
Abstract
Cohort studies and biobank projects have led to public discussions in several European countries in the past. In Germany, many medium-sized studies are currently running successfully in terms of respondent rates. However, EU-wide research on general public perceptions of biobanks and cohort studies have shown that Germany is among those countries where people express the highest reluctance for providing body material and other data for research purposes. Because of early efforts of the just-initiated German National Cohort Study, we are able to begin to investigate in greater detail how various groups of people across Germany reflect and discuss the ongoing implementation of cohort studies and biobanking in Germany. Our research is based on 15 focus group discussions in four German regions, as well as on Eurobarometer poll data on biobanking.
Introduction
A
The GNC is a national interdisciplinary endeavor of scientists from the Helmholtz Association, the Leibniz Association, the Robert Koch Institute, universities, and other research institutes. In 18 study centers across Germany, a representative sample of the general population will be drawn for the GNC and will include a total of 200,000 participants aged 20–69 years. Baseline assessments include extensive questionnaire data, a series of medical examinations, and the collection of blood, urine, and other biomaterials. For about 40,000 participants, an intense assessment program is foreseen, and in 30,000 of these, extensive magnetic resonance imaging will be performed of the whole body, heart, and brain. After 4–5 years, all GNC participants will be invited for a follow-up examination. In addition, information about chronic disease endpoints will be collected through a combination of active follow-up and record linkages. The planned duration for the GNC is 25–30 years. The GNC will provide a major, central resource for future population-based epidemiology in Germany, and its results will help identify new and tailored strategies for prevention, prediction, and early detection of major diseases.
Medium-sized cohort studies such as CARLA (Cardiovascular Disease, Living and Ageing in Halle), EPIC (European Prospective Investigation into Cancer and Nutrition in Heidelberg und Potsdam), KORA (Kooperative Gesundheitsforschung in der Region Augsburg), RECALL (Risk Factors, Evaluation of Coronary Calcification, and Lifestyle in Essen), and SHIP (Study of Health In Pomerania in Greifswald) currently exist in Germany.8–12 All of these studies have high participation rates in comparison to other biobank-related cohort studies such as for example UK Biobank. 13
For more than a century, tissue and blood-derived biosamples have been stored for research purposes around the world without triggering much political, scientific, or public attention. 14 However, within the last decades, biobanks became increasingly framed as challenging.15,16 So far, biobank projects in a number of countries have led to broad public discussions; there is however no reported resistance in regard to German research endeavors.17,18
In this article, we will investigate how different groups of people in Germany reason about cohort studies and biobanking during a time when the largest German cohort study has been initiated. Numerous studies point at the fact that Germans display a comparatively critical attitude towards a variety of applications of biotechnology.19,20 We will show that this picture is not that clear when it comes to the planned German national cohort.
Between 2010 and 2013, we conducted a comprehensive qualitative study to investigate what various German people think about cohort studies and biobanks, and which preferences they express. Groups of people were introduced to the topics of biobanking and cohort studies and were given space to debate and express their points of view. Our data are supplemented by related Eurobarometer survey data. The goal of this investigation is to explore public perceptions of cohort studies in Germany as part of the preparatory phase of the GNC and to supplement this investigation with further prospective research.
Materials and Methods
The overall aim of this study was to develop an understanding of how groups of people in Germany discuss and reflect on population-based cohort studies and biobanking activities. A total of 15 focus groups were conducted across Germany, taking into consideration regional specifics in Augsburg, Berlin, Essen, and Kiel. Focus group discussions are a qualitative method of data collection, drawing on group interaction, in addition to individual statements on specific topics introduced by a moderator.21,22
Participants were selected purposively, recruited via telephone and snowball sampling, approximating the characteristics of the anticipated population of the GNC. One set of groups was therefore sampled for different people who live in Germany with various socio-demographic backgrounds. Following this approach, we did not assume a single German ‘public’ consisted of the total sum of all people within this socio-political space, but rather aimed to explore typical public opinions and patterns of meaning stressed by selective groups of people. This accounts for given social relations of power within societies.23,24 Another set of focus groups consisted of people who had already donated blood or tissue or who had previously participated in a cohort study. These groups were recruited via the study centres of the GNC. Additionally, two groups were sampled for people with migration backgrounds, to deepen our knowledge about this societal group.
Each group meeting lasted for about 2 hours. They were led by two moderators and consisted of between 9 and 12 people, totalling 151 participants: 73 men and 78 women between the ages of 18 and 80 with varying socio-cultural backgrounds. Table 1 provides an overview of the conducted focus groups.
Assuming that most people have limited knowledge about cohort studies and biobanks, we therefore introduced participants gradually to the topic and let them voice the issues they identified and their perceptions based on their own experiences and life-worlds.
All groups were conducted by two experienced moderators who led the group with only enough involvement to keep them on track. However, all groups followed a script developed at the beginning of the project, rendering the resulting qualitative data comparable and rigorous. Five central themes were deductively selected due to their relevance in related expert discourse on the governance of cohort studies and biobanks:
1. Knowledge on cohort studies and biobanks: Discussants were asked about five items that displayed the extent to which people are familiar with this topic. The items addressed data collection, exploration of genetics and lifestyle, as well as long-term research. The assignment also provided the participants with general information on cohort studies and biobanks. 2. Advantages and disadvantages: Participants were asked what kind of advantages and disadvantages they expect, and under which conditions they could imagine participating in cohort studies. 3. Problems and special issues in the ethics of cohort studies and biobanks: In these sections, we discussed well-known ethical issues in the field of biobanking, such as informed consent (broad and narrow consent, withdrawing, etc.), privacy (data linkage, protection, and confidentiality), compensation (financial compensation, obtaining results, and the common good), and commercialization (benefit sharing, actors involved, and medication). 4. Cohort studies and biobanks in international and transnational contexts: Perceptions of international and transnational exchange and cooperation between cohort studies and biobanks were addressed. 5. Governance and regulation: Participants were asked which issues they find important for governance to deal with and about who should be responsible for regulating cohort studies and related data storage.
