
Abstract
Background:
Conducting high throughput -omics research requires high quality, data-rich biospecimens to unravel factors underlying childhood cancers; this is an extra burden in a limited resources country. For this purpose, Children's Cancer Hospital (CCHE), the largest pediatric cancer hospital worldwide, established a cutting-edge Biorepository and Biospecimen Research Facility (CCHE-BBR).
Objective:
To present a step-by-step guide to establishing a hospital-based biorepository with limited resources, and working in collaboration with different hospital facilities to supply the research community with high quality data-rich biospecimens fit for a wide range of research purposes. This approach will foster research in the era of personalized precision medicine.
Methods:
CCHE-IRB approved the collection and storage of biospecimens from patients and parents for future research. We focused on staff training, recruiting qualified scientists, and establishing the infrastructure. The CCHE Biorepository developed strict standardized procedures for sample acquisition, processing, annotation, storage, and distribution based on ISBER Best Practices and CAP-accreditation guidelines. We collect samples at different clinical time points (e.g., at remission and/or relapse) as well as parents' samples for genetic studies. Using CaTissue®, an electronic storage management system, allowed sample annotation and full integration with clinical data and the cancer registry.
Results:
In 2 years, we succeeded in establishing a well-designed biorepository within our regulations, bylaws, and SOPs, and with a minimal budget. We store high quality blood derivatives, CSF, and malignant/normal tissue samples.
Conclusion:
Building a high quality biorepository with minimal-resources to encourage research is possible. Having the suitable infrastructure with a significant number of clinically annotated samples can play a major role in international research projects, sharing samples and/or data with other groups.
Introduction
C
This led to their under-representation in projects such as HapMap, with the result that there are no available genomic data to detect biological differences and provide different treatment responses in this population. With the rapid evolution of technology, and the increase in biomedical research aimed at developing personalized medicine, this in turn, will require a supply of high quality clinically annotated biospecimens fit-for-all research. Hence, having a biorepository to standardize procedures supported by evidence-based science for all sample procurement, processing, storage, and distribution processes is a basic requirement.
CCHE-BBR as a state-of-art facility in a limited resource setting
Children's Cancer Hospital-57357-Egypt (CCHE) is a non-governmental hospital that aims to provide the highest level of care for children with cancer, at no charge. It is the largest specialized pediatric oncology center of its kind worldwide. In 2008, CCHE established the Research Department, whose mission is to conduct, facilitate, and support innovative quality research integrated into all hospital activities.
Faced with many challenges, we succeeded in paving the way for pediatric cancer research at CCHE by offering improved access to information and accurate, reliable data. Now researchers have instant access to patient information whenever they need it. The Research Department hosts the online secure and reliable system applications for data management, as well as the cancer registry.
For decades, banking of samples was done by investigators for their own research interests. Recently, there have been persistent efforts to define and standardize the science of biobanking, when it became clear that there is an increasing demand among institutions for a centralized biobank as a core facility. The International Society for Biological and Environmental Repositories (ISBER), the National Cancer Institute (NCI), and other organizations have published evidence-based best practices for collection and storage of human biospecimens. 2 Biospecimen research is a rapidly growing field of research.
The Research Department decided to establish a CCHE Biorepository and Biospecimen Research Facility (CCHE-BBR) that contains biospecimens linked to accurate and reliable clinical, pathological, and epidemiological data. CCHE-BBR is a precious resource for pediatric cancer research requiring high quality data-rich samples that are fit-for-all research. The vision is to establish CCHE-BBR to be one of our shared core facilities. The mission is to procure, process, and store high quality biospecimens, linking them with clinical data.
With this publication, we present a step-by-step guide for the establishment phases of our CCHE-BBR.
Methods
Phase I: Planning
CCHE Biorepository and Biospecimen Research Facility (CCHE-BBR)
Governance
CCHE-BBR is governed by the Research Department and the Vice President for Research, Outreach and Academic Affairs. The Institutional Review Board (IRB) ensures the adherence to ethical commitments. A Biorepository Coordinating Committee (BCC) provides the approvals of sample release. A Scientific Medical Advisory Committee (SMAC) governs the scientific aspects of sample release (Fig. 1).
