
Abstract
Human tissue biorepositories have become key platforms for the acceleration of basic and translational biomedical research on cancer in China. The maintenance of sufficient amounts of tumor cells is critical for a wide variety of cancer studies. Ensuring the high quality of frozen stored tissue specimens is a crucial requirement. However, different tumor locations and various methods of tumor tissue removal can lead to variable numbers of tumor cells from banked tissue specimens. Thus, an effective method to assess the tumor cell content is essential for tissue samples in biobanks. In the present study, the mirror image method was used to evaluate the amount of tumor cells in stored tumor tissues of six common cancer types, including solid and hollow organ cancers. All tissues were stored in the Tianjin Medical University Cancer Institute and Hospital (TMUCIH). Histological assessment was performed by pathologists who conducted morphological diagnoses of tumor percentage on mirror image sections of frozen stored samples that were stained with hematoxylin and eosin (H&E). Results showed that the tumor percentage of solid organ cancers was higher than that of hollow organ cancers (χ2=17.11, p<0.0001). Among solid organ cancers, the highest tumor percentage was observed in renal tumor tissues, and likewise esophagus tumor tissues had the highest tumor content among hollow organ cancers (multiple tests, p<0.05). Three kinds of samples, which showed higher proportions of tumor content under 25%, were stomach, liver, and colorectal cancers, and the proportions were 15.0%, 10.9%, and 10.6%, respectively. Therefore, histological assessment based on the review of mirror-image H&E sections offers the most direct and objective judgment. The results can not only be applied to the tissue quality feedback process of biobanks, but also guide a wide variety of scientific studies.
Introduction
T
Despite the notable work of JTB, the lack of high quality tumor tissues has limited the advancement of translational research and personalized medicine in China. A biobank that provides specimens should be able to ensure that the quality of the collected frozen tissue samples meets the high quality requirements of future studies. Thus, tissue quality control is necessary. Quality control (QC) procedures, including molecular and histological assessments, play an important role in the quality assessment of stored tissue samples 1 . Unlike common molecular assessments, such as RNA integrity and DNA quality testing,2–5 pathological diagnosis or histological composition of the stored tissues must be acquired before a sample is used. In some studies, approximately 10% of the samples have been deemed unsuitable for molecular analysis because of sampling problems with the tissue (e.g., no tumor, insufficient tumor cells, and insufficient viable tumor cells).6,7 Therefore, the histological assessment of stored tumor tissues is necessary.
However, such assessments are rarely conducted in China. Three general methods for pathological assessment are based on frozen sections, mirror images, and imprint cytology (IC). 8 Frozen sections could represent the reference samples in terms of their morphological control. However, this method is time consuming, can easily lead to nucleic acid degradation, and consumes tissue samples. IC has been recommended by several studies as an alternative to the use of frozen sections for diagnosis. However, this method may require better storage conditions in the tissue bank.
The mirror image method involves the regular morphological analysis of a tumor tissue sample obtained near the frozen tissue sample. Although the method is limited by the prescribed analysis of the tissue adjacent to the frozen one and not of the frozen tissue itself, this technique provides high-quality information regarding the morphological aspects of the frozen tissue. Furthermore, this method can be easily implemented. Given the practicality and requirements of these methods, we have performed regular morphological quality analysis of banked tumor tissue in the biobank by using the mirror image slides since 2012. We evaluated the tumor content by counting the cellular percentage, conducted the morphological analysis of the stored tumor tissue samples, and analyzed the histological quality of different cancer types in the biobank.
Materials and Methods
Based on standard operating procedures for tissue collection according to NCI Best Practices for Biospecimen Resources, and with the consent of the patients, we obtained three fresh tumor tissues from each case when tumor sizes were appropriate. Samples were collected according to the mirror image method above mentioned (Fig. 1). Generally, the first tissue sample was embedded in paraffin (formalin-fixed paraffin-embedded, FFPE) to produce a mirror image sample on a paraffin block. This sample was sectioned and then stained with hematoxylin and eosin (H&E). The results were used to assess the other two corresponding tissue samples, which were snap-frozen and transferred to the freezer for storage. Morphological assessment was performed by two pathologists who reviewed the respective H&E sections in the biobank. The evaluation of tumor cell content was scored using four levels (<25%, 25%–50%, 50%–75%, and >75%) to determine the percentages of a wide variety of tumor cells (Fig. 2A–2H).
