
Abstract
Nottingham Health Science Biobank (NHSB) was established in 2011 by a 3-year “pump priming” grant from the United Kingdom National Institute of Health Research. Before biobanking operations began, NHSB commissioned a financial report on the full costs of biobanking and worked with key stakeholders and external consultants to develop a business plan with the aim of achieving financial and operational sustainability. The plan included: scanning published information, telephone interviews with commercial companies, Freedom of Information Requests, dialogue with prospective customers, and a market analysis of global trends in the use of human tissue samples in research.
Our financial report provided a comprehensive and structured costing template for biobanking and confirmed the absolute requirement to ensure cost-efficient processes, careful staff utilization, and maximization of sample turnover. Together with our external consultants, we developed a business model responsive to global interest in healthcare founded on i) identification of key therapeutic areas that mapped to the strengths of the NHSB; ii) a systematic approach to identifying companies operating in these therapy areas; iii) engagement with noncommercial stakeholders to agree strategically aligned sample collection with the aim of ensuring the value of our tissue resource.
By adopting this systematic approach to business modelling, the NHSB has achieved sustainability after less than 3 years of operation.
Introduction
T
The NHSB forms the center of a ‘hub and spoke’ model that synergizes existing facilities in the University of Nottingham and other linked research environments and includes the Breast Cancer Campaign Tissue Bank. We have Trust-wide ethical approval for generic and enduring donor consent. This approval allows the collection of any biomaterial taken in the course of routine care and which is excess to diagnostic requirements. Our activity is regulated under the UK Human Tissue Act (HTA) by license from the Human Tissue Authority. The information collected and released to researchers complies with NHS Caldicott requirements, the Data Protection Act 1998 and the European Convention for Human Rights (Human Rights Act 1998) Article 8.
The NHSB uses state-of-the-art systems for biomaterial storage and tracking, temperature monitoring, and sample processing, and has worked closely with commercial partners Achiever Medical to evolve a sophisticated, centralized, computer-based system of biosamples linked-data procurement and management. The NHSB collects a wide range of biomaterials including: fresh tissue, snap-frozen tissues, formalin-fixed, paraffin-embedded tissues (FFPEs), blood (serum and plasma), PBMC (1×106), packed red blood cells, and provides dedicated facilities for tissue processing, including the routine extraction of RNA, DNA, and the formation of tissue microarrays.
NHSB was established by a development grant of £1.6M provided by the UK National Institute of Health Research. No other income was assured and it was therefore anticipated that the Bank would need to be self-funded by April 2015. However, following rescheduling of a proportion of the development grant, the original proposal was revised and the ‘break-even’ point at which the NHSB would be required to be self-sustaining was brought forward to March 2014. It was therefore clear from the outset that the NHSB was confronted with a major survival challenge and required a robust business plan to maximize the likelihood of achieving sustainability within a short time scale.
Methods
Financial and business modeling
The first act of the NHSB, performed prior to any sample collection, was to commission a detailed financial report on the ‘real world’ costs of harvesting, storing, and releasing biosamples. The report used prevalent NHS staff, estates, and overhead rates to produce an itemized costing structure for all types of samples, derivatives, and clinical annotation. Costs were calculated primarily on the time taken for a given activity, and based on the minimum grade of post required to undertake the process. This financial forecast demonstrated that the actual costs associated with biobanking were significantly higher than recognized by most researchers and funding bodies—for example, in aggregate an average sample could cost 5–10 times more than estimated by the UK Medical Research Council. The financial plan then used a variety of methods, included scanning published information, telephone interviews with commercial companies, Freedom of Information Requests, and dialogue with potential customers to establish the market value of biosamples and linked clinical data. This exercise both established that research grants, using current costing schemes in the UK, could not sustain the biobank and that, while supporting academic research was the primary purpose of the NHSB, cost recovery from commercial organizations would be needed.