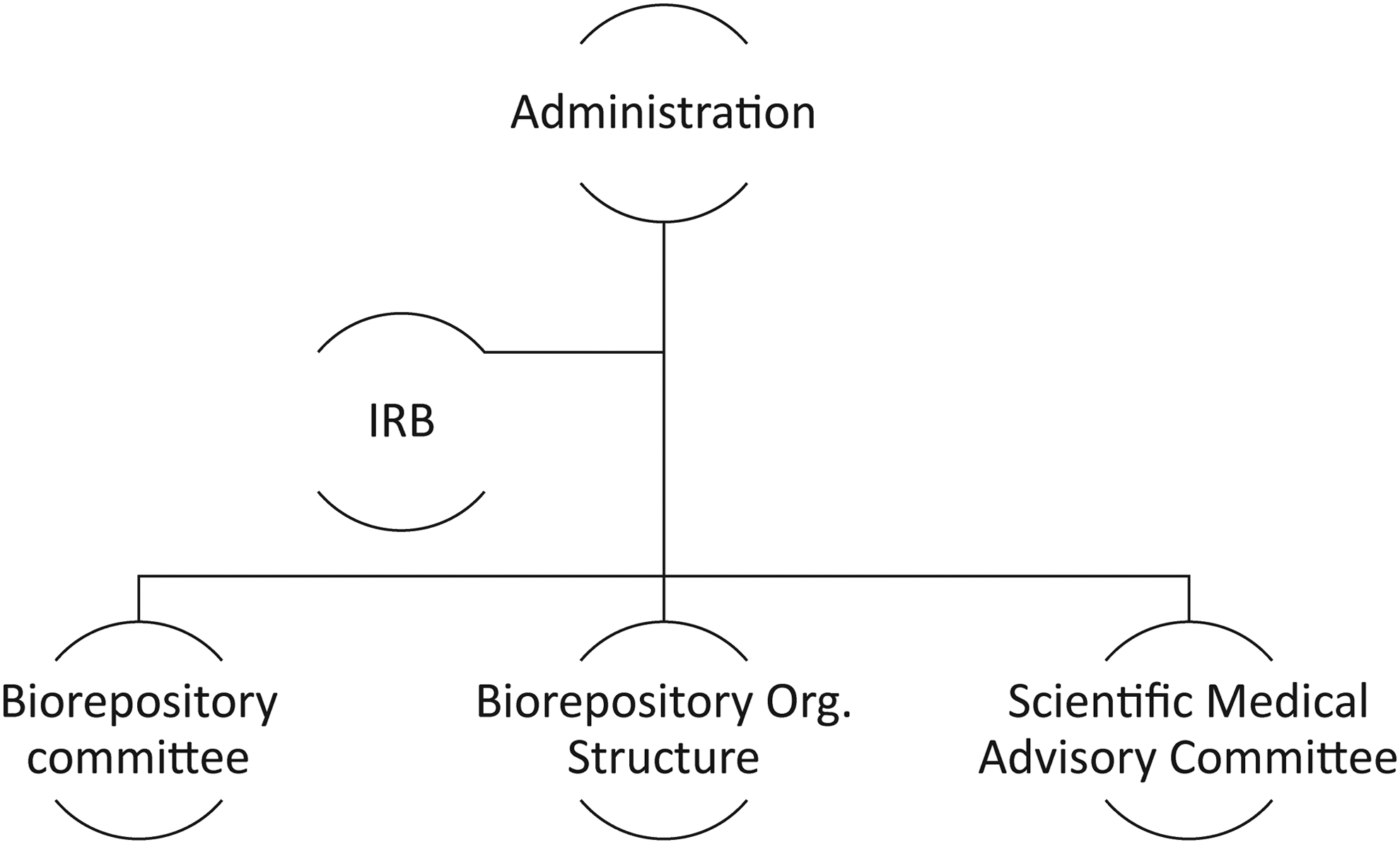
CCHE-BBR governance structure.