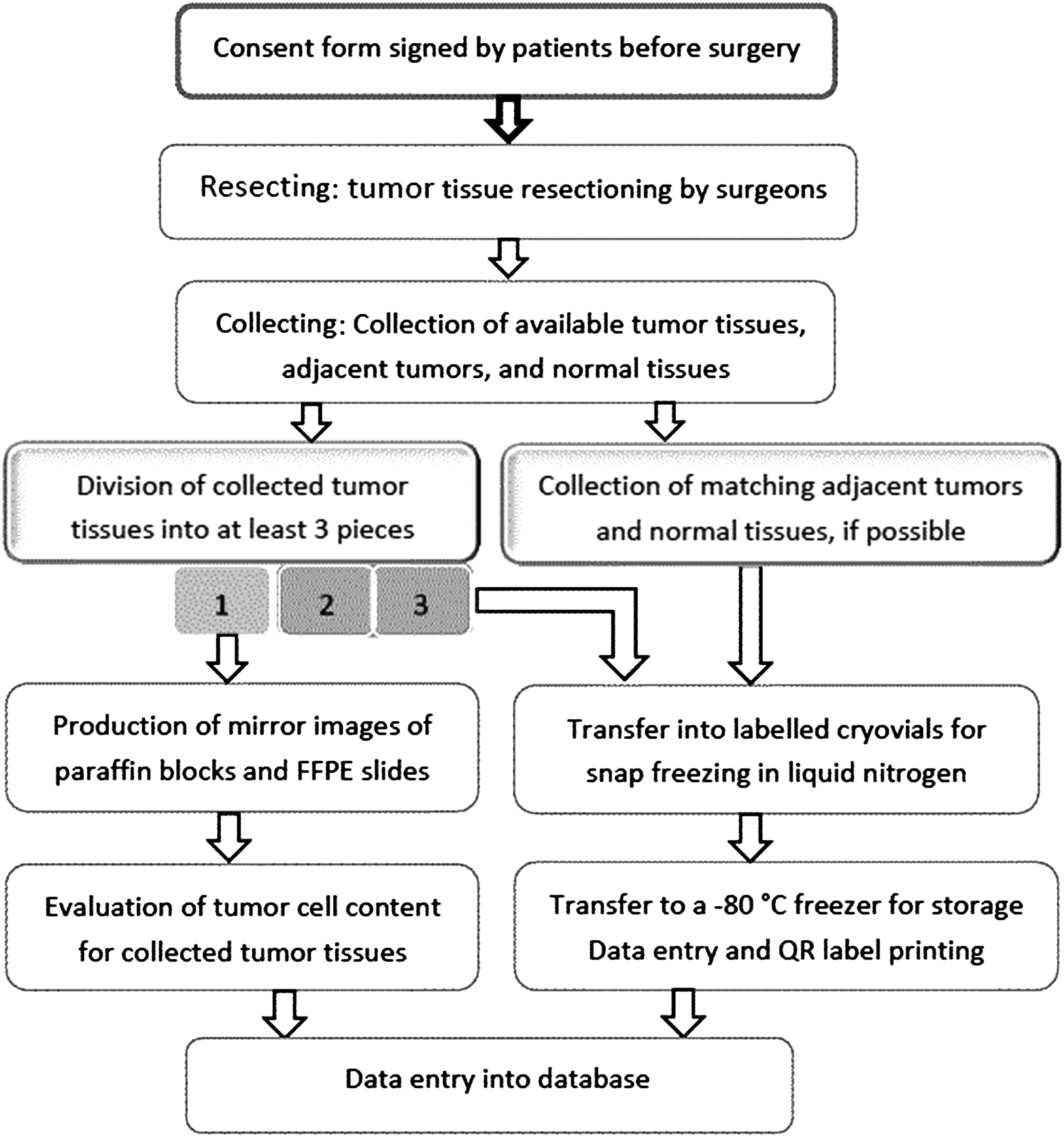
Flow chart for fresh tissue sample collection.