NHSB therefore engaged external consultants to assist in setting our plan in the context of market needs and trends for the use of human tissue samples in research. Together with our external consultants, we developed a business model responsive to global interest in healthcare founded on: i) identification of key therapeutic areas that mapped to the strengths of the NHSB; ii) a systematic approach to identifying companies operating in these therapy areas; iii) engagement with noncommercial stakeholders to agree on strategically aligned sample collection with the aim of maximizing the value of our tissue resource, together with iv) consistently high quality of biosamples; v) rapid response time; and v) cost effective process.
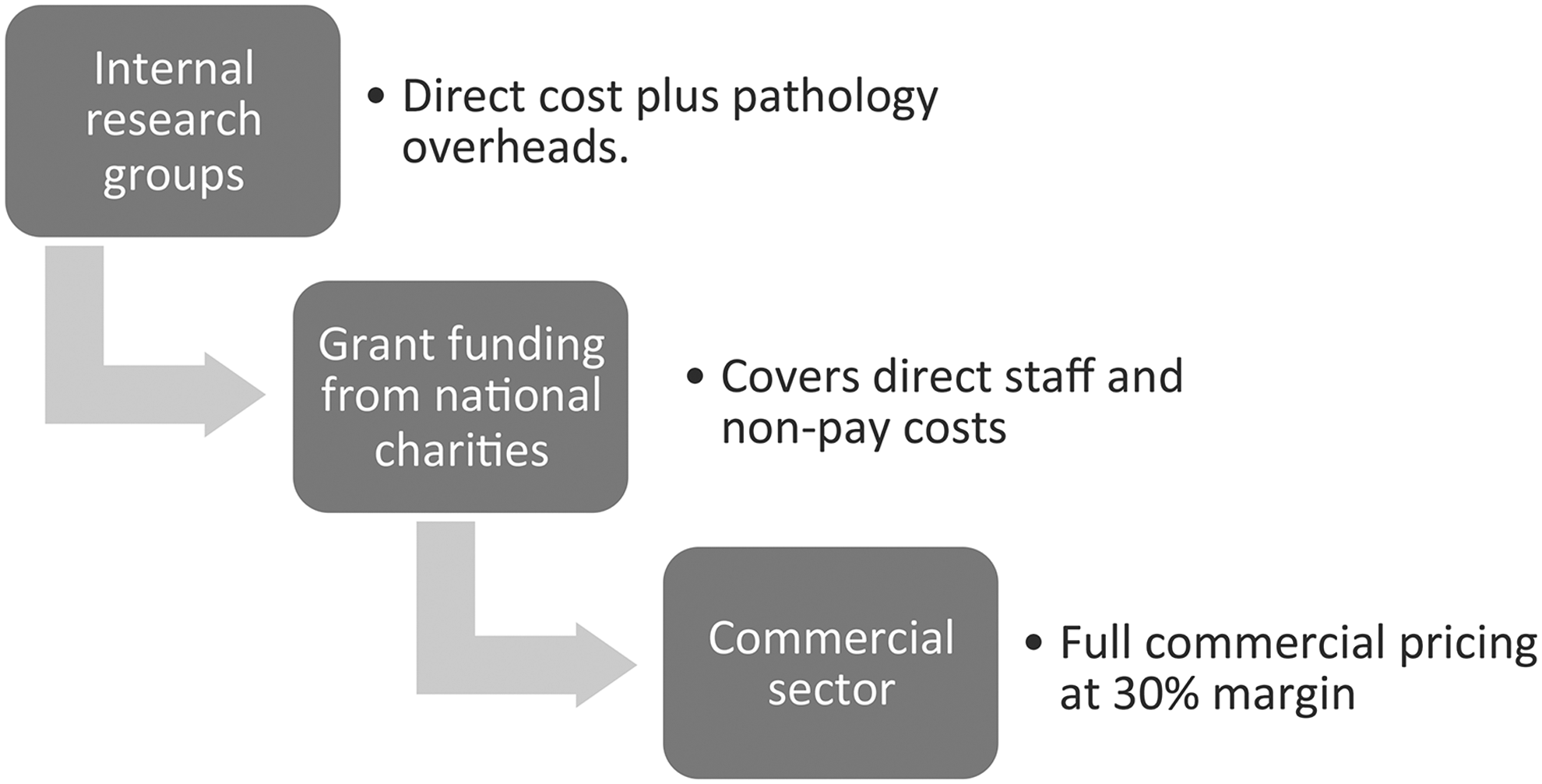
Our stratified approach to cost recovery is shown in Figure 1. In this structured access, industry is required to pay a competitive market rate to cover the cost of the samples, including biobank and Trust overheads. This average market rate did not, however, fully meet the requirements for sustainability. We therefore developed a further, more detailed process in which the provision and processing of the sample, QA and QC, and the provision of data were separately itemized and priced in three tiers, depending on the type and rarity of the sample. The tiers essentially reflected the additional time required to track and access rarer sample sets. This stratified but transparent costing structure has proved acceptable to commercial partners.
