
Abstract
Mesenchymal stem cells (MSCs) hold many advantages over embryonic stem cells (ESCs) and other somatic cells in clinical applications. MSCs are multipotent cells with strong immunosuppressive properties. They can be harvested from various locations in the human body (e.g., bone marrow and adipose tissues). Cryopreservation represents an efficient method for the preservation and pooling of MSCs, to obtain the cell counts required for clinical applications, such as cell-based therapies and regenerative medicine. Upon cryopreservation, it is important to preserve MSCs functional properties including immunomodulatory properties and multilineage differentiation ability. Further, a biosafety evaluation of cryopreserved MSCs is essential prior to their clinical applications. However, the existing cryopreservation methods for MSCs are associated with notable limitations, leading to a need for new or improved methods to be established for a more efficient application of cryopreserved MSCs in stem cell-based therapies. We review the important parameters for cryopreservation of MSCs and the existing cryopreservation methods for MSCs. Further, we also discuss the challenges to be addressed in order to preserve MSCs effectively for clinical applications.
Introduction
S
MSCs are also capable of differentiating to multiple specific types of cells such those in bone or cartilage,14,15 and implantation of MSCs may overcome the problems of the organ shortage crisis. MSCs also have strong immunoregulatory and immunosuppressive effects, which support the use of MSCs in allogeneic transplantation.16,17 Implantation of allogeneic MSCs can avoid the graft versus host diseases (GvHD), which are often observed in recipients after allogeneic organ transplantation.18,19
To achieve the large numbers of MSCs required for clinical applications, the cells either need to be expanded in culture, or MSCs from multiple donors must be pooled. In either case, a method for long-term storage of the cells is required for off-the-shelf availability. 20 Cryopreservation is currently the only method to preserve cells, including MSCs, for any considerable period. Cryopreservation maintains cell functional properties and allows pooling of cells to reach the cell numbers required for clinical application. 21 Without cryopreservation, cells have to be continuously subcultured, which may accumulate genetic changes, resulting in heterogeneity or tumorigenicity.22,23
At −196°C (i.e., in liquid nitrogen), cells have no metabolic demands, thus avoiding biological variation due to genetic drift even when stored for multiple years. Further, cells are protected from infection while cryopreserved. 24 Therefore, cryopreservation provides cells with their specific genetic characteristics and intact function at specific passages for clinical and research purposes. 23 The modern technique of cryopreservation allows the long-term storage of living cells and tissues that offer a great potential for clinical applications, including bone marrow transplantation, 25 bone grafts, 26 blood transfusion, 27 bone marrow transplantation, 25 and in vitro fertilization. 28 Although preclinical studies have shown that implantation of cryopreserved MSCs is capable of restoring myocardial function 29 and treat intestinal inflammation, 30 the use of cryopreserved MSCs in clinical applications is still not well established.
Various methods have been developed for cryopreservation of MSCs, such as slow freezing and vitrification. However, these methods have their limitations. First, MSCs preserved with these methods still have the risk of cryo-injury even though cryoprotective agents (CPAs) are involved in protecting the cells against cryo-injury. 31 Second, CPAs such as DMSO may induce undesired differentiation of MSCs to neuron-like cells. 32 To address these issues, optimization of CPA use or the development of new cryopreservation methods is required.
Most recently, with advances in the micro/nano technologies, it is possible to improve the efficiency of cryopreservation while overcoming the limitations of existing cryopreservation methods. Freezing cells encapsulated in nanoliter droplets on highly hydrophobic nano-rough surfaces and the development of nontoxic nanoscale bio-inspired CPAs are the promising advances in cryopreservation. 33 But for now, MSCs can only be routinely cryopreserved with the existing methods.
There are some existing reviews on cryopreservation of stem cells.34–37 However, this review focuses not only on the important parameters for MSCs cryopreservation, but also discusses the limitations of the existing cryopreservation methods and the challenges to be addressed in order to preserve MSCs effectively for clinical applications.