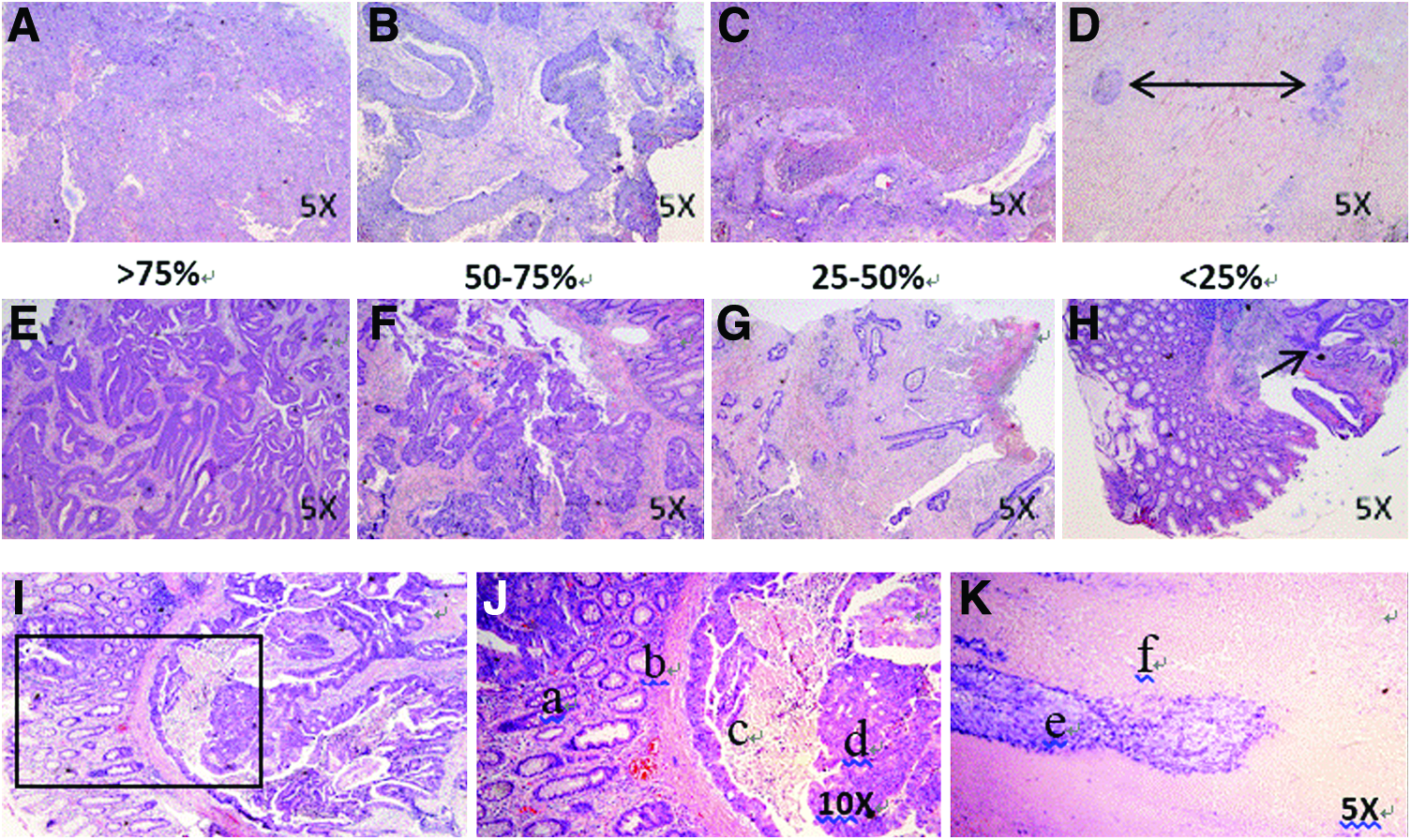
Evaluation of the tumor cell content of stored tumor tissues using mirror images.