The tiered cost-recovery models
Quality assurance
Quality has been achieved by the implementation of carefully considered systems, regular audits, and a clear structure for strategic and operational oversight. Records include the information necessary to ensure that material procured and/or distributed by NHSB can be traced back from the donor to the recipient and vice-versa. Policies are in place covering all key activities such as consent; tissue processing and storage; distribution of body parts, tissues and cells, labeling; equipment maintenance and calibration; cleaning, air control. These documents are dated and reviewed on a regular basis. Annual audits of human tissue are conducted by the NHSB under the supervision of the HTA.
The basic elements of a QM system have also been established and procedures are documented and validated and all steps are traceable. Our QM system covers the identification, collection, indexing, access, storage, maintenance, confidentiality, transfer, and safe disposal of records.
QA is supported throughout the department in the following ways:
• A rigorous quality management system and associated documentation • Strict compliance with HTA requirements • Regular audits of all samples types, documentation, equipment, and data • Registration of BMS/Medical staff • Regular staff appraisal and competency assessment • Recording and regular monitoring of incidents and errors • Response to patient and user feedback
QA procedures operate at every stage of any process, from receipt of specimens to use or release of biological material. Maintenance of QA and internal quality control is underpinned by operational SOPs developed specifically to assure and sustain the quality and security of samples and patient information. Early in our set-up phase, industrial users checked the quality of samples, including RNA quality and methodologies, SOPs, and processes as far back as 1989 before entering into contracts with the biobank.
Rapid response time
Access to the NHSB is regulated by an Access Committee, which has been formed with authority from NHS Research Ethics Service to review and approve applications without seeking further ethical approval. The committee is comprised of researchers in NUH and the University of Nottingham, together with lay membership. Approval is conducted online and takes a maximum of 2 weeks, with the majority of samples distributed within 4 weeks of approval.
Our experience has also demonstrated that the capacity to make a rapid decision—whether positive or negative—was essential to attract and maintain commercial partnership. One of the main challenges to doing so is establishing the feasibility of the study, and whether the bank has the sample set requested; this has prompted the NHSB to prioritize the cataloguing of our tissue archives to enable us to respond to requests quickly.
Cost effective process
As part of our business and financial planning exercise, the NHSB assessed the skill set required to run our bank effectively, including skills in sample processing and assessment, IT, clinical data management and, most importantly, interaction with researchers. We then set out to create an infrastructure in which these resources were provided in the most cost effective manner (i.e., using the lowest grade/banding of posts compatible with the provision of high quality services).
NHSB has also developed a novel model of patient led consent designed, developed and delivered in partnership with our PPI/E (patient and public involvement and engagement) group to provide an effective and user friendly consenting processes which places patient experience at the heart of our activity. Although the principle purpose of this scheme is to enhance the patient experience, this model is also highly cost-effective and therefore sustainable.
Finally, placement of the NHSB in the NHS rather than the University has greatly facilitated the drive to both financial and operational sustainability. This arrangement has enabled close engagement with our pathology services in the essential process of identifying and securing sufficient material for diagnostic purposes as well as for the NHSB. We are also able to use routine Trust processes to collect, process, and deliver biomaterials for small incremental charges, with significant saving in infrastructure costs.