In addition to this structure of topics and questions, all groups were designed to give enough freedom to all participants to introduce new issues and to explain their own narratives. This yielded the possibility for new insights and debates. Carey and Smith 25 argue that the biggest advantage of focus group discussions is the opportunity to capture rich and detailed information, which implies that, during intense discussions, issues may arise that might otherwise have been withheld in a structured, two-person conversation.
The focus group discussion data were recorded, transcribed, and then analyzed with support of qualitative data analysis software. Data collection, interpretation, and reflexion overlapped and proceeded randomly. 26 Analysis began when the first data were available.
For reasons of comparability and because of the large data set, a structured content analysis was initially applied for analyzing the transcribed data. 27 The structure of the focus group script provided the frame for the categories, whereas the related codes were created inductively. Each code was amended with a description and built based on predefined levels of abstraction. This strategy was set to increase the reliability of the coding structure. All codes were furthermore scaled as either positive-, negative-, or as conditional issue. The code structure was created from the first data and then continuously adapted with all involved researchers.
In the next step, a comparable and in-depth interpretive analysis was performed with selective data pieces, aiming for revealing hermeneutic structures and discourse and to deepen our knowledge and interpretations beyond the manifest content.26,28
Additionally, in the 2010 Eurobarometer data on biotechnology, 19 six questions on biobanking were posed. Those questions were created in close cooperation with this research project. In the next section, we introduce some quantitative findings from different Eurobarometer surveys to provide a broader overview, illustrate the most central insights from the focus group discussions in more detail in following sections, and discuss our findings in the context of the planned GNC.
The broader picture: Quantitative data
Compared to other European countries, Germany is characterized by moderate to low awareness of cohort studies and biobanks, moderate to low potential participation, and a comparatively high demand for specific consent, as demonstrated in Figure 1 from the 2010 Eurobarometer on Biotechnology. 19
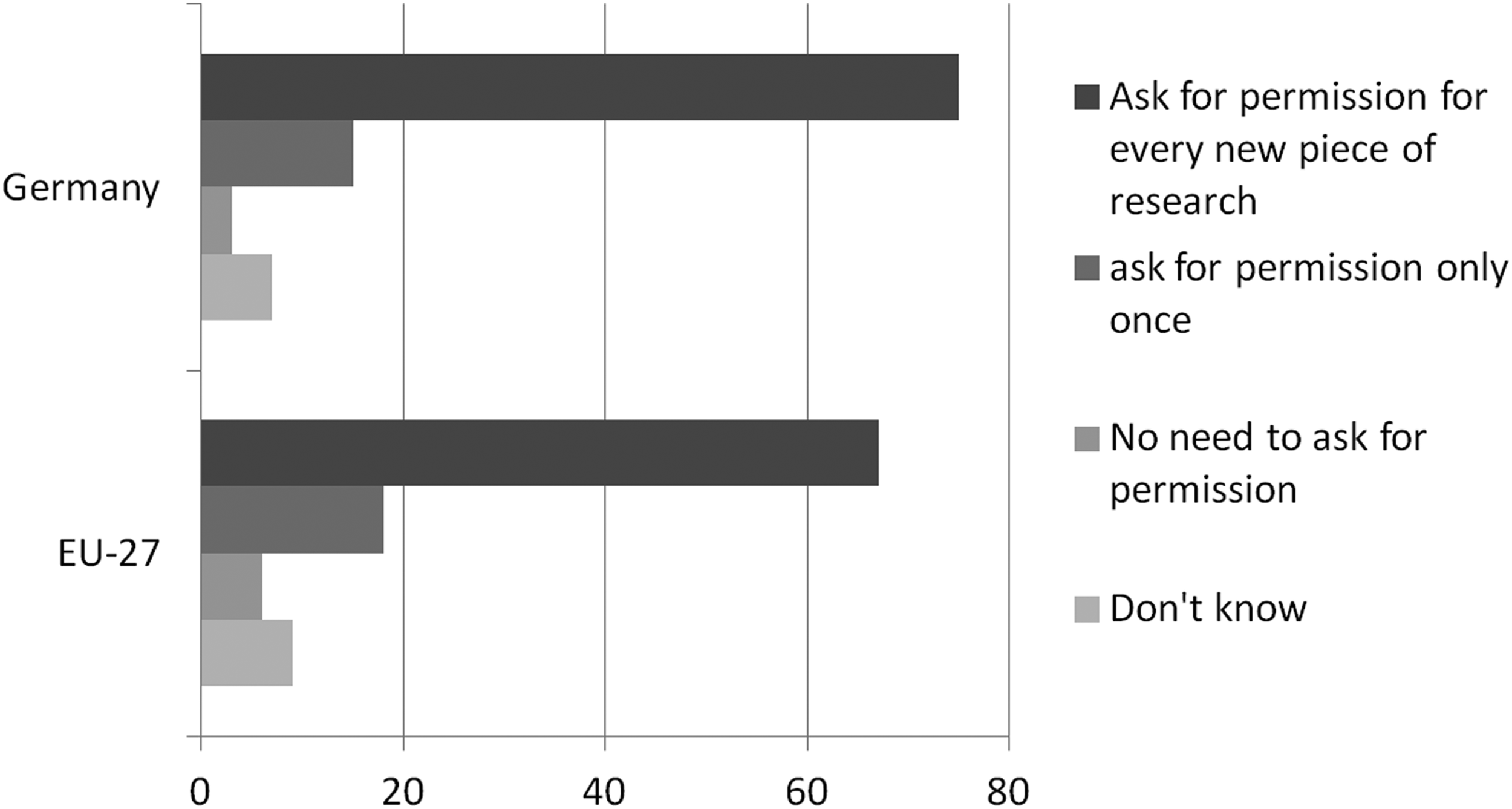
Preferred form of consent in Germany and EU-27, in percentages.