Important Parameters for Cryopreservation of MSCs
Compared to cryopreservation of specialized cells such as osteoblasts and chondrocytes, more parameters need to be evaluated for cryopreservation of MSCs. For instance, it is important to assess the immunomodulatory and multilineage differentiation ability of MSCs after cryopreservation on top of cell viability and phenotype, which are important in cryopreservation of the specialized cells. If the immunomodulatory and differentiation ability are compromised during the cryopreservation process, MSCs might not be able to suppress the transplant rejection and differentiate into other types of cells to aid in regeneration and repair of damaged organs.
Moreover, information regarding the biosafety of cryopreserved MSCs is still not well established. After cryopreservation, stem cells might run the risk of undergoing genetic instability that may affect cellular proliferation and differentiation, eventually leading to tumorigenesis. 38 It has been suggested that tumorigenicity of stem cells might be caused by CPAs during cryopreservation (e.g., DMSO has the potential to induce genetic instability 39 ), whereas the biosafety of other CPAs has not yet been well established. 38 Therefore, the assessment of the biosafety of cryopreserved MSCs in terms of genetic stability and tumorigenic potential is essential prior to clinical applications. Furthermore, the assessment of homing/engraftment potential of cryopreserved MSCs has been explored recently.
Immunomodulatory ability
MSCs hold great potential for use within immunomodulatory therapies (e.g., GvHD) and allogeneic transplantation.17,19 They have the ability to secrete immunosuppressive molecules (e.g., interleukin-4 (IL-4) and IL-10) to inhibit the activation of immune cells (e.g., dendritic cells and lymphocytes), thus preventing autoimmune activities and inflammation.40,41 To evaluate the use of cryopreserved MSCs in these applications, their immunomodulatory ability is determined by the immunosuppressive effect on lymphocytes or peripheral blood mononuclear cells (PBMCs).42–46 It has been reported that cryopreservation does not affect the ability of MSCs to suppress the proliferation of lymphocytes or PBMCs.42,45,46 However, Francois et al. 43 and Moll et al. 44 suggested a potential impairment of cryopreserved MSC immunosuppressive phenotype directly after thawing, which is associated with the activation of heat-shock proteins (e.g., Hsp 27, Hsp 47, Hsp 56, and Hsp 90) that initiate a heat-shock stress on MSCs during the thawing process. 43 Moreover, the loss of viability observed in both studies also directly affects the immunomodulation capacity of MSCs. 43 The difference in viability observed in the respective studies may be due to the different methods of cultivation and freezing used. 45
Interestingly, the immunosuppressive effect of cryopreserved MSCs on lymphocytes or PBMCs could be restored to levels comparable to fresh MSCs after post-thaw culture for a short duration (fewer than 7 days).43,44 These results imply that cryopreservation negatively affects the immunomodulatory properties of MSCs in a reversible manner, 43 and the therapeutic effects of cryopreserved MSCs should be recovered in culture prior to clinical applications. Future studies should aim to improve the therapeutic efficacy and delivery mode of cryopreserved MSCs for efficient clinical applications. 44
Cell differentiation capacity
Stemness markers such as Nanog, Rex-1, Sox-2, and Oct-4 have been used to analyze the multipotency of stem cells.47,48 Studies have shown that the reduction of MSCs differentiation capacity was associated with the decreased expression level of those markers.48,49 Therefore, stemness markers should be evaluated as they might be affected by cryopreservation and thus compromise the differentiation ability of stem cells. Angelo et al. 12 and Janz Fde et al. 50 have shown that MSCs are capable of retaining their differentiation ability by maintaining the stemness markers (e.g., Nanog, Sox-2, and Oct-4) level.
