
Abstract
Genome-wide sequencing in glioma samples provides comprehensive insights into oncogenesis and malignant transformation. Several distinct biomarkers have been proven to have clinical significance and are being widely applied in routine clinical practice. Standard sample processing lays the foundation for successful molecular testing. In this study, we found intraoperative neuronavigation ensured higher tumor purity during sample collection, and an automated device helped improve DNA quality and increased yields. These two technologies are beneficial for glioma tissue bank construction and provide for accurate molecular testing during routine clinical practice.
Introduction
G
Materials and Methods
Patients enrollment
The Huashan Glioma Tissue Bank (GTB) was established in 2009. Using samples from the tissue bank, we carried out molecular testing at the beginning of 2014. By the end of June 2014, we had performed molecular testing on 132 samples. All patients were given informed consent and the tumor samples were collected and stored according to a previously described protocol. 3 Among these samples there were 51 astrocytomas, 11 oligodendrogliomas, 12 oligoastrocytomas, 53 glioblastomas, and 5 other histological gliomas. Pathological diagnosis was made according the 2007 WHO classification of tumors of the central nervous system.
Sample collection under neuronavigation
Among the 132 samples, 106 were collected according to standard operating procedures of the Huashan GTB. Eight of the remaining 26 cases were biopsy samples that were obtained by using the neuronavigation system (StealStation S7, Medtronic, USA). The other 18 cases were obtained during craniotomies for glioma resection. Neurosurgeons helped to collect tumor samples with neuronavigation during the operation, and then transferred the samples to a technician for additional processing. The target tumor sample was selected according to RANO Criteria.4,5
DNA extraction and quality assessment
132 tumor frozen samples were obtained from the Glioma Tissue Bank with the assistance of biobank management software. A sample of up to 10 mg tissue was dissected, followed by homogenization with an ultrasound homogenizer (BIOSPEC, USA). The resulting homogenate was separated into two parts for DNA extraction by manual and automated operations separately. Manual DNA extraction was performed according to the standard protocol for the QIAamp DNA mini kit (Qiagen, Cat: 51306). Automated extraction was performed on a liquid handling workstation (Chemagic Prepito, USA) equipped with wash stations for the array of 12 samples. The Prepito Genomic DNA kit (Cat: cmg-2027) compatible with the Chemagic workstation was chosen. The whole procedure was performed according to the manufacturer's instructions. DNA concentration and the A260/A280 ratios were assessed by NanoDrop 2000 (Thermal Scientific, USA).
PCR and sequencing analysis
DNA was amplified in a 10 μL reaction system containing 1 μL template, 10 mM Tris-HCl (pH 8.3), 50 mM KCl, 2.5 mM MgCl2, 0.2 mM of each deoxyribonucleoside triphosphate, 0.4 mM of each primer (Forward: 5′-CGGTCT TCAGAGAAGCCATT-3′, Reverse: 5′-CACATTATTGCC AACATGAC-3′), and 0.2 U of AmpliTaq Gold DNA polymerase (Life Technologies Corporation, China). PCR conditions included 95 degrees for 10 min, 45–50 cycles of 95°C for 20 sec, 60–66°C for 20 sec, and 72°C for 30 sec, and a final extension step of 72°C for 3 min. PCR products were then treated with exonuclease I and thermosensitive alkaline phosphatase (TakaRa Biotechnology Limited, China). Sequencing was performed using the BigDye Terminator Cycle Sequencing kit v1.1 (Life Technologies). The products were resolved in the Genetic Analyzer 3130xl and analyzed by Sequencing Analysis software.
Statistical analysis
Statistical analysis was performed by IBM Statistical Product and Service Solutions version 20 (SPSS Inc., IBM Corp, USA). The DNA concentration and A260/A280 ratios from manual and automated operations were compared with t-test and Chi-square test, respectively. All tests were two-tailed, with a confidence interval of 95%. P values of less than 0.05 were considered statistically significant.