When a consensus was reached during the evaluation, the average percentage of tumor cells for each tumor tissue sample was reported by the pathologists. We focused on the appraisal of six cancer types using matching H&E slides. The samples included kidney, liver, lung, esophagus, stomach, and colorectal tissues. These tissue samples were grouped into solid organ cancers (kidney, liver, and lung) and hollow organ cancers (esophagus, stomach, and colorectal). The Kruskal–Wallis test was used to test for differences in the histological quality among all groups. The Nemenyi test was applied for multiple testing within the various organ groups. All statistical analyses were performed using SAS for Windows, version 9.3. Significance was defined as p<0.05.
Results
A total of 1221 stored tumor tissue samples with definite pathological diagnosis and covering six common cancers were evaluated in the present study. The percentage of tumor cells was determined by reviewing matched H&E-stained slides. The distribution of all tissue samples, which consisted of two main kinds of organ sources, namely, solid and hollow organs, is summarized in Table 1. The solid organ tissues included 110 kidney samples, 110 liver samples, and 331 lung samples. The hollow organ tissues were composed of 95 esophageal samples, 273 stomach samples, and 302 colorectal samples. A significantly higher proportion of samples with high tumor cell content was observed in the stored tumor tissues from solid organs, as compared with those from hollow organs (Kruskal–Wallis test χ2=17.11, p<0.0001). Approximately 78.3% of the solid organ tumor tissues had tumor cell content higher than 50%, whereas only 72.6% was observed for the tumor tissues from hollow organs cancers (Fig. 3A). The results showed that the collected tumor tissues of solid organ cancers had higher histological quality than those of hollow organ cancers.
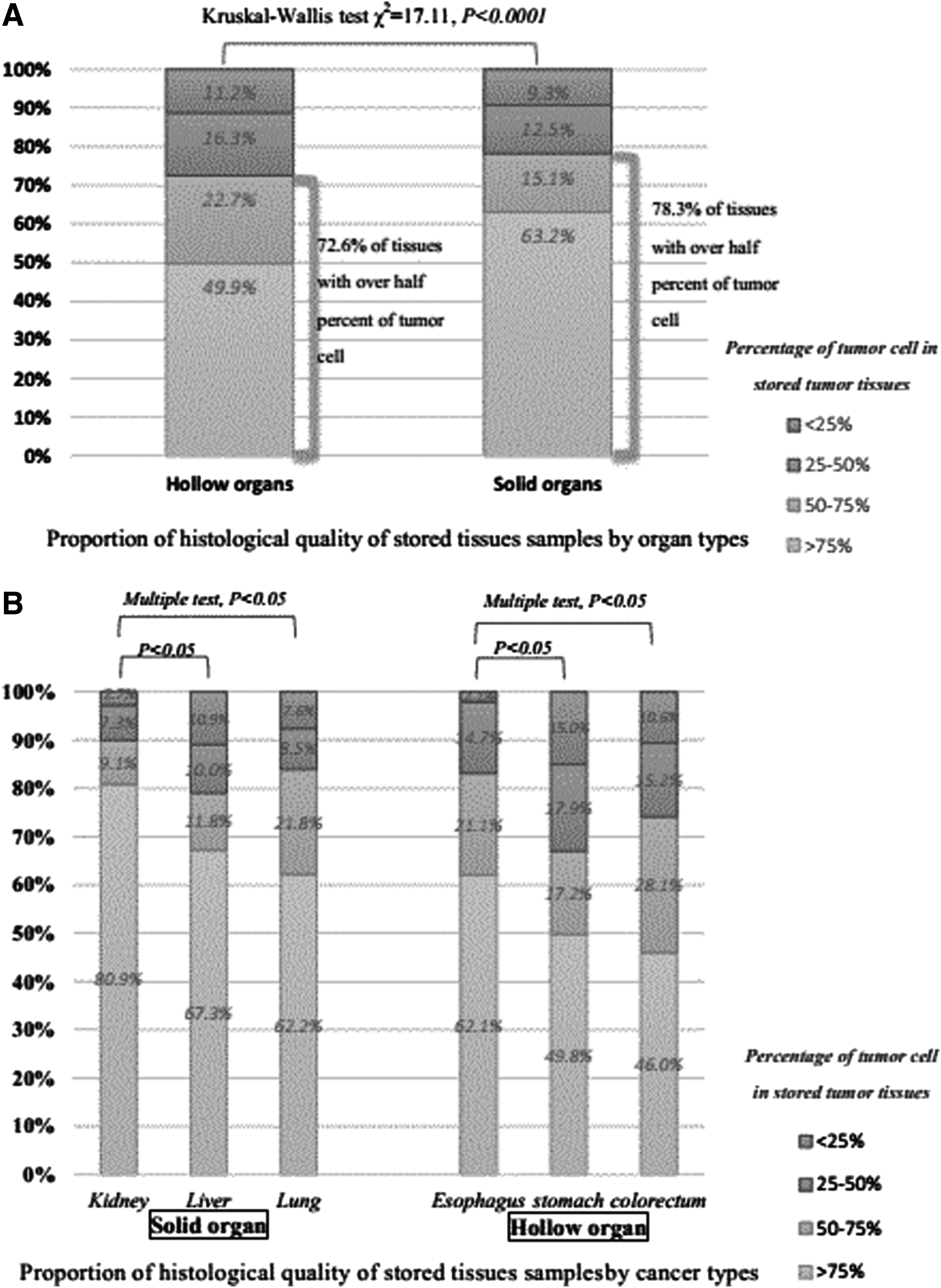
Comparison of morphological assessment in stored tumor tissues.
To further evaluate the histological quality of collected tumor tissues among the various cancer types, we compared the proportion of tumor tissues with high tumor cell content in the different cancer types within each organ group. A significant association was found between the levels of tumor content and the cancer types for each group by comparing the values in pairs. The results indicated that the collected kidney and esophagus tumor tissues had higher histological quality than the other cancer types in their respective groups. The kidney samples were of higher quality than the liver and lung samples, whereas the esophagus samples were better than the stomach and colorectum samples (Fig. 3B; multiple tests, p<0.05). The proportion of collected tumor tissues with over 75% tumor cell content was 80.9% and 62.1% in the kidney and esophagus tumor tissues, respectively.