The differentiation of MSCs into specific cell types such as adipocytes, osteocytes, and chondrocytes has been assessed by histochemical staining and gene expression studies. The presence of round lipid droplets stained by Oil Red O was observed after cryopreserved MSCs were induced to differentiate into adipogenic-like cells.10,12,51–53 These adipogenic-like cells expressed adipogenic markers such as lipoprotein lipase and peroxisome proliferator-activated receptor-γ (PPAR-γ).50,51
To assess the osteogenic potential of cryopreserved MSCs, the presence of calcium deposition after osteogenic induction of cryopreserved MSCs was confirmed by Alizarin Red or Von Kossa staining.10,13,51,53,54 These osteogenic-like cells showed a high expression level of osteogenic markers such as osteocalcin (OSC) and alkaline phosphatase (ALP).51,54 The presence of proteoglycan after chondrogenic induction of cryopreserved MSCs was confirmed by Alcian Blue or Safranin O staining.10,12,51,55 These chondrogenic-like cells expressed chondrogenic markers such as collagen type II. 50
Taken together, although the stemness profiles of cryopreserved MSCs have not been evaluated in most of the studies, existing evidence has not shown a significant effect of cryopreservation on the MSC differentiation ability, especially in term of adipogenic, osteogenic, and chondrogenic differentiation. On the contrary, James et al. 56 reported that adipose-derived MSCs preserved in 10% DMSO and 90% fetal bovine serum (FBS) displayed low adipogenic and osteogenic potential when compared to fresh cells, by downregulating the expression of adipogenic and osteogenic genes. Therefore, it is essential to determine and compare the effects of cryopreservation on gene expression of differentiation capacity and stemness among MSCs preserved in various CPAs, to provide insight into molecular changes that may occur following cell freezing 20 .
Cell viability
To achieve an adequate therapeutic effect from immediately applied cryopreserved MSCs, it is very important to evaluate the cell viability. CPAs are essential to maintain the cell viability when the cells are stored at −196°C. 57 Viability assays such as trypan blue exclusion, annexin V-propidium iodide (annexin V-PI), and live-dead cell staining (e.g., acetomethoxy derivate of calcein (calcein-AM)/ethidium bromide) assays, have been used to evaluate the viability of MSCs after cryopreservation. These assays consistently indicate that DMSO (≤10%) gives a high cell viability of MSCs (>75%) following cryopreservation.7,8,50,58
In general, cell viability is affected by different types and concentrations of CPAs used in the cryopreservation process. A comparison study on cell viability of amnion-derived MSCs preserved in various types of CPAs showed that DMSO gives a higher cell viability (>80%) than glycerol (70%–80%) or nonpermeating CPAs such as trehalose (30%–40%) and sucrose (20%–30%), 50 indicating the relatively high efficiency of DMSO in maintaining the survival rate of MSCs throughout the freezing and thawing process.
Cell phenotype and proliferation capacity
The cell phenotype of MSCs can be determined through their morphology and surface marker (CD marker) expression. Morphologically, MSCs have spindle or fibroblast-like shapes.59,60 It has been reported that there were no morphological changes to MSCs after cryopreservation.9,53,61 MSCs are positive for mesenchymal-associated markers such as CD90, CD105, and CD73, while they lack hematopoietic associated markers such as CD34, CD19 CD45, CD14, and HLA DRDPDQ.62,63 After cryopreservation, MSCs retained a similar expression level of positive and negative CD markers.7,50,53–55,61 Overall, existing evidence shows that cryopreservation has no significant effect on phenotype of MSCs.
The proliferation capacity of MSCs can be determined through their growth kinetics. Growth kinetics can be analyzed by calculating population doubling time.64,65 It has been reported that population doubling time was similar between cryopreserved and noncryopreserved MSCs from various adult tissues.9,55,61 These results indicate that MSCs are capable of maintaining their proliferative potential after cryopreservation.
Biosafety (genetic stability and tumorigenicity)
To determine whether stem cells are safe to be used in clinical applications, potential risks of the stem cells must be assessed through the analytical assessment of the product characteristics, animal studies and nonclinical safety assessment. 66 A failure from insufficient safety assessment resulting in tumor formation or life threatening graft rejection, indicates that they are not safe to be used in clinical applications. 67 Because genetic aberrations have been strongly associated with cancers, it is important that cell preparations for clinical use are free from cancer-associated genomic alterations, and this requires defined culture conditions and the genetic characterization of the final clinical product.22,68
According to Diaferia et al., 38 a cryopreservation process involving DMSO has the potential to modify the cell cycle and chromosome stability of stem cells and lead to alteration of cell functions that might eventually result in tumorigenesis. As chromosomal aberrations are hallmarks of human cancer, 69 it is very important to analyze the total choromosomal content of cells through karyotyping prior to clinical applications. Karyotyping allows the detection of aneuploidy (loss and gain of chromosomes) and chromosomal anomalies like inversions, depletions, translocation and duplications, which are frequently observed in genetic diseases. 70 The cytogenetic status of cryopreserved MSCs has been determined in previous studies using the karyotyping method, which demonstrated that cryopreservation did not alter chromosomes' numbers and structures in MSCs.12,45,46,51
Tumorigenesis can also be induced through epigenetic changes to cellular function. 71 Both DNA methylation and histone modification are among mechanisms that cause such changes. 72 DMSO is likely to affect these epigenetic changes on cellular functions, particularly proliferation and differentiation of stem cells. 39 The effect of other CPAs on epigenetic changes has not yet been explored. 38 These epigenetic changes cannot be detected by the karyotyping method. Therefore, the tumorigenic potential of cryopreserved MSCs should be further evaluated through tumorigenic assessment such as DNA damage, and expression levels of both tumor suppressor genes and oncogenes. These concerns have further strengthened the need for more thorough biosafety evaluation of cryopreserved MSCs. In addition, biosafety comparison studies among various types of CPAs are needed to determine the most suitable CPA use for clinical therapy.