Results
Routine procedure for molecular diagnosis testing in clinical practice
Glioma samples were collected according to the “Huashan Glioma Tissue Bank Project” protocol. In addition to saving a portion of the tumor for deposit in the tissue bank, a small portion was allocated for molecular testing to provide feedback to clinical neurosurgeons. The workflow was as follows: 1) DNA extraction; 2) Molecular testing (gene mutational analysis, MGMT methylation assessment, copy number variation by FISH); 3) Results analysis and report publication; 4) Molecular data compiled and input into glioma database; 5) Personalized treatment regimen designed by neurosurgeons based on the molecular diagnostic result; 6) Patient follow-up. The whole procedure duration was 10 days, to provide neurosurgeons with adequate time to develop adjuvant treatment plans before patients were discharged (Fig. 1).

The workflow of clinical molecular testing based on Huashan Glioma Tissue Bank Project.
Precise tumor collection under neuronavigation during operation
Due to the classic pathological features of vascular proliferation and necrosis, along with intra-tumoral hemorrhage, glioma tumor purity will be obviously affected during sample collection using the naked eye, even by an experienced technician. Especially for low grade glioma, it is challenging to distinguish the tumor cells from normal brain components. We tried to collect tumor tissues assisted by MR image-guidance during neuronavigational surgery in 26 cases (Fig. 2). All of the cases had a tumor content >70% when collected under neuronavigational resection. Only 73% of tumors collected by a technician after tumor removal achieved those criteria. Among the remaining 29 cases, tumor content was lower than 50% and mixed with significant amounts of vascularization, necrosis, and neurons that may interfere with molecular testing results (Fig. 3).