Composition
For establishing CCHE-BBR, professors from the stakeholder departments of research, surgical pathology, clinical pathology, surgery, pediatric oncology, radiotherapy, and IT were appointed to a BCC. It is composed of 8–10 voting members selected based on their research experience to provide a broad base of clinical, basic, ethical, and IT research expertise.
Biobank model
The BCC decided that CCHE-BBR model will be a cancer-oriented trios biobank collecting samples from children and their parents.
Responsibilities
The BCC is responsible for organizing the projects at CCHE-BBR. It is responsible for approving standard operating procedures (SOPs) implemented at CCHE-BBR and will have auditing authority. This Committee will ensure that good laboratory practices (GLP) are followed in every step involved with sample collection, processing, storage, and retrieval. The Committee showed a collaborative spirit interacting in harmony with our workflow ensuring support, yet distinction between samples for the biorepository and the clinical care setting, thus preventing overlap with patient care.
Ethical, legal, and social implications
The CCHE-BBR consent form permits the banking of body fluids and leftover tissue that is not required for diagnosis, as well as developing cell lines from these samples. Considering the Egyptian law, it was found that a child's parent/first-degree guardian is the only responsible party for signing any legal document until the age of 18.
Challenges
Research in developing countries is facing many ethical challenges in sample collection that may be due to:
• Lack of research culture in the community, • Religion-based misconceptions • Level of public trust and fear of being abused • Parents' educational level • Patient privacy and sample coding as explained in IT section
These factors may play a major role in the rate of participation. Other challenges appear when there is need for multiple time point collection, and collection of surgical samples, where patients may tend to withdraw out of fear.
Action
To ensure that all regulations are met, a simple, concise and informative consent form was designed and written in native Arabic as well as in English. This consent addresses, in the form of a questionnaire, all aspects of the project such as risks, advantages, and the right to withdraw at any time. The consent form passed through a long process in order to ensure that it covers all the necessary ethical aspects,3–5 starting with the approval of the committee, followed by the IRB approval, which is renewed annually.
Our goal was to identify the ELSI barriers and overcome them. A survey was designed to include and analyze the socioeconomic and educational level of parents/guardians regardless of whether they accept or refuse to participate. This survey included some personal information regarding their educational and financial levels for further possible epidemiological studies, as well as possible reasons of refusal. This survey data will be analyzed and published, including the results where we found that patients were very trusting of the hospital and its staff due to the clinical quality of care they are offered, so they did not fear being abused. Yet, there were some psychological reasons that were correlated with the refusal rate (3.9%), as well as with withdrawal from participation.
Logistics (Space design and infrastructure)
The aim was to design the space allocated for the biobank efficiently, purchase required equipment, and hire personnel and train them to adhere to the best standards. The challenges were:
• A well-equipped space; • Electrical emergencies and security; • Patient's and sample data safety; • A secure, limited controlled-access database;
6
• Personnel and training.
Space design
A space that was close to the blood drawing facility and the surgery/pathology theater was chosen. The area was divided into five sections: sample receiving area, sample processing area, an office for all documentation, next to a storage area containing the freezers and liquid nitrogen, as well as area for quality control and biospecimen research (Fig. 2).
