, and participants must be informed of the nature and purpose of their participation, of risks and benefits, of their right to withdraw, and of their right or lack thereof to commercial patents derived from research using their samples. All of these elements exist to varying degrees in all of Israel's standardized consent forms for various types of research, and are particularly important when considering consent to future projects.
Israeli institutions do not engage in front door consent or consent to store samples and data as part of diagnostic or therapeutic procedures. Such consent, which exists in several hospitals around the world, would allow for the accumulation of vast biological specimen collections.
According to Israel's regulations regarding research on human subjects, all Israeli hospitals must use standardized informed consent forms provided by the Ministry of Health, with specific alterations as appropriate for the proposed project. Over the last 5 years, a standardized consent form for genetic research has been used for biobanking. This form, which is intended for specific studies, is not appropriate in the context of biobanking, since biobanking in and of itself does not constitute genetic research, and although the potential exists, not all research performed on banked specimens and data is genetic research. As such, over the course of 3 months (June–September 2012), biobank managers and members of the national ethics committee for human subjects research created a consent form specific for biobanking. Due to lack of resources, this form, as well as those for pediatric patients, and patients with nonmalignant disease (control patients), were drawn up on a voluntary basis in accordance with Israel's law of genetic information 7 and Israeli regulations for research involving human subjects. The form and explanatory leaflet, which together comprise five typed pages, have been approved by the Ministry of Health.
In keeping with ethical standards in Western countries, such as the requirement by the National Bioethics Advisory Committee in the United States, that research consent be multi-layered, 11 and with published literature concerning public opinion and the use of genetic material and data, 12 the form includes tiers of consent regarding the types of experiments the donor consents to, and an opt-in clause for return of genetic results; in contrast to the standard form for genetic research, it does not presently include the option of returning to the donor for re-consent.
Since biobanking in Israel is currently grouped with genetic research for informed consent purposes, specimens must be stored in an identified manner. However, samples are reversibly de-identified when provided to investigators performing ethics review committee-approved studies for which they may receive a waiver for further informed consent, depending on the nature of the study and IRB approval.
Currently, donors may be consented by a biobank's principal investigator, or by a co-investigator. Such an individual could be a coordinator working as a biobank employee. All consenters must have completed a good clinical practice (GCP) course.
In Israel, informing the donor has additional hurdles of multiple languages and religious considerations. Israel's most widely spoken languages include Hebrew, Arabic, Russian, English, and Amharic. Consent forms should be available in all languages, and verbal explanations must be provided in the donor's mother tongue. While written forms may be simple to translate, verbal explanation in the donor's mother tongue by a bank-affiliated physician or investigator may be difficult to provide. Indeed, funding of translation services is an additional challenge to consider in a multi-lingual society. In addition to language, religion plays a major role in some Israeli denominations. For example, when approached for consent, some religious Jews express the wish to consult with their rabbi prior to making a decision.
Since funding for the network is aimed at enhancing cancer research in Israel, donors will primarily be cancer patients of all types. Currently in the separate institutional banks, several types of cancers, mainly from adults, are banked. In addition, since there is now a consent form for control donors, patients undergoing procedures for nontumorous conditions, such as resections for inflammatory bowel disease, reduction mammoplasty, and bariatric surgery, may also be consented. In addition, a biobanking consent form for parents of children has also been designed and approved.
The meandering trail to form a national network for biobanking in Israel is similar to that of the trails followed in other small countries, the best example of which is that of the Biobank Ireland Trust (BIT), with its similar timeline. 13 While many similarities exist—extensive government lobbying, formation of a four-hospital network, design of a standardized patient information sheet and informed consent form—a number of major differences are apparent. First, BIT was established as a public charity, with early collaboration between academia and industry to promote public health. Second, BIT's interaction with patient advocacy groups has clearly been helpful. Third, it is clear that the result of these ethical and social experiences and interactions have accelerated the development of the network and enhanced its ability to function and increase its funding sources. In Israel, we are still at the stage of debating return of results and an acceptable sample access policy, whereas it appears that in Ireland these debates have largely been resolved.
Enhancing Cooperation Among Medical Institutions and Approaching the Public
Since we embarked on the challenge of building Israel's first biorepository network, several medical centers have expressed an interest in biobanking. We have met with individuals in at least three other hospitals, and provided documents of all types to assist and encourage the establishment of a centralized biorepository throughout Israel. In November 2010, Hadassah-Hebrew University Medical Center hosted the Marble Arch Working Group's semi-annual meeting, and in 2011, Sheba Medical Center hosted the first national meeting on biobanking, designed to raise awareness among medical professionals and researchers in the country.
One particular challenge has been encouraging parallel groups from different hospitals (e.g., information technology staff ) to work with each other. This is one of the reasons that so much effort has been made to enlist government intervention. A carefully constructed and funded national infrastructure that includes all hospitals in the network will obviate the need to provide incentives other than altruism for those not directly involved in patient care. For those involved in patient care, such as surgeons who participate in obtaining informed consent and directly provide specimens for research, some motivation to assist in specimen collection is certainly derived from altruism. However, in designing the policy that will guide the daily activities of the national biorepository, we have found that some stakeholders in each center (e.g., surgeons) wish for a modicum of access control. A clause stipulating that a certain percentage (35%) of samples will be made available to in-house investigators, following IRB approval, for little to no processing fee, has been included in the policy. Reaching an appropriate middle-ground to balance the interests of various stakeholders is one of the great challenges of biobanking, 14 and despite our best efforts, we accept the possibility that not all stakeholders will be completely satisfied.
One of the exciting spin-offs of institutional biobanking—and we hope to see it expand with the advent of the network—has been more collaboration, and more communication between investigators and clinicians involved in research projects. Since all projects currently require an IRB submission to one of the participating hospitals, through a physician, this creates a situation in which an outside researcher must approach a physician, usually an actively collecting surgeon, for collaboration. While scientists have traditionally expressed the view that surgeons excise tissue as part of their profession, and therefore should not receive credit as collaborators for such work, this attitude is changing. As the value of biological specimens is being increasingly understood, and as collectors are demanding due recognition for their contribution to science, the surgeons are becoming more actively involved in research, from the ethics application, which outside scientists cannot submit on their own, to true scientific collaboration using the collected biospecimens. We are pleased to enhance the connection and communication between investigators of all types, as this is one of the goals of biobanking which we expect will eventually lead to improved patient care.
Summary and Conclusions
Israel is a small, multicultural, and multilingual country, with a deeply ingrained tradition of academic achievement and competition. Networked biobanking is a complicated, laborious activity that emphasizes altruism and collaboration. In the last few years, Israel has made great strides in establishing centralized biorepositories in its larger academic institutions, as well as in its attempts to unify and harmonize its activities into a single network. Israel's biorepository network initiative still faces a long road ahead. We hope that our experience will shed light on some of the challenges in creating a biorepository network in our region.
At all times, hospital-based biobanking must be publicly promoted as an important, collaborative effort, providing a service to the community, and as such, it requires support from all stakeholders.
Acknowledgments
Sheba Medical Center Biorepository has received support from the Flight Attendants Medical Research Institute (FAMRI).
Author Disclosure Statement
No competing financial interests exist.