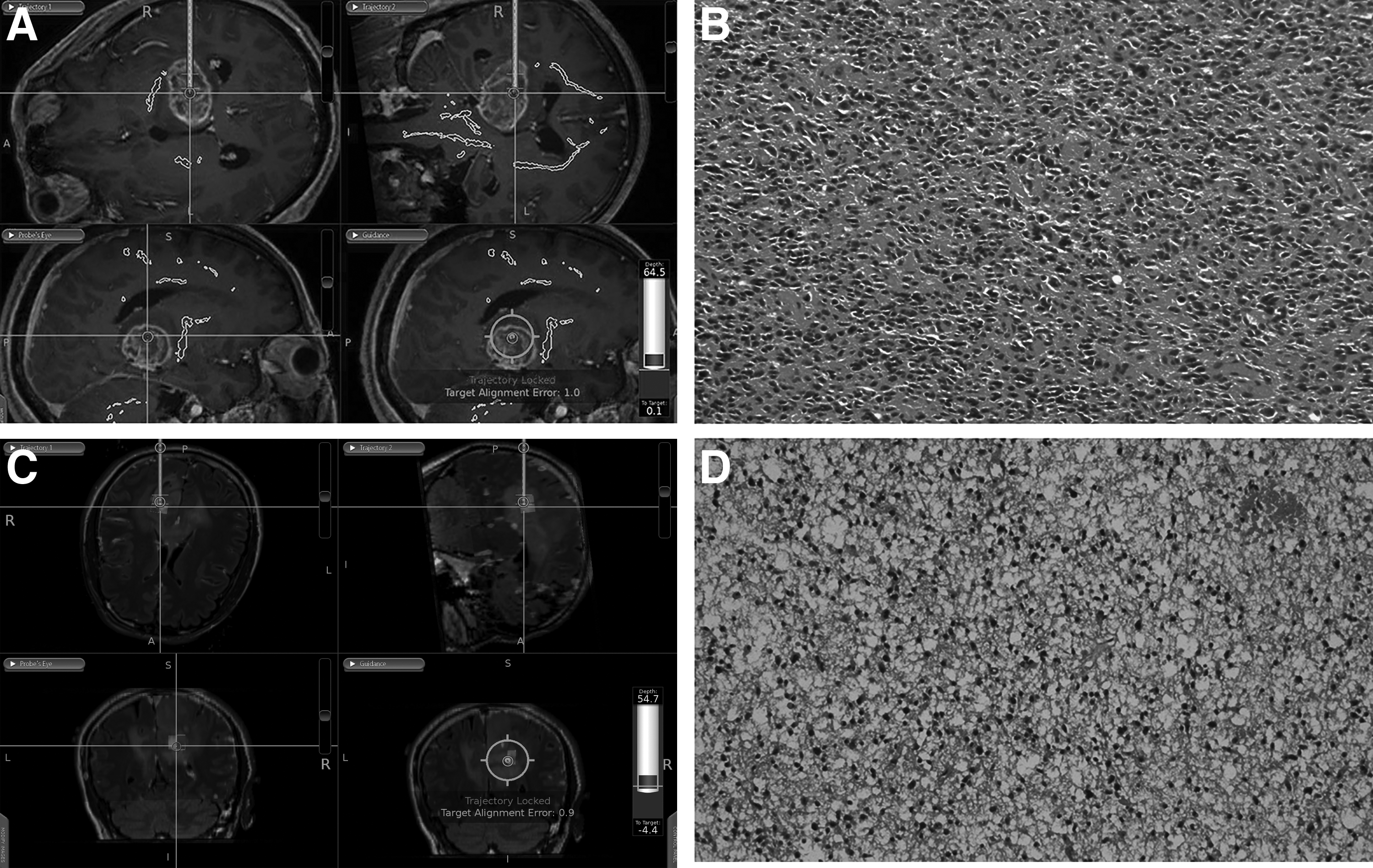
Tumor sample collection with assistance of MR image-guidance during neuronavigational surgery ensures high purity of glioma. (
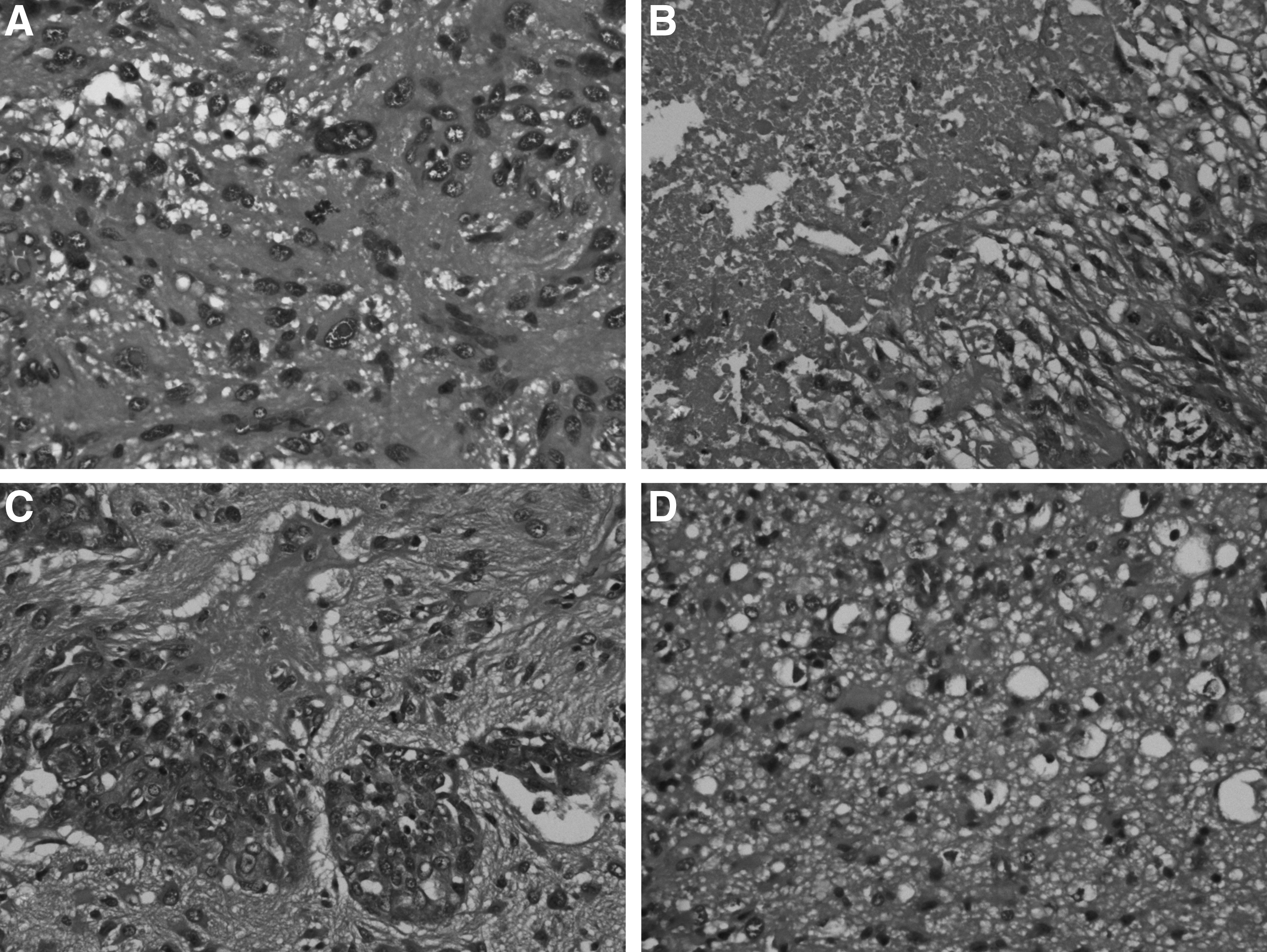
HE (x200) slides indicated vascular proliferation, necrosis, and neural cells would be mixed with tumor cells during sample collection.
Higher quality of DNA extracted by automated method
Genomic DNA extraction is a very important part of the process for standardizing diagnostic procedures. Normally we have extracted DNA using manual commercial kits. For this project we compared an automated extraction device with manual extraction in terms of DNA quality and amount. For the automated device, the average DNA concentration from 132 tumor samples was 136.83±52.27 ng/μL. The manual