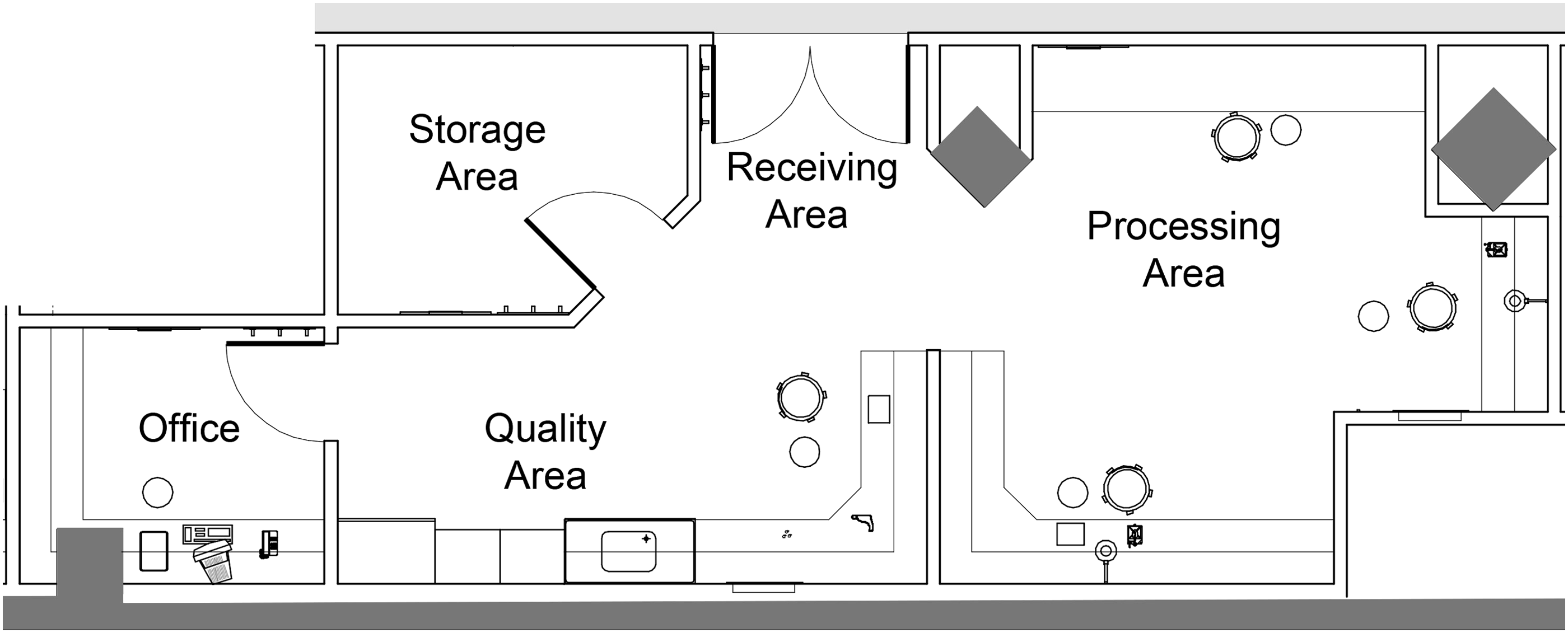
CCHE-BBR space design.
Electrical power
Electrical power is ensured through CCHE's emergency power system. A generator enabling our infrastructure to be self-sufficient in power for at least 7 days during an electrical emergency is connected to all storage equipment. A 24/7 system operates for remote surveillance of temperature.
Equipment
Due to limited funding, basic equipment was purchased with the intention to increase when needed, as shown in Table 1.
Security and alarm systems
We have a policy that guarantees controlled access with video surveillance as well as a fire alarm system. A remote alarm system is connected to all freezers, which can dial up to 4 numbers if there are any fluctuations in freezer temperature and/or room temperature.
Patient data safety
To protect the privacy of participants who donate their samples for research, all measures were taken to ensure security of data and prevent any misuse or unethical practices. Patients' samples are de-identified and coded with a secure unique ID, which is only accessible by CCHE-BBR staff.
Software
During the system design phase, many elements governed choosing the software, including need for a web-based central solution, flexibility and variability of the properties of the banking freezer slots, need for sample tracking, integration with other software, keeping certain information about samples and samples relations to each other, and the future expandability with the presence of a supportive IT community.
We reviewed the best available commercial and open source solutions by examining their prerequisites, scalability, and interoperability. For 2–3 months, we tested the deployment of the last freely available stable release of software packages. We chose caTissue® that was developed by the US NCI to serve as a next-generation tissue banking application). 7 We first used the software in a virtual environment, then we placed an installation on a virtual private server (VPS). After a soft-run period of 6 months for testing its components and the backup workflow, we deployedthe software on a PC of Intel ® Core™ i5-2400 CPU @3.10 GHz, 6.00 GB install memory (RAM) and Windows 7 (64-bit) operating system.