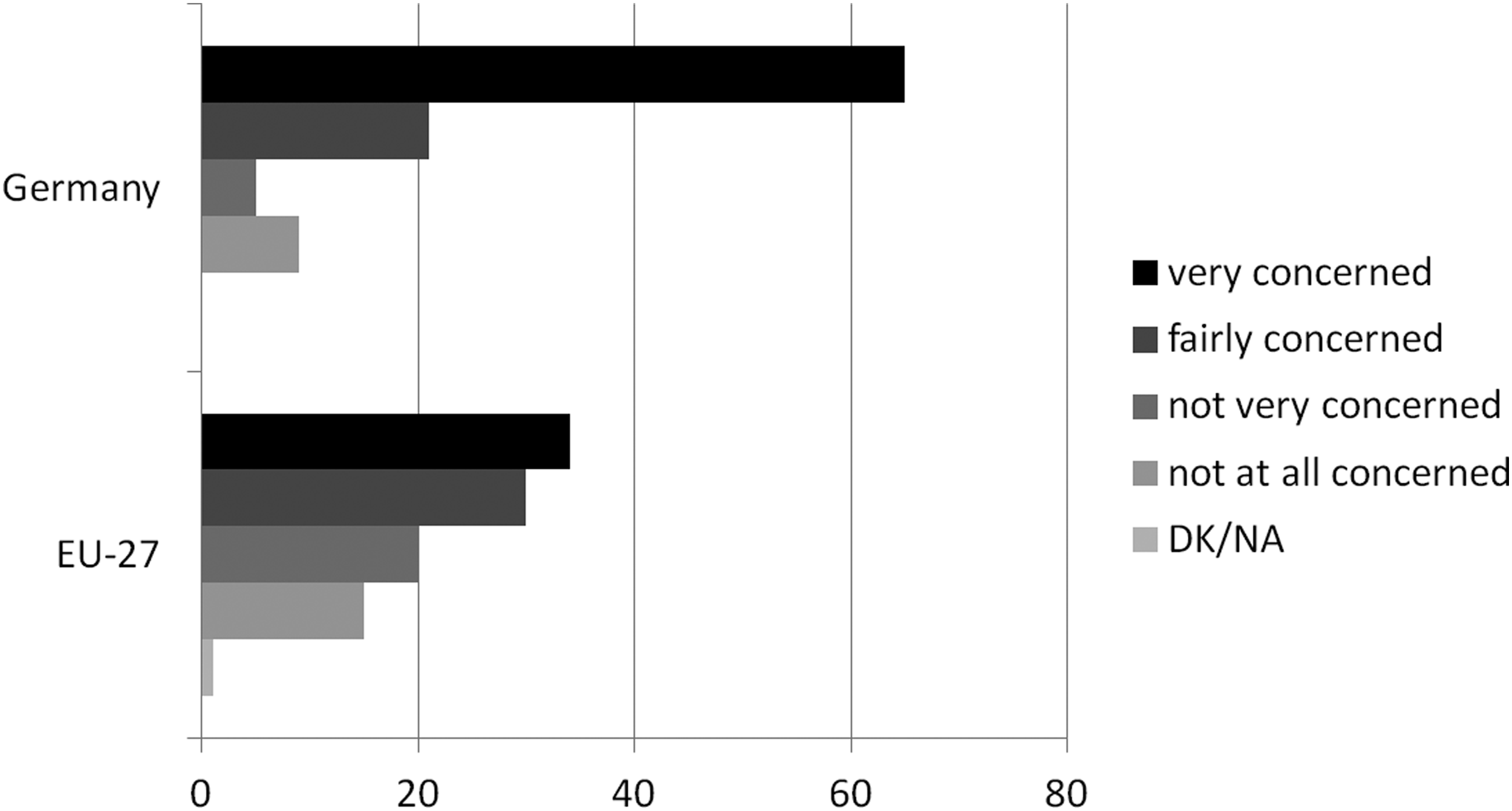
Most noticeable are Germans' very high concerns about providing different kinds of information for research purposes. For both biological and social data, German people expressed the most concerns across Europe; 19 ; see Figure 2.

Concerns about supplying different types of biomaterials and data in Germany and EU-27, in percentages.
Another Eurobarometer on general data security issues from 2008 shows high levels of concerns about personal data fraud of German publics compared to other European countries. 29 People were asked about their level of concerns regarding private and public organizations holding personal data. The percentage of those in Germany who claim to be very concerned is far higher than in any other EU-27 country, with the exception of Austria; see Figure 3.
Concerns about data privacy about the various private and public organizations that store personal data, in percentages.
A Eurobarometer Survey on Science and Technology from 2010 supports the trend described above. 30 Compared to other European countries, Germans show higher concerns about the possible impacts of scientific developments. They clearly opt for a straightforward framework that sets boundaries about what science should investigate and what it should not. Only 21% of all polled Germans agree that “science should have no limits to what it is able to investigate?”; see Figure 4.