Results
Building on these principles, the NHSB has succeeded in achieving financial and operational sustainability within only 3 years of operation.
Sample collection and release
The NHSB has collected a diverse range of samples sets over the last 3 years (Fig. 2). The majority of collections have taken place in specialties, such as rheumatic diseases, liver disease, respiratory disease, and breast cancer, which represent strategic priorities for the Trust and University, with an associated research infrastructure and highly visible research leadership. Such focused research excellence underpinned by strategic sample collection promotes high rates of sample release for both academic research and partnership with commercial companies. The NHSB has released 45,000 samples in the first 3 years of operation (Fig. 3).

The number of distributed samples and the different customer groups supported by the NHSB.
Activity and expenditure
Income in the years 2011/12 to 2013/14 increased progressively to the end of the pump priming period in March 2014. Details of projected income and expenditure for 2014/15 are shown in Figure 4. Projected commercial income is based on either contracts with existing long term commercial partners, or new contracts that have already been agreed, and is therefore likely to be an underestimate. Expenditure includes full costs of running the biobank, including the pay, non-pay and overheads and capital depreciation.
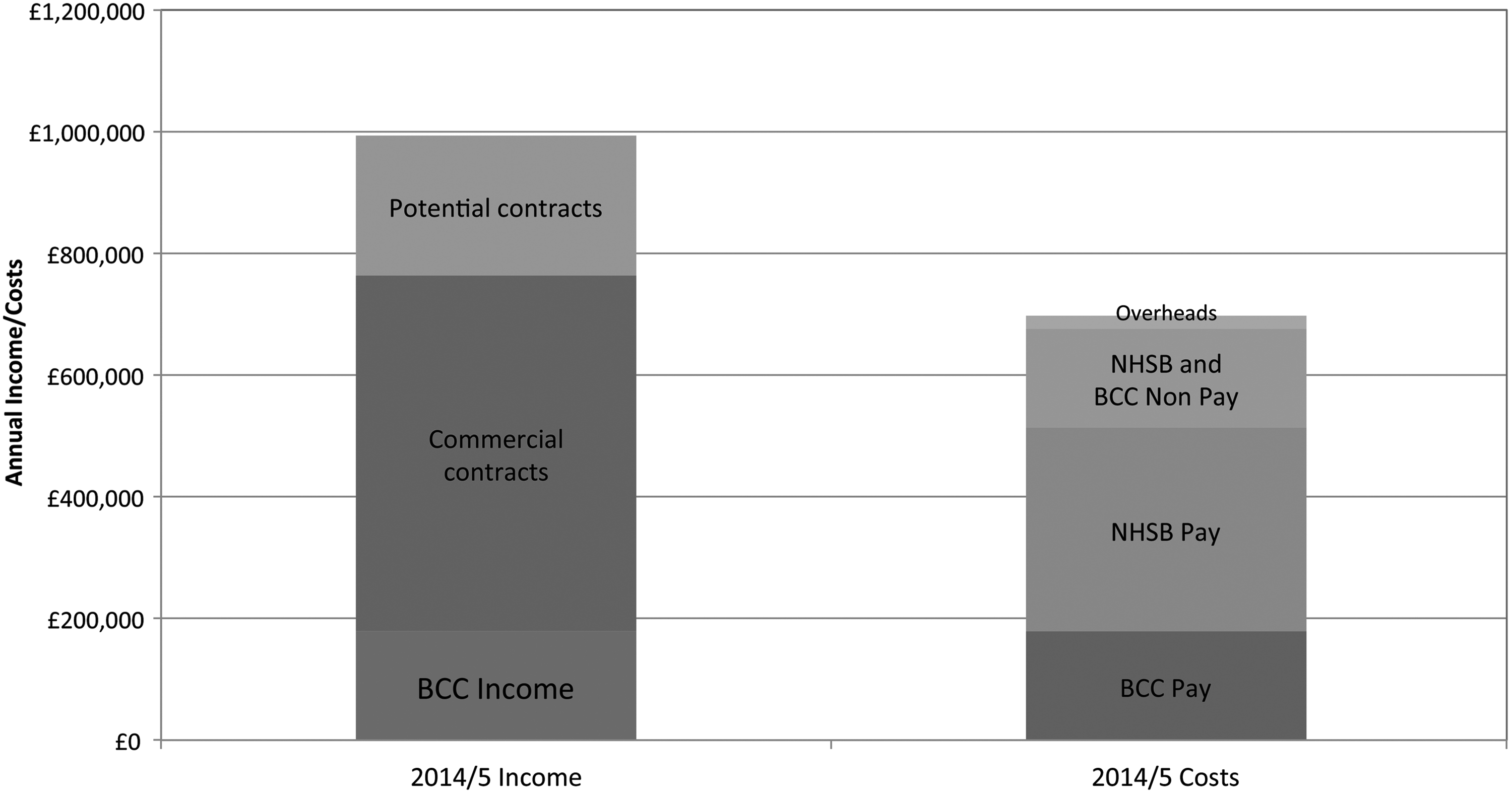
2014/2015 projected income and costs both pay and non-pay with overheads for the NHSB.
Discussion