Homing/engraftment potential
The homing/engraftment of MSCs is the process by which cells migrate, engraft, and exert local functional effects (e.g., immunosuppresion). 73 For example, upon sensing an injury signal, MSCs will migrate to areas of inflammation and suppress the inflammation process. 74 . However, Chinnadurai et al. 75 showed that cryopreservation reduces the homing/engraftment potential of MSCs, indicated by poor binding to the extracellular matrix (e.g., fibronectin) and human endothelial cells compared to fresh MSCs. This reduction is associated with a reduced cytoskeletal F-actin content in cryopreserved MSCs. The critical process that led to the change in F-actin content was the freezing process. 76 To date, the impact of cryopreservation on homing/engraftment potential of MSCs has not been fully evaluated, and therefore should be further explored.
Cryopreservation Methods for MSCs
There are two main methods of cryopreservation: 1) slow freezing and 2) rapid freezing/vitrification. Both methods have their advantages and disadvantages (Table 1) when it comes to MSC cryopreservation. The limitations of the existing cryopreservation methods should be addressed to ensure cryopreservation efficiency.
CPAs, Cryoprotective agents.
Apart from freezing, optimizing the thawing method of frozen MSCs is also important. To date, the standard method of thawing frozen MSCs (either from slow freezing or vitrification) is to warm them rapidly (>100°C/min) in a water bath at 37°C until all ice crystals disappear. 35 This method generally results in high post-thaw recovery of viable cells without using high-cost equipment.
However, due to the potential contamination of the water-bath with microorganisms, it might be safer to thaw cell suspensions using a dry warming procedure. 77 To achieve this, frozen MSCs can be thawed at 10°C/min in a controlled-rate freezing/thawing chamber. This method has resulted in high post-thaw viability of MSCs comparable to those thawed with the standard method. 78 The development of a low-cost, reliable, and controlled-rate dry warming device for thawing frozen MSCs is essential for efficient clinical applications.
After thawing, MSCs are washed by centrifugation prior to clinical applications to remove the CPAs, especially those which are toxic (e.g., DMSO). However, this method has resulted in cell loss that might affect the clinical outcome. Therefore, the development of methods to remove CPAs while minimizing cell loss would benefit all recipients of cryopreserved MSC transplants. 37
Slow freezing