We translated the first protocol and workflow for procurement procedures, preparation, and storage of biospecimens to electronic orders. We designed and implemented a backup solution that ensures the coverage of day-to-day activities, and distributed the backup images on reliable geographically distant servers, including a backup server in Cairo, another server in UK, and Amazon® S3™ service in the east coast, USA. We customized the caTissue® code to integrate multiple elements in sample ID directly from the protocol template in caTissue® and created a custom automated ID that represents the type of sample and number. The initiation phase did not require extra costs for personnel, or software costs.
Later, we developed an inheritance (to describe familial relations between samples) module inside caTissue®, which was developed by a commercial software company. Clinical reports from Cerner ® Millennium™ (EMR) Power Forms are extracted via SAP ® BusinessObjects InfoView™. Process Integration with clinical research software/cancer registry will be implemented.
Labeling
For sample tracking, we created our labeling system as shown in Table 2 and Figure 3. The labels are of high-quality adhesive type, avoiding handwritten labels and providing human-readable and barcode formatting of unique IDs on each specimen. 2

CCHE-BBR label system. 4_838: patient cat_ID is 838 in protocol 4. WB2013S1 is whole blood as parent sample collected in 2013 as first sample. A1, aliquot 1; SE, serum.
Personnel and training
An interviewer was hired for the task of consenting participants. A secretary was assigned the extra task of tracking the consent forms. A laboratory worker was hired for the biobank, and a senior person from the research department coordinated and established the biobank. A year after operation, the team consisted of a manager, two full-time lab persons, two full-time interviewers, and one dedicated secretary. Full-scale training was offered to the biobank coordinator at the Luxembourg biobank. Interviewers were given both ethics and communication training.
Pre-Phase II: Challenges
To formulate our SOPs, we had issues to resolve:
• Should we start according to sample type (e.g., blood) in all cancer subtypes or should we start according to disease category (e.g, hematology) and collect all samples types? Should we start with initial samples and then start collecting samples at different clinical response time points? How many aliquots/volume should be store? • What workflow is the most appropriate in our setting? What SOPs should we adopt? How quickly should we process and freeze a sample? • How long before we start sample distribution?
In this section, we will present what we agreed upon with our committee and from a literature review for development of most SOPs. The committee decided to start by collecting only blood samples from patients and tissue with minimal SOPs to harmonize processes. Afterwards, parents' samples were collected, after modifying the consent and IRB approvals. Then we collected CSF samples. We started with only collecting initial samples, due to lack of personnel to follow patients for clinical remission or relapse, as well as genomic DNA from retrospective patients at the hospital. Later, we managed to gain the assistance of clinical research associates (CRA) to report patients showing relapse or remission in their clinical evaluation. Concerning sample release, the committee agreed to start sample distribution after 5 years of operation, to collect a significant number of samples, and to ensure the quality of processes.
Phase II: Operation
A fully integrated large-scale and coordinated institutional biorepository was started in November, 2012. It was staffed with dedicated Clinical Research Associates, Research Interviewers, and a Managing Head.
Workflow and SOPs
SOPs for collection, processing, and storage were developed based on a literature review of the available guidelines and best practices. 2 These SOPs were written by the head of the biobank and the laboratory personnel. The workflow depends on the support shown from different departments at the hospital. The central hospital laboratory provided in-kind equipment, supplies, and a phlebotomist helped in blood collection. The pathologist provided tissue sampling, and nurses collected samples when requested from the inpatient setting. The Research Department provided personnel and data management; clinical research associates helped in linking to clinical data. The IT Department, hosting the server and the software, and the Medical Engineering Department, provided the expertise for space, infrastructure, and equipment.