The NHSB is founded on a strategy of active engagement with academic and commercial stakeholders as both funders and research customers. Our engagement has from the outset included early dialogue with these prospective partners in order to understand their requirements for services, clinical data, and sample sets from either archived or prospective collections. Our aim has been to create dynamic partnerships with commercial companies that work in synergy with the areas of research strength of the Trust/University partnership in Nottingham. In particular, we have sought to establish long term public-private relationships with selected commercial partners. 1 We have also, subject to constraints of IPR and publication, adopted a strategy of requiring the return of data generated by commercial use of our samples with the aim of adding incremental value to our sample sets. We have consequently been able to generate a robust financial platform for future growth.
In order to secure our competitive position in a rapidly changing market, we have set out to develop a number of ‘unique selling points’. The selection of these USPs, which are summarized in Table 1, support our Business Plan and have been informed both by the drive to create innovative solutions to key biobanking challenges, and a keen understanding of the needs of our commercial and noncommercial users. These USPs are intended to establish a market niche for the NHSB, founded on the supply of high quality, high value, and clinically annotated sample sets. Our informatics strategies (not described in this text) will shortly come on stream and we anticipate are likely to reinforce our market profile by radically improving the quality, accuracy, and efficiency of clinical annotation of our biosamples. We have identified our immediate strategic and operation priorities for the maintenance of sustainability in Figure 5.
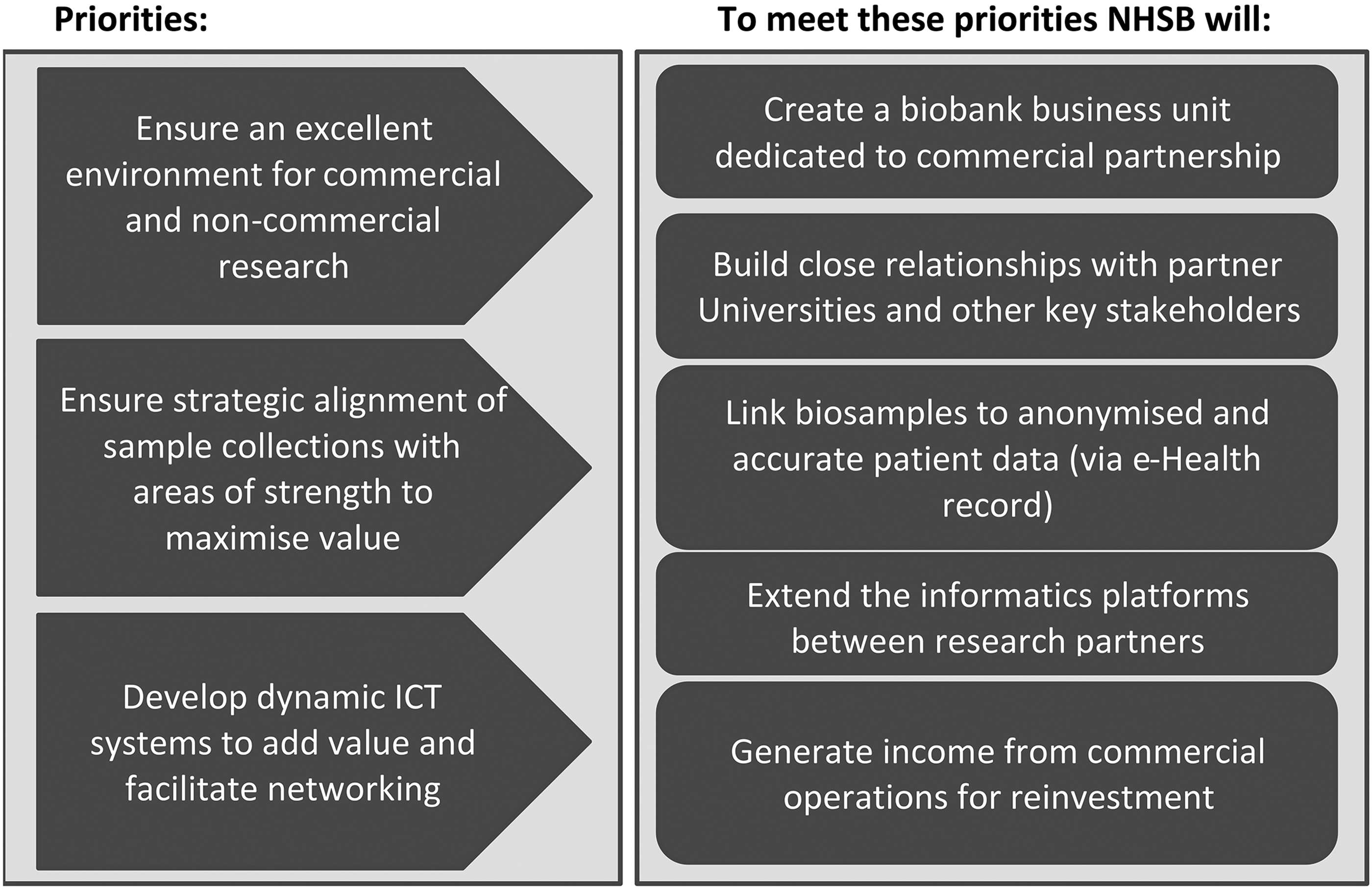