The slow freezing method is preferable for MSC cryopreservation in clinics and research laboratories, due to the low risk of contamination and easier processing. 33 With a freezing rate of 1°C/min, a large number of MSCs can be easily frozen in one vial with the required CPA at low concentrations (<1.5 M). 79 Further, there is no direct contact between cells and nonsterile liquid nitrogen during the freezing process, significantly reducing the potential risk of contamination. Initially, MSCs loaded with CPAs were frozen using a nonprogrammable time freezing protocol in a −20°C freezer or freezing device called “Mr. Frosty” that produces a freezing rate of 1°C/min. To improve cryopreservation efficiency, a programmable freezing time protocol was developed using a high-cost controlled-rate freezer. However, a comparison study showed that either of these protocols can be used to freeze human MSCs without affecting their viability, phenotypes, and functional properties. 50
With an advance in technology, a programmed freezer with alternating magnetic field and electric field called the ‘Cell Alive System’ (CAS) has been introduced. The principle of this system is to prevent the formation of ice by vibrating the cells and water molecules during freezing with a nonthermal mechanism. 80 This can further reduce the risk of freeze injury to MSCs. 81 To date, the nonprogrammable freezing time protocol is still the preferable protocol for MSC cryopreservation due to its high cryopreservation efficiency and low cost. Optimization of the use of CPA is the only remaining challenge to be addressed in order to preserve MSCs effectively using slow freezing method. Xeno-free 5% DMSO was reported to be an ideal CPA to preserve MSCs for clinical applications, after this approach was accurately compared with other CPAs in terms of preserving the viability, phenotype, and functional properties of MSCs in a quantitative manner. 82
Limitations of slow freezing
Slow freezing involves issues related to a higher risk of freeze injury (e.g., cell death) due to the formation of intra- and extracellular ice during the freezing process.83,84 To address this issue, optimization of the use of CPA is very important to avoid ice crystal formation by loading the MSCs with the optimum concentration of suitable CPAs (Fig. 1). DMSO with a concentration of 10% (v/v) combined with FBS (20%–90%) (v/v) is often used to preserve MSCs.13,51,56,61 DMSO can penetrate cells and remove water from them, thus preventing intracellular ice formation and cell rupture. 34
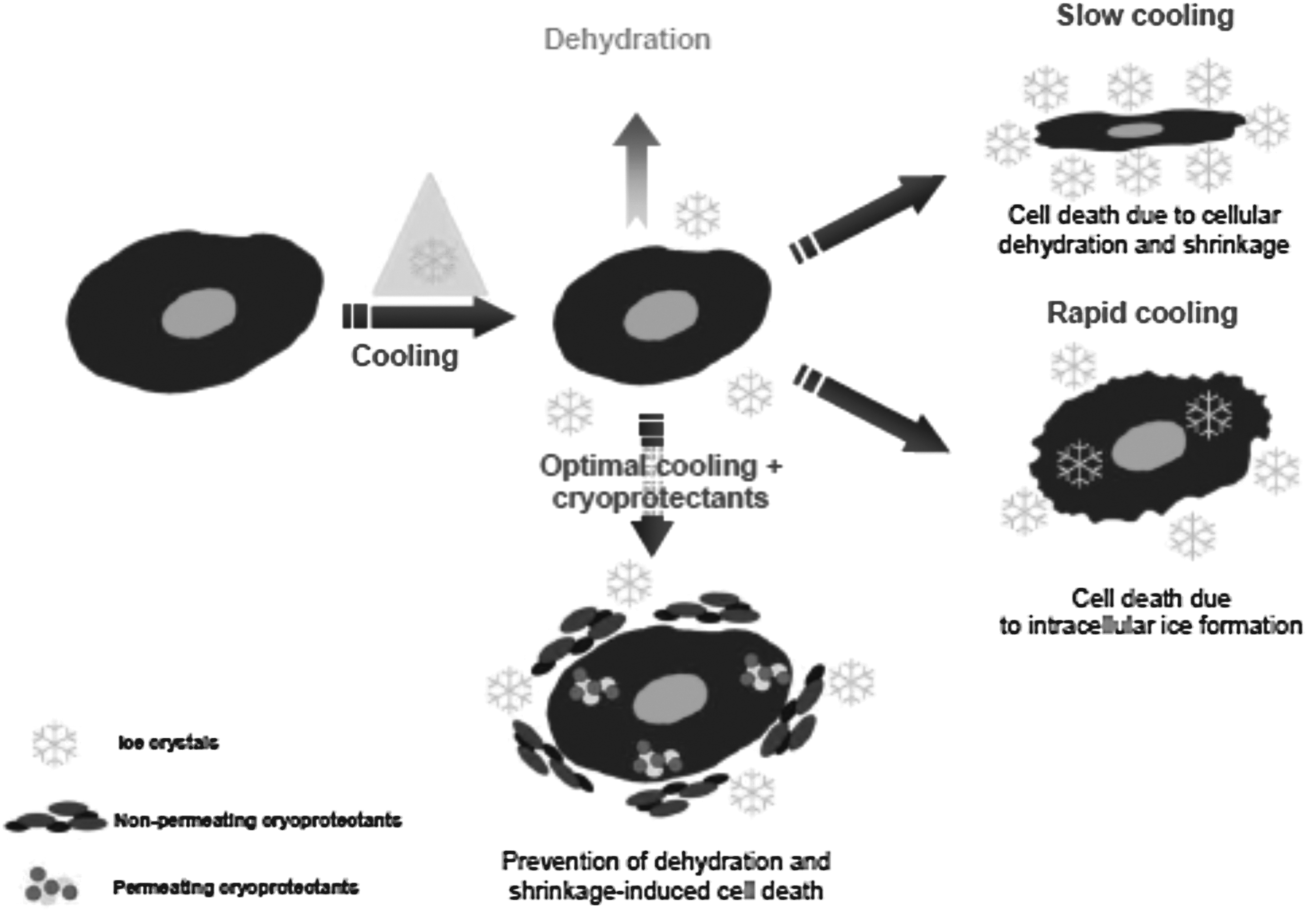
Mechanisms of cell injury during cryopreservation process. An optimal concentration of suitable CPAs should be added to cell suspensions to avoid such injury. Reproduced with permission from Martin-Ibanez et al. 84
However, DMSO is cytotoxic at temperatures beyond 4°C. 85 It is essential to reduce the toxicity by removing the DMSO from cryopreserved cells prior to clinical use, but the total removal of DMSO is complex and time consuming. 35 This has resulted in the need for development of an alternative cryopreservation medium or a cryopreservation medium consisting of low concentration of DMSO. 86 In general, FBS is routinely added to stabilize the cell membranes and adjust intra- and extracellular osmotic pressure, thus maintaining the survival rate of cells. However, the use of FBS in cryopreservation media should be minimized due to its potential to trigger a xenogeneic immune response or transmit pathogens to the recipient.85,87