Furthermore, three kinds of samples, which showed higher proportion of tumor content under 25%, were stomach, liver, and colorectal cancers, and the proportions were 15.0%, 10.9%, and 10.6%, respectively (Table 2). We found that the inferior quality of the gastric cancer samples could be attributed to their inherent morphological structure (Fig. 2H–2I). The lower tumor cell content of liver and colorectal tissue samples could have been caused by the abundant sites of large-scale necrosis (Fig. 2K). The primary reasons for these results are discussed in the next section.
It signifies each cancer type occupies the constituent ratio of the same type.
Discussion
The role of human cancer biobanks in the prevention, diagnosis, and treatment of cancer, as well as in other biomedical studies, has become increasingly critical. A necessary prerequisite for the success of biobanks is the ability to obtain high-quality biospecimens to meet a diverse range of research demands. Several aspects, including environmental factors, the laboratory banking process, and personnel experience, influence the quality of samples. Nevertheless, a quick and efficient feedback system for QC is necessary for the evaluation of work procedures and improvement of the daily efficiency of biobanks. To assure that banked specimens have an acceptable degree of integrity and are ready for use, most repositories in China utilize RNA quality assessment to establish QC. 9 However, RNA quality assessment is not relevant to the morphological analysis of samples. For instance, this method cannot evaluate the tumor cell content, the occurrence of hemorrhage, and the level of necrosis. Most of the frozen stored specimens in the cancer biobank could match corresponding paraffin blocks and H&E sections without affecting the pathological diagnosis. The considerable increase in the number of frozen stored tissues requires effective methods that can promptly provide tissue quality assessment. As previously mentioned, tumor cell content of more than 50% occurred in solid organs more than in hollow organs (78.3% vs. 72.6%). This trend can be mainly attributed to the methods of specimen dissection. A majority of the technical personnel collect the full thickness of tumors from hollow organs. Thus, the acquired samples contain tumor tissues and a variety of stromal elements (Fig. 2I) that could decrease the tumor cell content. Regardless of whether the collected tissue samples are from solid or hollow organ tumors, the internal differences within each group were confirmed.