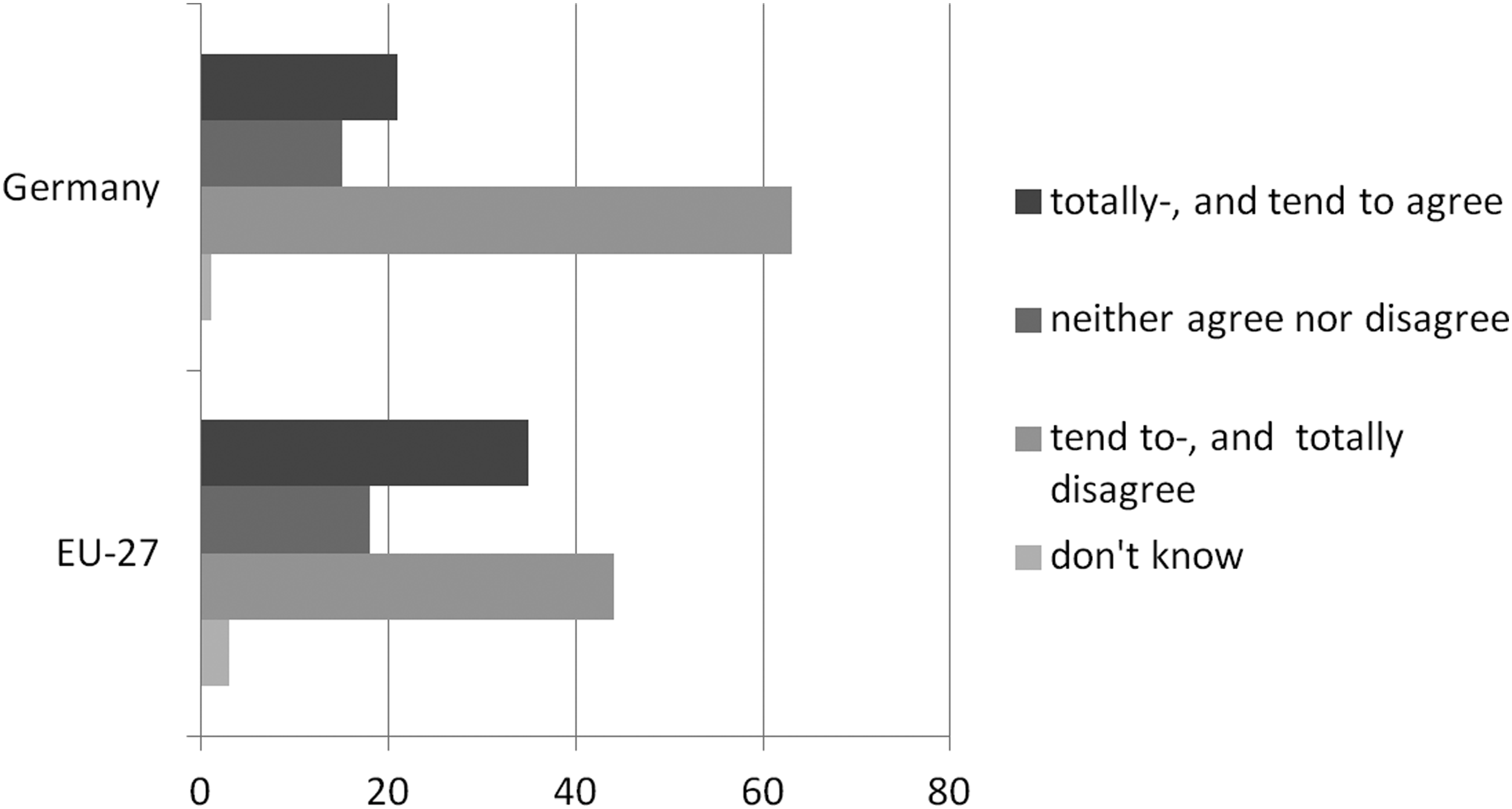
Agreement and disagreement on limits for scientific investigations, in percentages.
Germans are particularly sceptical about commercial interests in medical contexts. The 2010 Eurobarometer data on science and technology show that Germany is the second-most reluctant country when it comes to third-party funding. 30 72% of all Germans agreed that “we can no longer trust scientists to tell the truth about controversial scientific and technological issues because they depend more and more on money from industry,” compared with only 68% in the EU-27 average; see Figure 5.

Agreement and disagreement on mistrust in scientists on account of commercial impacts, in percentages.
However, many people in Germany are positively confident about scientific research and new technologies in general, and well aware of the possible benefits. Figure 6 indicates that 85% of the representatively polled German participants agree that “a scientific discovery is in itself neither ‘good’ nor ‘bad,’ it is only the way the discovery is used that matters.” 30
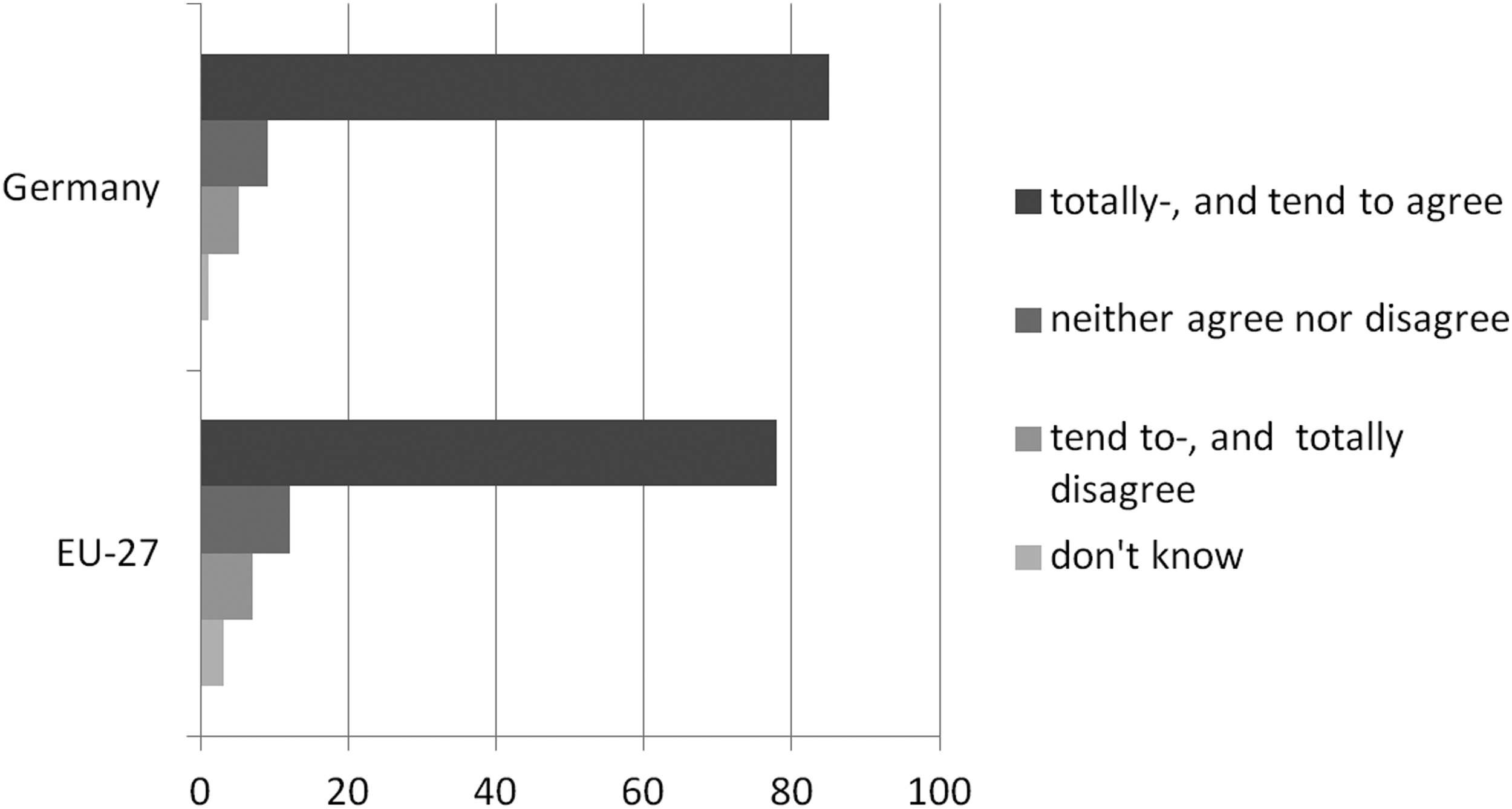
Agreement and disagreement that the usage of scientific discoveries prevails over general valuations of being good or bad, in percentages.
The following sections provide insight into the central issues discussed during the focus groups. The interplay of the above described expressed reluctance and support for biomedical research by German people is explored in greater detail.
Where discussions start
The following data show how discussants' perceptions of cohort studies are strongly affected by their expectations and hopes about medical benefits, as well as by former experiences with data transfers and frauds. That participants referred randomly to more general, familiar topics makes sense, as most of them expressed moderate to low knowledge about cohort studies and biobanks. Many of the participants wondered aloud why they have never heard of these research endeavours, and they expressed their desire for transparency. They wanted to know about responsibilities, involved actors, goals, and financial interests.
FG10, P5: “My first thought was that I was a bit scared, that I don't know much about it, cohort studies. I did not know the name, but, well, now I know something about it (…). Biobanks, there I know almost nothing about it, and this I find somehow suspicious.”
The discussions with groups of people from Germany have shown particular preferences for cohort studies and biobanks. Those discussants who have already participated in medical research before have valued cohort studies based on experiences they had with the research and typically expressed fewer ethical concerns. Another notable finding was the comparably positive view on cohort biobank studies in the discussions in the region around Essen in the Ruhr Area, where pollution and environmental issues have been present in the past. People from this region were