Challenges of overcoming the limitations of slow freezing
The introduction of nontoxic disaccharides such as trehalose, and hydrophilic macromolecules such as polyvinylpyrollidone as a CPA, has the potential to replace the use of DMSO.50,52 These CPAs cannot move across the cell membrane but are able to protect the cells from rupture by forming a viscous glassy shell around the outer surface of the cell. 57 However, they are less efficient than DMSO in terms of maintaining the survival rate of MSCs. Therefore, the alternative CPAs or CPA cocktails used to replace DMSO completely will require further investigation.
To replace the use of FBS, xeno-free cryomedium (e.g., sericin and 5% human albumin solution plus 5% DMSO)10,88 have been proposed. Moreover, our recent study also demonstrates that adipose-derived MSCs preserved in cryomedium containing only 5% DMSO were able to maintain their phenotype, stemness, proliferative and differentiation potential, and high cell viability in a way comparable to 10% DMSO. 82 These results indicate that xeno-free 5% DMSO may be an ideal CPA to preserve MSCs effectively for clinical applications. However, further investigation is needed to evaluate its effect on the biosafety of MSCs.
Vitrification
Vitrification is a process by which cell suspensions are transformed directly from the aqueous phase to a glass state, after direct exposure to liquid nitrogen. 89 Two such approaches have been used to preserve cells. One of the approaches has been termed equilibrium vitrification. This approach requires both formulation of multimolar CPA mixtures and their introduction to the cell suspensions in a stepwise fashion, to help lower chemical toxicity before the cells were flash frozen with liquid nitrogen. However, this approach has the risk of inflicting osmotic damage on the cells. 36 So far, only human amnion-derived MSCs have been preserved with vitrification using this approach, and the results showed that vitrification does not affect the phenotype and functional properties of MSCs. 90
An alternative approach is nonequilibrium vitrification, which employs extremely high freezing rates in conjunction with one lower concentrations of CPA mixture for preserving the cells. 36 In this approach, vitrification systems are divided into carrier-based systems and carrier-free systems (Fig. 2). Various types of carrier for vitrification, such as straws, quartz microcapillaries, and cryoloops have been developed to achieve a high freezing rate and to prevent the cells from cryo-injury.