We found that the tumor cell content of renal cancer samples is significantly higher than those of liver and lung cancer samples. Most renal cancers are easy to observe in terms of their malignant tumor tissues, hemorrhage, and necrosis. Lung neoplasms vary regardless of the tumor location and morphology. Thus, lung tumors are generally difficult to distinguish. Although kidney and lung tissues can both be accurately collected, more tumor components are still present in the former, as compared with the latter. Except for the tumor cells, lung cancer tissues have relatively high quantities of stromal components such as glands, cartilage, necrotic tissue, and inflammatory components. Similarly, tumor cell content of esophageal and colorectal cancer samples is higher than that of gastric cancer. This trend can be mainly attributed to the accuracy of collection by cancer biobank technicians. Sample collection is influenced by the inherent morphological structure of the tumor cells, including their growth patterns, pathological types, and the proportion of individual components (Fig. 2J). Nevertheless, the accurate and proficient collection by each technician in a biobank cannot be separated from the targeted training of the personnel, as indicated by the results of histological evaluation.
Consequently, histological assessment through the review of mirror images of morphological H&E sections from matched frozen tissue specimens offers the best direct and impartial judgment. This method can be applied to provide feedback on the tissue quality of samples in biobanks. For instance, when the pathologists in our biobank review pieces of necrotic areas from several H&E sections by microscopy (Fig. 2K), these experts can quickly remind the relatively new technical staff members and advise them on how to decrease if not completely avoid errors during sample collection. Technicians should be able to select independently the right location for sample collection, and should be able to remove necrotic tissue or other nontumor components as much as possible. The different levels of tumor cell content in the collected samples could be caused by the morphological structure of the tumors. However, skilled personnel who can accurately locate specimens are equally critical to efforts to improve the quality of specimens further and to decrease the variable location of the primary sites of tumor samples. Given the above-mentioned factors, histological assessment can be used as a QC method to provide an efficient means of increasing the proportion of tumor cells in each tissue sample. QC programs of biobanks should include training in avoiding the collection of necrotic tissue and other nontumor components, as well as in the collection of the mucosa of tumor tissues from hollow organ cancers rather than their full thickness whenever possible.
The histological assessment of tumor tissue samples is widely applicable in biomedicine. The biobank has supported several paraffin tissue-based technical approaches and medical studies. These techniques include the construction of tissue microarrays (TMAs) and immunohistochemistry for protein localization. An adequate quantity of tumor cells from donor blocks is a crucial concern for TMAs construction, which is based on the previous tumor percentage scores of H&E sections as provided by our pathologists. Furthermore, the same principle is applicable to immunohistochemistry. Ultimately, researchers should only select the desired FFPE tumor sections and avoid samples with necrosis, inflammation, and hemorrhage. In recent years, the use of FFPE tissue sections for molecular assays has gained notable progress.10–14 These sections represent a valuable source of retrospective biological material for researchers. As previously mentioned, successful molecular oncology testing is dependent on the accurate assessment of the percentage of malignant cells in the analyzed tissue samples from fresh, frozen, or FFPE tissues.
In summary, the histological assessment of tumor tissue samples provides quick QC feedback, and may be used as a downstream platform to assure sufficient quality and quantity of a tumor sample.
Footnotes
Acknowledgments
We thank Jingjing Shi, Wenbin Xia, Yu Jiang, and Zhiju Xu for their technical assistance from Cancer Biobank of Tianjin Medical University Cancer Institute and Hospital.
Grant Support: National Science and Technology Major Project of China (No.2013ZX09303001 and No.2011ZX09307-001-04) and National Natural Science Foundation of China (No.81302487). Fund of National Foundation for Cancer Research (US).
Author Disclosure Statement
No competing financial interests exist.