Informed consent
All patients with confirmed cancer diagnosis who were accepted to be treated at CCHE were invited to participate. Well-trained interviewers met parents at the outpatient clinic, presented our aims, and explained the scientific and ethical aspects of CCHE-BBR (Table 3). Then they asked the parents/guardians to read the informed consent and the ELSI survey, allowing them to freely participate or not.
Sample procurement
Biofluids
Blood is one of the most common biospecimens used in clinical and translational research. There are several types of anti-coagulants used. Every preservative has its own pros and cons based on the research or application for which it is needed. Issues with blood collection include:
• How we will convince parents of the need for such an invasive technique? • What method to be used in collection? • What type of preservative will be used in collection, to provide for a wide range of research use?? • What blood volume to collect in initial visit?
Procedure
• Immediately after being consented, an initial blood sample is ordered through Cerner ®.
• Blood samples are collected by the central lab phlebotomists at the same time as the sample collected for clinical purposes, to prevent any extra minor invasive technique.
• Research blood tube labels are generated at the blood draw setting with three identifiers; patient's name, MRN, and birth date, and clearly marked as “CCHE-BIOREPOSITORY” to avoid confusion with routine diagnostic samples. Future orders are placed in the system and scheduled with the patient's next clinic visit.
• In case of CSF, samples are collected in the procedure room in polypropylene tubes.
Upon sample arrival, samples are checked for the three identifiers and then the date, sample collection time, sample receiving time are documented on the daily log sheet. Further, samples are de-identified and coded using a CaTissue® ID. All specimens are registered on CaTissue® and the daily log sheet. Also a blood sample is ordered from both parents (Table 4).
Tissue
For ordering and collection of tissues, the daily surgical list is checked and consent status is verified. The eligible cases' requests are sent to the Pathology Department for coordination. The pathologist, after considering the samples required for the clinical diagnosis, will refer extra samples for processing and storage. Each sample arrives labeled with three identifiers; patient's name, MRN, and surgical pathology number (SP-number). Upon sample arrival, the warm ischemia time, type of tissue (normal/malignant), and its condition (fresh/OCT/fixed), are recorded into a log sheet. Then samples are de-identified using the CaTissue® ID. All specimens are registered in CaTissue® and the daily log sheet.