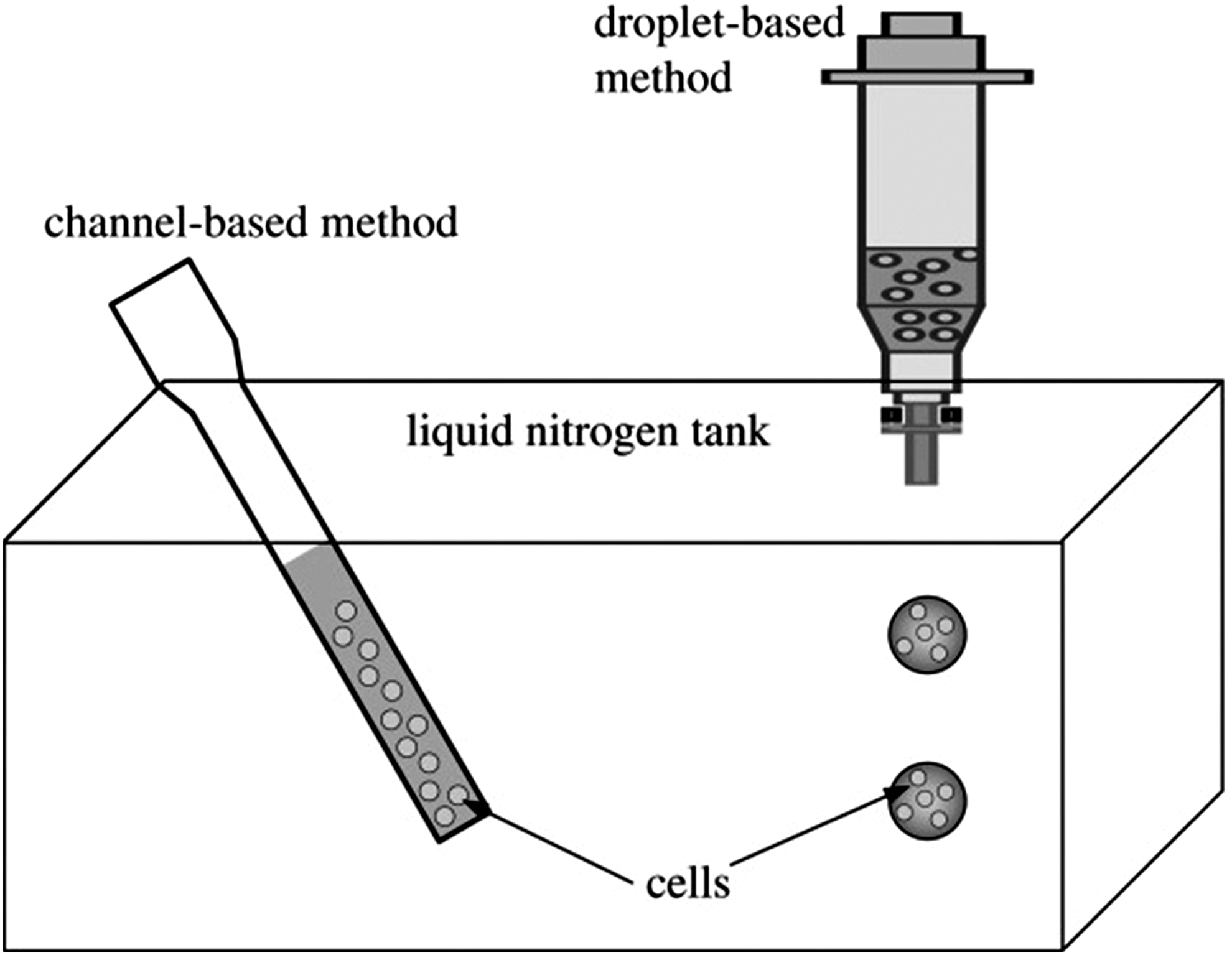
Carrier-based (channel-based) and carrier-free (droplet-based) methods for vitrification. In carrier-based methods, CPAs are mixed with cells in a carrier (e.g., straw and capillary). Then the cell-loaded carrier is immersed in liquid nitrogen for freezing. In carrier-free methods, cell-loaded droplets premixed with CPAs are ejected into liquid nitrogen for freezing. Direct contact of cells with liquid nitrogen is required in both methods in order to preserve cells effectively. Adapted from Xu et al. 98
Each carrier system offers a different freezing rate. Plastic straws were the initial carrier used for vitrification, but only provide a freezing rate at 2500°C/min. Quartz microcapillaries, which provide a higher freezing rate of 250,000°C/min were developed, followed by cryoloops offering a freezing rate as high as 700,000°C/min. 79 The use of higher freezing/thawing rates permits vitrification using lower CPA concentrations, thereby reducing the potential for CPA toxicity and osmotic damage. To achieve a higher freezing rate, microscale (nanoliter) droplet vitrification systems (carrier-free systems) that involve generation of cell encapsulating CPA droplets, followed by direct injection into liquid nitrogen, have been developed. 79 To date, MSCs have not been preserved using nonequilibrium vitrification.