not only more willing to participate, but also less inclined to name personal disadvantages for long-term studies. However, these groups were also wary about discrimination based on regional issues. In the two groups with people with immigration background, we found comparable high expectations for medical research and health implications, but also increased rejection of cohort studies due to doubts about their validity based on preferences for traditional medicine.
Overall, positive associations that participants had with cohort studies were mentioned slightly less often than negative ones, which reflects also in the quantity of coded data pieces scaled as negative (537) in comparison to those framed as positive (406). The focus groups suggest that most people have a clearer picture of the possible benefits of this sort of research. Gaining knowledge, contributing to science, and finding solutions for diseases are common aspects that were randomly addressed.
Once introduced to the topic of cohort studies and biobanks, people typically expressed support for medical research and referred to notions of ‘the common good’ and ‘collective demands.’ These arguments often imply an idea of benefits for humanity or for Germany as a state. The participants connected science and medicine with the idea that benefits will likely affect a broad range of people. Expectations for various health benefits were repeatedly framed as privileged over concerns, such as the following statement demonstrates:
FG4, P3: “…because if one is affected, then you don't give a damn if a database gets linked (…). Then you are happy if the researchers say ‘yes, we have something, your child gets rescued.’ One always has to consider it from this side, too.”
However, a number of people also expressed hopes for personal benefits, such as a follow-up that would provide personal results, or other forms of compensation. More on that later.
Discussants did however also name difficulties of which they were aware. Most prevalent were questions about data usage and the distribution of benefits. Once people were personally asked to list their hypothetical reasons for and against participating in this kind of research, privacy issues became less dominant and questions about the entities who actually conduct research were addressed more frequently. Participants thereby expressed the desire to know about responsibilities, actors involved, and how this research is financed.
FG14, P9: “I mean, who has access? Who has real access on what happens with these data? And if it is a public issue, for me it is something different, as if it is some company.”
Fears about data abuse were present, but impacts were also argued along the lines of practical issues, such as personal time commitment.The most debated topics during the group discussions were data usage and the distribution of benefits; discussants' reflections on these are explored in greater detail in the following sections.