manipulation method resulted in DNA concentration averaging 53.59±36.23 ng/μL. The results showed that the automated method yielded significantly more DNA than the manual method (p=0.000) (Fig. 4). In addition, more DNA samples obtained by automated method had A260/A280 values within the qualified range of 1.80–2.00 6 than those from the manual procedure, but with no statistical significance (SD: 0.074 vs. 0.141, p=0.401) (Fig. 5). However, the automated method was significantly less time-consuming. Every 12 samples totaled only one hour to complete the entire DNA extraction procedure, while 1.5 hours were needed for the manual operation by a well-trained technician.
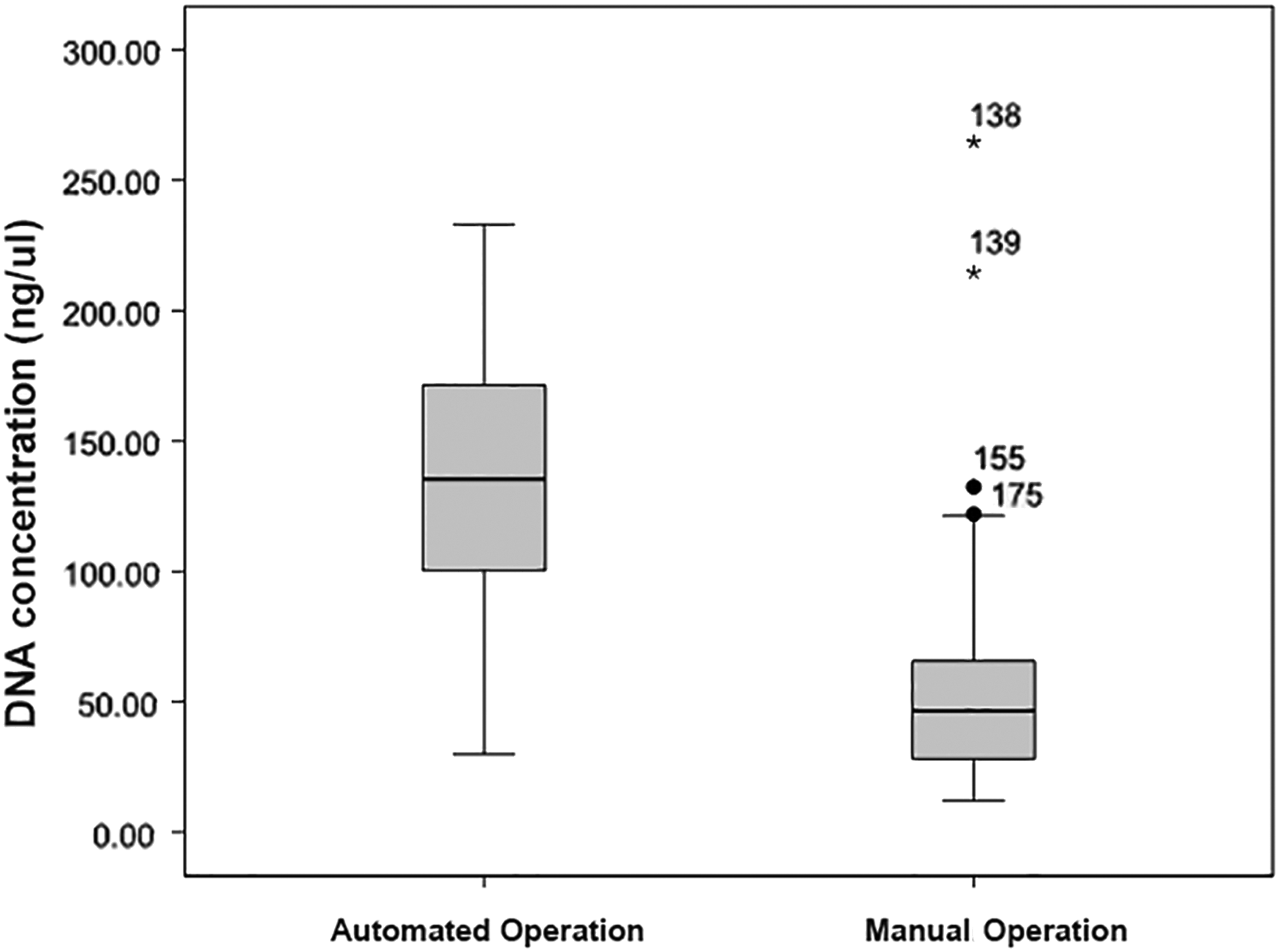
Higher DNA concentration obtained by automated method versus manual operation with commercial DNA kit (p=0.000).
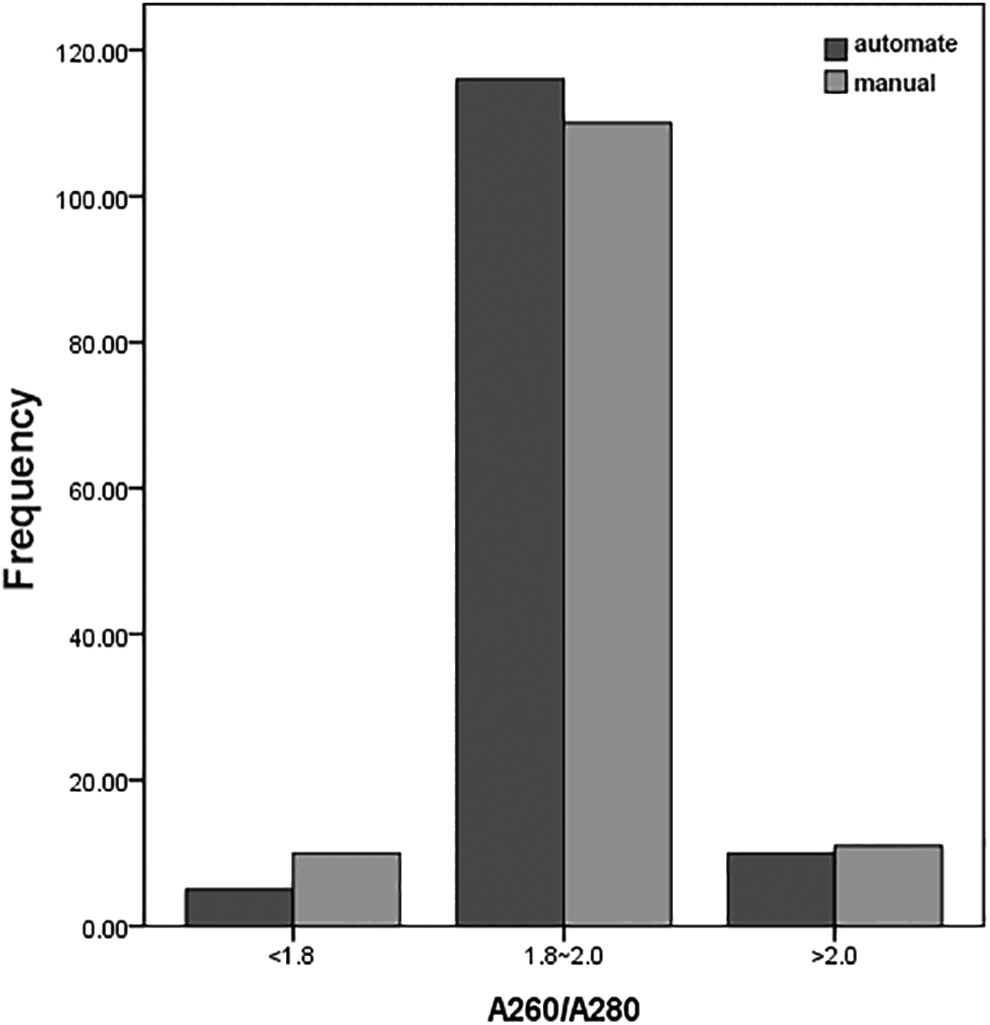
No significant difference of DNA quality was observed by automated method and manual manipulation, while more samples fit into qualified range of DNA extraction. (SD: 0.074 vs. 0.141, p=0.401).
Good DNA quality and tumor purity provides accurate molecular testing result
In order to evaluate the practical efficiency of extracted DNA, we performed PCR amplification and sequencing for the IDH1 gene. Eight PCR reactions failed (Fig. 6a), and sequencing results for seven cases had high background signals (Fig. 6b). All of these cases belonged to the subgroup with tumor content <70% with obvious vascular proliferation, necrosis, and neural cells. Further analysis found that four samples were of low DNA concentration (<30 ng/μL), 3 were necrotic (>50%), and 1 contained neurons (>50%), resulting in PCR reaction failure. Five out the seven samples with high background signals featured a mixture with more than 50% blood cells.