Limitations of vitrification
Vitrification carrier systems generally need manual handling with great manipulation skills, leading to a low throughput process. The approach only fits well with cryopreservation of cells in small volumes such as oocytes 91 but not with MSCs in large volumes. Further, vitrification requires a high concentration of CPAs (6–8 M), which have the potential to cause chemical toxicity and osmotic shock to cells. 79 Moreover, vitrification might also lead to potential MSCs contamination with pathogenic agents, due to the direct exposure of the cell suspensions to nonsterile liquid nitrogen. Liquid nitrogen has been reported to have the issues of potential contamination with pathogens such as Aspergillus sp. and Hepatitis B virus.92,93 The contamination may come from cross-contamination from infected samples in the storage tank or nonsterile liquid nitrogen itself. 94
Challenges of overcoming the limitations of vitrification
Several attempts have been carried out to improve the efficiency of vitrification, which include the stepwise addition of CPA in small volumes with a microfluidic device to minimize osmotic shock, and the development of ejector-based microscale (nanolitre) droplet generation systems for vitrification of cells at high throughput.95,96 The microdroplets of cell suspensions loaded with CPA can achieve a higher freezing rate than carrier-based systems and so minimize osmotic shock. Moreover, as the carrier-free systems allow efficient vitrification of droplets in a continuous manner, throughput capability has been significantly improved to the levels required for MSC cryopreservation. However, the recycling of the cells is labor-consuming as individual cell colonies need to be selected manually.79,83
To date, the risk of contamination with pathogens should be reduced for the potential clinical use of vitrified MSCs. Given the prior concerns, the development of a sterile, closed, fully automated and high throughput system that allows MSCs to be vitrified without any direct exposure to liquid nitrogen is required. 33 For future clinical applications, liquid nitrogen and ejection-based droplet generation systems must be sterilized and operated in sterile hoods. Liquid nitrogen can be sterilized by using ultraviolet radiation or sterile polyetrafluoroethylene cartridge filteration. 97
Conclusions and Future Perspectives
It is essential to have a good cryopreservation protocol in order to preserve MSCs effectively for clinical applications. The protocol must be capable of maintaining the functional properties (e.g., immunomodulatory and differentiation ability) and survival rate of MSCs. There are many issues and challenges that need to be addressed concerning existing MSCs cryopreservation protocols. First, cryopreservation protocols (e.g., types and concentrations of CPAs) should be optimized to decrease the risk of harmful effects on MSCs. For instance, the heat transfer modeling suggested by Xu et al. 98 can be applied to optimize the current protocols in order to minimize freeze injury to MSCs due to osmotic shock.
Second, MSCs should be preserved without direct exposure to liquid nitrogen, to reduce the risk of pathogenic contamination. In addition, biosafety assessments of cryopreserved MSCs are necessary to ensure the safe use of the cells prior to clinical applications. Last but not least, the development of a sterile, closed, fully automated and high throughput system for MSC cryopreservation is required for clinical applications in the near future. Overcoming these challenges would establish the standardized cryopreservation protocol of human MSCs for future clinical applications.
Footnotes
Acknowledgments
This study was supported by University of Malaya, High Impact Research Grant (UM.C/HIR/MOHE/ENG/44) and Postgraduate Research Grant (PPP) (PG007-2014A) from the Ministry of Higher Education Malaysia. FX was partially supported by the Major International Joint Research Program of China (11120101002), the National Natural Science Foundation of China (11372243), the International Science and Technology Cooperation Program of China (2013DFG02930), and the National 111 Project of China (B06024).
Author Disclosure Statement
All authors declare no financial conflict of interest.