Data provision and informed consent
While most discussants express general support for medical research and its anticipated health benefits, many of them initially raised issues about providing data and about further use of those data. Focus group participants set out specific conditions they want to see observed in terms of data linking. Intensively discussed was a desire for regulation and control and the feeling that personal privacy should be protected. The consensus among participants was that, within biobank cohort studies, the data themselves have to be made anonymous or collected anonymously, and data access to third parties must be restricted as closely as possible.
FG2, P7: “Data must be coded, must be separated from genetic material, and must not be given to other non-authorized persons, for research or marked analysis purposes or whatever. This would be the main criteria. And another point: once this cohort is over, or once I opt out, I can trust that the data will be deleted.”
Many discussants stressed concerns about data being abused because they were confident that even the most sophisticated data protection system could be bypassed. They perceive that data linking might lead to personal disadvantages. A randomly mentioned fear among most people is third-party access to their data, particularly by insurance companies or employers.
FG5, P6: “How is security guaranteed? That no employer has the idea afterwards to say, based on research findings, ‘no, I do not want to employ such people.’ These are things I have experienced myself.”
Discussions about data streams were in many cases complemented with general examples of data frauds with which people are familiar. The recent discussion about an illegally procured data medium with banking details that was purchased by the German government was mentioned during the discussions. In speaking about data protection, people also referred to surveillance practices established by the State Security Service (Staatssicherheit or Stasi) in the DDR between 1950 and 1989. Talking about these examples, people typically concluded that data protection and its regulation in cohort studies may always be subject to uncertainty. Germans therefore seem sensitive to surveillance and violations of informational privacy, and we can observe an absence of trust in the ability and intention of stakeholders to protect and guarantee informational privacy:
FG5, P6: “Just think about what secret material has been forwarded by a single secretary during the Cold War period.”
These concerns about privacy are strongly consistent with assumptions about future societal developments and a general loss of control. People named the possible exclusion of persons or groups of persons from health care benefits legitimized by genetic risk profiles.
Perhaps paradoxically, concerns about data provision do not necessarily prevent discussants from approving hypothetical participation in cohort studies. Many of the people said they were nowadays constantly faced with data streams and privacy issues in their personal and professional lives. They often couched even their positive or supportive statements about biobanks in terms of resignation regarding data protection. As described above, people accept the “fact” that they cannot avoid dealing with these kinds of issues nowadays. There are various ways of acting when people show limited trust in data protection. Some people believe that there are plenty of data already “out there,” that everyone has lots of data “out there,” and that no one is interested in their specific data. New Web 2.0. developments such as Google Street View and social networks were specifically named in this context. We can distinguish between personal resignation, which implies the perception that the chance of being affected by privacy violations is low, and societal resignation, whereby people are confident that they are at constant risk anyway regardless of whether they participate in research and regardless of any protective measures taken. While the first type constitutes in typical examples such as, “I am not important,” “I have nothing to hide,” or “these data are unproblematic,” the latter refers to narratives such as “everyone is doing it,” “data are already everywhere,” or “that's how the world is.” It is in either case the possible common or individual benefits that people set at stake, rather than associated risks.
Once these risks associated with data provision are either perceived as low or as inescapable, possible benefits come to the fore. People then talk about personalized medicine or new treatments for diseases. Possible personal or societal benefits are even named as swaying factors for accepting a certain amount of risk.
FG4, P6: “If one finds out via a cohort study, or via my samples that I have given, that I have a specific risk, for which it might be advantageous if someone informs me about it. So, if I say I want it all [to remain] anonymous, this also means I cannot be informed. But maybe I want to be informed, once for specific questions, [if ] the likelihood is high that a certain disease appears with me or in my family.”
Once participants were asked about informed consent, groups were torn about the preference for either broader or narrow forms of consent. Those who chose broader consent mainly referred to research benefits often framed in altruistic narratives on contributing for science. Focus group participants with prior experience with medical research debated comparably more supportive on broad forms of consent. On the other side, narrow consent was mainly preferred due to fear of data frauds and the unpredictability of long-term research. They anticipate that providing broad consent might subject them to unethical practices such as cloning, commercialization, or extensive medication that participants do not agree with.
Distribution of benefits
The issue of benefit sharing—receiving something in return for participating in a biobank—emerged as an topic that was debated randomly along different aspects of cohort studies and biobanking, such as when discussing informed consent or impacts of data streams. Feedback about findings from personal check-ups was widely demanded by the vast majority. Still, there was a conflict between the desire to be informed about personal results and the desire for complete anonymity. Fears about negative results were, however, uncommon across the groups. Many people assumed that as a consequence of their participation they would receive insight into their health status, and they looked forward to the possibility of regular health checks with the opportunity of meetings with medical experts.
FG8, P7: “The uncomplicated contact with specialists. […]. They might give me knowledge that my family doctor does not have, because they are actually doing this research, and I think this could be a great incentive, to take part in such study […] and have the possibility for special audiences or the opportunity to talk with a professor who usually does not have any private patients.”
Receiving general research information did not trigger negative associations in any of the focus groups, but participants were generally less enthusiastic about this kind of follow-up. Still, some discussants valued this kind of feedback for one or more of the following three reasons. First, they saw it as a fair gesture; second, some people were interested in results; and, third, it provided insight in what has been achieved with one's data. The third option (insight) is the most often named reason for desiring general information. However, many people voiced their fears that they would have difficulty understanding or have limited time resources to deal with this sort of information, which led some to suggest that it should be provided in an easy and understandable manner:
FG8, P7: “I think everyone who participates in such a study should have the right to know the findings.”