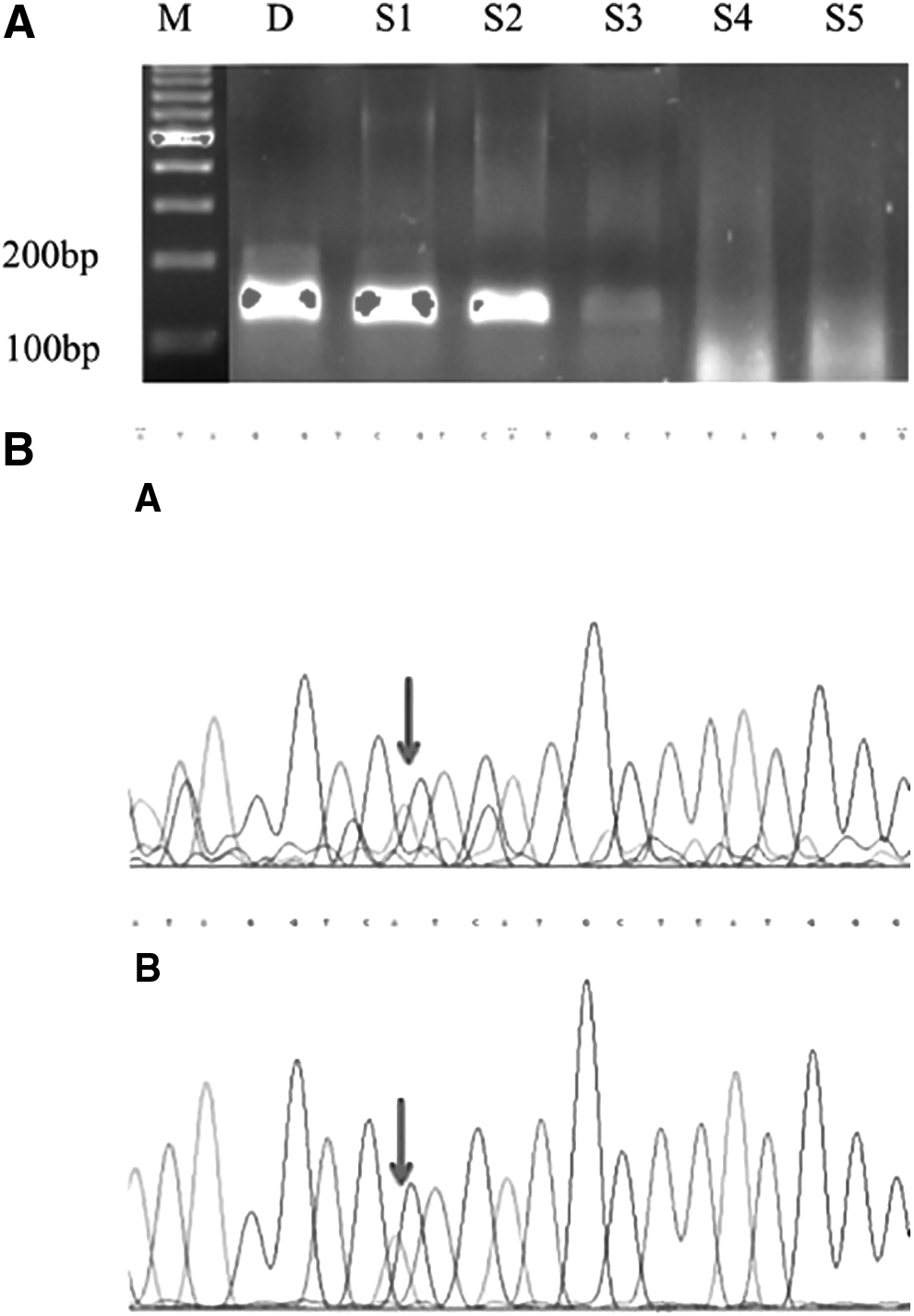
PCR reaction was performed to evaluate the practical efficiency of extracted DNA. (M, marker; D, positive control of placenta DNA; S1 and S2 are qualified DNA samples, S3 is the sample with DNA concentration <30 ng/μL, S4 and S5 are samples mixed with necrosis and neurons more than 50%).
Discussion
Genome-wide sequencing of glioma has provided new insights into tumorigenesis and malignant transformation during the past 10 years. Utilizing tumor samples provided by large glioma tissue banks, several leading organizations in glioma research have mapped out the genetic background of glioma,2,7 making a panel of biomarkers available for clinical diagnosis and personalized treatment, and overcoming the limitations imposed by histology diagnosis and the WHO grading system. Many neurosurgical centers have applied molecular diagnosis in routine clinical practice and an abundance of clinical trials. 8 IDH mutation, MGMT promoter methylation, 1p19q codeletion, EGFR amplification, and TERT promoter mutations were presented as five symbolic biomarkers for glioma diagnosis, prognosis, and for deciding treatment options. 9 Especially with regard to IDH, MGMT, and 1p19q, neurosurgeons can tailor optimized adjuvant treatment for individual glioma patients, which may result in the most improved outcome for patients. This is the major reason we chose these five biomarkers for clinical molecular testing.