The future priorities of the NHSB and what will be needed to meet these priorities.
We consider that the NHSB model we describe meets the key criteria for financial and operational sustainability recently set out by Watson, Simeon-Dubach and colleagues.2,3 We further strongly support the notion2,3 that societal sustainability is ultimately essential to realizing the enormous potential benefits for health of the biobanking enterprise. This is particularly important against a background of increasing and legitimate focus on personal privacy and a re-examination of the legal framework for the use of personal data for research in the European Union and elsewhere. 4 The NHSB therefore has both a strong focus on patient involvement and engagement locally and a strategy of working through national initiatives to establish a platform for debate and a public mandate for biobanking. We consider full transparency of biobank business, sample usage, and performance metrics to be an essential requirement for public trust in biobanks and therefore necessary for future sustainability. Finally, we believe that ultimately the most important form of sustainability is that of scientific purpose. Therefore, although we have constructed a successful business proposition, we continue to engage in active dialogue with our major academic and commercial stakeholders with the aim of creating focused partnerships to facilitate discovery and accelerate translation of research for patient benefit.
Footnotes
Acknowledgments
We wish to thank all patients who have taken part in the NHSB. We would also like to thank all Biobank staff, the patient advocates, and NUH clinical and allied staff for their valuable contributions.
Author Disclosure Statement
No competing financial interests exist.