The question of whether financial benefit should be granted was dominant among the discussions about compensation. Financial compensation in terms of payment was mostly rejected, although some participants supported financial compensation for having no additional costs and/or a small allowance for the commitment. Financial compensation was therefore also perceived as a gesture of respect and appreciation. Debating financial compensation, people often spoke in the third person, likely to distance them from appearing greedy. The focus group participants were divided about whether it should be compensation of allowances, payment, or no money at all. All narratives were found repeatedly among the groups. Rejecting the principle of financial payback, was mainly justified by the expectation that research will benefit the public, anyway. Moreover, this group of people also typically feared that research would likely be steered by financial interests and people might be forced to participate for financial reasons (as with students participating in clinical trials). In this context, blood donation was repeatedly mentioned as an example, with participants drawing on notions of ‘the common good.’
Discussions on compensation typically led to questions about the entities that conduct research, and its anticipated aims. If a private institution would ask for time-consuming or even risky check-ups, people said to be seeking financial compensation more often. The discussants were overall critical when it came to private, commercial involvement in cohort studies and medical research. However, while first reactions were mainly negative, people often developed more moderate stands during the discussions and related to the necessity of private partners and possible benefits from this cooperation. Particularly in the field of drug development, positive associations with private involvement due to research progress were typical. Nevertheless, research conducted by well established public research institutes was randomly named as most preferable option.
Discussion
Future research in epidemiology is dependent on public support and the successful recruitment of volunteers across Germany, including achieving respondent rates that meet scientific standards. Knowing where societal sensitivities are democratizes science and provides the opportunity to regard the expressed demands of German citizens.
Despite individual and regional variations, three key findings emerged from the focus groups regarding participants' thoughts on medical and epidemiological research. There seems to be (1) general support for cohort studies and biobanking in the field of bio-medicine, mainly based on expectations for individual and communal research benefits. (2) Concerns about data streams and fraud most likely lead to rejection of research. (3) Those entities who conduct research have significant impact on people's expectations about benefits and data streams, as well as about their general willingness for and against providing data.
1. Both quantitative and qualitative data presented reveal some general support for cohort studies and biobanking. Focus group participants perceived medical research as important and expected general and personal benefits. The research activities of cohort studies are mostly welcome in principle, and the improvements of diagnostics as well as a more individualized medicine were promising outlooks for most discussants. In many cases, research was associated with common benefits for society, which relates to broader ethical discussions about communal framings of risks and benefits in biobanking. 31
Nevertheless, apart from communal advances, benefits on a personal level were addressed randomly during the discussions. The expressed preference is interesting, as Germans indeed perceive their public health care system quite positively, rating it as a six on a scale of ten, which more or less reflects the EU-27 average for this investigation. 32 But, compared to other nations in EU-27, Germans reported slightly more often a negative health status, and showed unmet medical needs. That was mostly the case because respondents had not consulted a medical expert, instead taking a “wait-and-see” attitude toward their health. 33 A majority of the focus group participants stated that they do not consult doctors regularly and that a cohort study might be a good way to receive regular check-ups. This implies that, after supplying biosamples in a cohort study, most people expect some sort of personal follow-up on their own health status, as well. This follow-up can consist of random check-ups or even specific tests such as computer tomography or magnetic resonance imaging. The desire for personal benefits may also be explained by the gap between people with public and private health insurance in Germany that was regularly mentioned during the focus group discussions. This situation was accompanied by the desire for medical experts who take the time to speak to their patients about health issues.
It is most interesting in the context of a country as wealthy as Germany that benefit sharing is such an important issue: Future studies therefore must find an appropriate model for “giving back” to participants, in particular in the form of health information. That this is successfully possible has been shown by the high response rates in ongoing German cohort studies, such as KORA, which had a high initial response as well as a high follow-up response rate. Indeed, in these studies, “giving back” of detailed health information and contact to their physician in the case of relevant findings play a major role. Building mainly on altruistic patterns for benefits has resulted in comparably low respondent rates in the case of the UK Biobank. 13
2. The provision of data is a topic where discussants were particularly sensitive. This began with a general desire for narrow consent, concerns about the provision of data and about public and private organizations that hold data, as described above. The focus group discussions revealed some further insights about how data frauds from other areas of life, as well as the long-term nature of cohort studies and biobanks enhance concerns. While the first aspect mainly refers to anticipated frauds by insurance companies and employers, the latter addresses the discrimination of individuals or certain groups on the basis of data originally collected for medical purposes. Long-term impacts are typically expected with genetic data and associated new forms of re-dividing groups of people based on genetic profiles.
However, most discussants were certain that each security system can be bypassed. Due to recent privacy violations and massive data streams in different areas of life, people were in many cases already accustomed to providing data and living with a certain amount of uncertainty. Participants then typically employ expressions of resignation in their narratives, in which people estimate the impact of data fraud on themselves to be limited and general developments within the society as dominant. In these cases, the risk of being affected by data fraud is either perceived as very low or as inescapable, but in both cases the fraud potential led participants to focus on benefits or burdens associated with participation rather than privacy issues.
If the risk of participation in cohort studies is framed as low, discussants either perceived their own person as not important, assuming that no one will be interested in tracking them, or they take the position that they have nothing to hide and that only wrongdoers might have a problem with giving away their data.
Once risks are framed as inescapable, participants expressed that data about them are already “out there” and that giving away another piece will not make any difference. They give away great amounts of information randomly in their lives, which currently happens most prominently in the context of social networks. This somehow leads to a situation in which the perception arises that further data pieces will not make a great difference. This point of view can be compared to the anonymity people perceive as theirs in the public spaces of large cities, even where digital surveillance might be constant.
This widespread attitude about privacy issues does not mean that people do not care about restricting their data in a biobank context. In fact, with long-term biobank projects, they do expect the best possible protection and the best research institutes to handle their data with care. Concerns about data misuse may easily lead to a rejection of cohort studies, but it may also be accepted in favor of expected benefits. Though participants understood that breaches might still occur, this possibility did not keep them from expressing the eventuality of participation in cohort studies. Data protection issues were identified as key for every cohort study, but this research suggests that privacy protection is mainly a basic prerequisite, and further support may be acquired if outcomes and benefits are expected.