Glioma grows diffusely and sometimes it is impossible to collect tumor tissues with very high purity when assessed by the naked eye, even for a well-trained technician. Tumor content of >70%, excluding blood cells, neural cells, and necrosis as much as possible are the basic conditions for accurate molecular diagnosis, especially for analyses by PCR and sequencing. 10 In our case cohort, tissues from 26 cases (8 for biopsy and 18 for craniotomy) were collected with assistance of MR image-guidance during neuronavigational surgery. The most representative tumor sample was selected according to RANO Criteria. Interestingly, tumor content of more than 70% was guaranteed with the neuronavigation method. Twenty nine (27.4%) samples collected by a technician were found to have tumor contents of <50%, and were mixed with blood cells, necrosis, and neurons. The other advantage was that tumor tissues could be obtained just after resection from patients to ensure the best DNA integrity. However, two critical points should be noted for such efficient collection: 1. Close cooperation with neurosurgeons and technicians requires attention; 2. The advanced neuronavigation system should be located in a surgical suite. Without such considerations, the method for precise tumor sample collection is hard to establish in the glioma tissue bank construction.
DNA extraction from tumor tissue is very important for follow-up molecular testing. Good DNA quality and quantity are essential for the accuracy of results. Currently commercial DNA extraction kits are widely used with good efficiency. The QIAamp DNA kit is highly recommended for research work. Irrespective of sample size, the final value of DNA concentration and purity remains constant with respect to its standard protocol. 6 However, samples must be processed one by one manually using this commercial DNA kit. Such manual processing is likely to produce heterogeneous results. For our study, we used an automated device to perform DNA extraction, leading to higher DNA yield and relatively better DNA quality with reference to recognized standards. 11 The whole procedure with a set of 12 samples saved half an hour compared to the manual procedure. In addition, we think homogeneity was an obvious advantage, since every step was carried out at one pace under the same conditions. With respect to economics, the average cost for each sample processed is the same with both methods. However, the ownership of one automated DNA extraction device is an advantage. This also should be taken into consideration for total cost. But in the long run, whether glioma tissue DNA extraction by the automated method is more cost-effective than the manual method has not been evaluated.
To evaluate the practical application of the extracted DNA, we also did PCR and sequencing as commonly performed. PCR amplification for IDH1 is a short segment of 122 base pairs. Since glioma is a highly heterogeneous malignant brain tumor, tumor DNA concentration is very important for successful PCR reactions, because non-tumor components will not present with distinct tumor-related genetic alterations. This finding has been validated by many research groups. 12 A high background signal is a common problem in genetic sequencing for accurate interpretation of results. In glioma, we found tumor tissue mixed with blood cells will give rise to such a problem. Although the sample number in our cohort is not large, some research groups also mentioned this kind of phenomenon in analyses of other cancer types. 13 This point highlights the importance of sample collection with as much pure tumor content as possible. This is the reason we attempted to collect samples using neuronavigation. Nevertheless, our sample size using the MR image-guidance method is still small. A large cohort of samples is needed to further validate this result before it is officially introduced into the standard glioma tissue bank protocol.
In conclusion, glioma is a special tumor type characterized by diffuse growth. Genetic heterogeneity contributes to the development of the molecular diagnosis, which allows neurosurgeons to develop a clear concept of the tumor makeup and how to treat it. Our experience of molecular testing based on the glioma tissue bank project will be a pilot demonstration project for many neurosurgical centers domestically. Tumor collection under neuronavigation and the automated DNA extraction method form the basis for a more accurate molecular diagnosis. We will introduce these methods into our glioma tissue bank protocol in the future for a large sample cohort validation.
Footnotes
Author Disclosure Statement
No competing financial interests exist. This work is supported by Shanghai Committee of Science and Technology, China (No. 12DZ2295003) and National Key Basic Research Program of China (No. 2013CB932502).