3. The balancing of data fraud and health benefits was randomly related to questions about the institutions that actually operate the research projects and storage infrastructures. Research done by well-established institutions, such as the Helmholtz Association orthe Robert Koch Institute, were particularly framed as promising and trustworthy during the discussions, even by participants who expressed comparably critical attitudes across the group discussions. These research institutes were expected to be more likely to share benefits with the public and individual patients than are private research institutes from the pharmaceutical industry.
Quantitative data have shown that the involvement of industry in science is perceived critical in Germany. Focus group data have shown that communitarian logics are indeed important for the field of epidemiology and that private involvement is oftentimes seen as contrary. However, particularly for the field of drug development, the necessity for public–private partnerships was acknowledged.
It is still unclear if the further implementation of the just launched GNC will work comparably well as former cohort studies, or if the reported critical attitudes in Germany may lead to public rejection. Therefore, topics of concern have been identified and addressed in the first stage.
Data usage will be regulated by several mechanisms in the GNC that will be performed based on the German Data Protection Act/16/and other directives. 34 Moreover, the Opinion of the German Ethics Council/17/ on human biobanks for research as well as other ethically relevant directives has been adapted. The concept of the GNC for data protection has been developed in close collaboration with German federal and state data protection officers. An external ethics advisory board has been established that will work with the GNC over the full period of the study. A Code of Ethics of the GNC has been developed. In the future, the ethics advisory board will publish all protocols in the web, following the model of the UK Biobank Ethics and Governance Council (www.egcukbiobank.org.uk).
We have, however, shown that data protection is widely perceived as one important step, whereas further expectations have to be met for gaining public support. Germans seem optimistic about research in general and individual and communal health benefits may indeed be anticipated with cohort studies and biobanks. Former cohort studies in Germany, such as KORA, have already managed to communicate a balance of security and beneficial relationships rather than being lost in general ethical debates.
It is mostly not what cohort studies are, but what they might become or develop into, that triggers fears and anxiety. The next years will show if the GNC can follow up to former cohort studies in terms of acceptance and respondent rates. The well established research institutes involved provide a good basis for that.
Footnotes
Acknowledgments
Author Disclosure Statement
All authors declare no conflict of interest.
Appendix
Quotations in original German language:
FG10, P5: “Mein erster Gedanke war, also ich war so ein bisschen erschrocken, dass ich quasi nicht viel darüber weiß: Kohortenstudien. Der Name war mir nicht geläufig, aber gut jetzt weiß ich was darüber (⋯). Biobanken, da weiß ich so gut wie gar nichts und das fand ich dann fast ein bisschen verdächtig. Dann der zweite Gedanke: weil ich lese Zeitung, bin normal gebildet, warum habe ich davon so wenig gehört?”
FG4, P3: “⋯Denn wenn man selber betroffen ist, dann ist einem das gelinde gesagt Scheiß egal ob da eine Datenbank verknüpft wird (⋯). Da ist man froh, wenn die Forschung sagt ja, wir haben was, ihr Kind wird gerettet. Man muss das immer von der Seite auch sehen.”
FG14, P9: “Ich meine wer hat Zugriff. Wer hat denn wirklich den maßgebenden Zugriff was mit diesen Daten passiert. Und wenn das eine staatliche Sache ist, ist das für mich was anderes, als wenn das ein Konzern ist.”
FG2, P7: “Die Daten müssen verschlüsselt sein, müssen getrennt von Genmaterial vorliegen. Dürfen nicht an irgendwelche Dritte unbefugt weiter gegeben werden. Zu Forschungszwecken oder Marktanalyse oder was weiß ich. Das wären einfach so die Hauptkriterien. Das wär auch noch ein Punkt, wenn diese Kohorte beendet wird oder wenn ich aus der Kohorte austrete, dass ich dann darauf vertrauen kann, dass die Daten gelöscht werden.”
FG5, P6: “Wie ist da die Sicherheit gewährleistet, dass nachher nicht irgendein Arbeitgeber auf die Idee kommt, anhand dieser Forschungsergebnisse zu sagen, nein, solche Leute wollen wir nicht einstellen. Das sind dann Dinge, die ich selber persönlich erlebt habe”
FG5, P6: “Denken Sie nur mal was alles an Geheimmaterial in der Zeit des Kalten Krieges dann doch über eine einsame Sekretärin nach draußen gekommen ist.”
FG4, P6: “Stellt man im Lauf der Kohortenstudie fest - oder über meine Probe die ich abgegeben habe - dass ich ein bestimmtes Risiko habe, für das es vielleicht vorteilhaft wäre, wenn man mich darüber informiert. Also wenn ich sage, ich will es ganz anonym haben, dann heißt das aber auch, ich kann nicht informiert werden. Vielleicht möchte ich aber informiert werden, wenn bei bestimmten Fragestellungen, wenn die Wahrscheinlichkeit groß ist, dass eine bestimmte Krankheit auftritt, bei mir, oder in der Familie.”
FG8, P7: “Ich finde jeder der an so einer Studie teilnimmt sollte das Recht haben, auch die Ergebnisse zu erfahren. Ja was mir hier in diesem Land immer so auffällt, dass zwar jeder irgendetwas sammelt, aber was dann so zu sagen rauskommt erfährt man nur unter äußerster Kraftanstrengung und ich finde jeder sollte wirklich das Recht haben, mir irgend meinetwegen Gutschein auf ein Exemplar dieser Studie und dann darf keiner kommen, der sagt, du verstehst das sowieso nicht was da drinnen steht. Dann muss man eben die Studie so schreiben, dass eben auch Ottonormalverbraucher die versteht.”