Processing
All steps are performed inside the laminar airflow safety cabinet class A-2. Laboratory personnel should be wearing a safety garment (lab coat).
Biofluids
Patients' blood samples are processed into serum, plasma, buffy coat, and either trizol-lysate or cryopreserved cells are processed based on CBC count and blast content (Fig 4.). For parents' samples, only the buffy coat layer is aliquoted. CSF samples are processed immediately upon arrival. Aliquots are labeled and their volumes with any sample specific notes are documented in the daily log sheet and in CaTissue®.
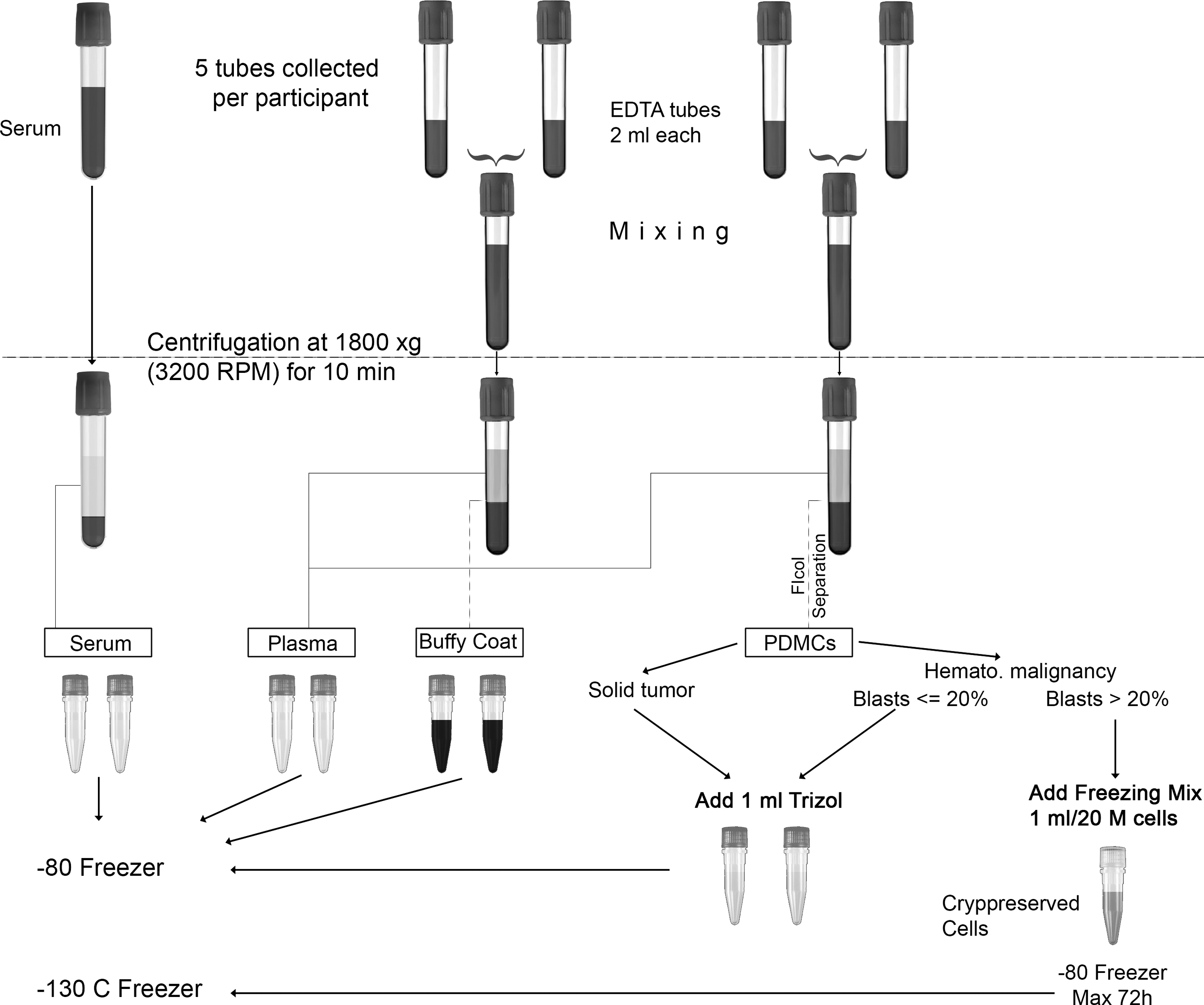
Blood processing SOPs.
Tissue
Processing should start immediately upon sample arrival. They are dissected using sterile surgical blades in sterile petri dishes, into 0.5 cm3 or smaller fragments. They are then transferred into labeled cryovials and documented in the daily log sheet.
Sample storage
Storage should be done while samples are labeled and capped. All serum, plasma, buffy coat aliquots, trizol-lysate, and CSF samples are stored in −80°C freezers, while cryopreserved cells are stored at −80°C for 24 hours and then transferred to liquid nitrogen freezers for long-term permanent storage. Tissue samples are snap frozen in liquid nitrogen and later transferred to 80°C freezers. Specific boxes are devoted to storage of both serum and plasma together, while buffy coats, Trizol-lysate, cryopreserved cells, tissues, and CSF samples are stored solely in their specific numbered and labeled boxes. A sample backup is made via a mirrored storage freezer; where each aliquot is stored in the same position as the other but in a different freezer. This minimizes any hazards of sample loss from a sudden failure or disaster to one of the freezers. 2
Quality assurance plan
A critical point in having an accredited biobank is designing a quality program. Having a supply of high-quality biospecimens (“sample as a mini-me patient”) that realistically and precisely represents the patient's disease pathophysiology, enhances the possibility of high quality research with reliable outcomes. Adherence to approved SOPs helps preserve the quality of the stored samples. Therefore each step in the workflow, starting from collection and ending by retrieval, should follow both a document control system and specimen management system (Fig. 5). All quality management documents are kept in hard and soft copy formats.
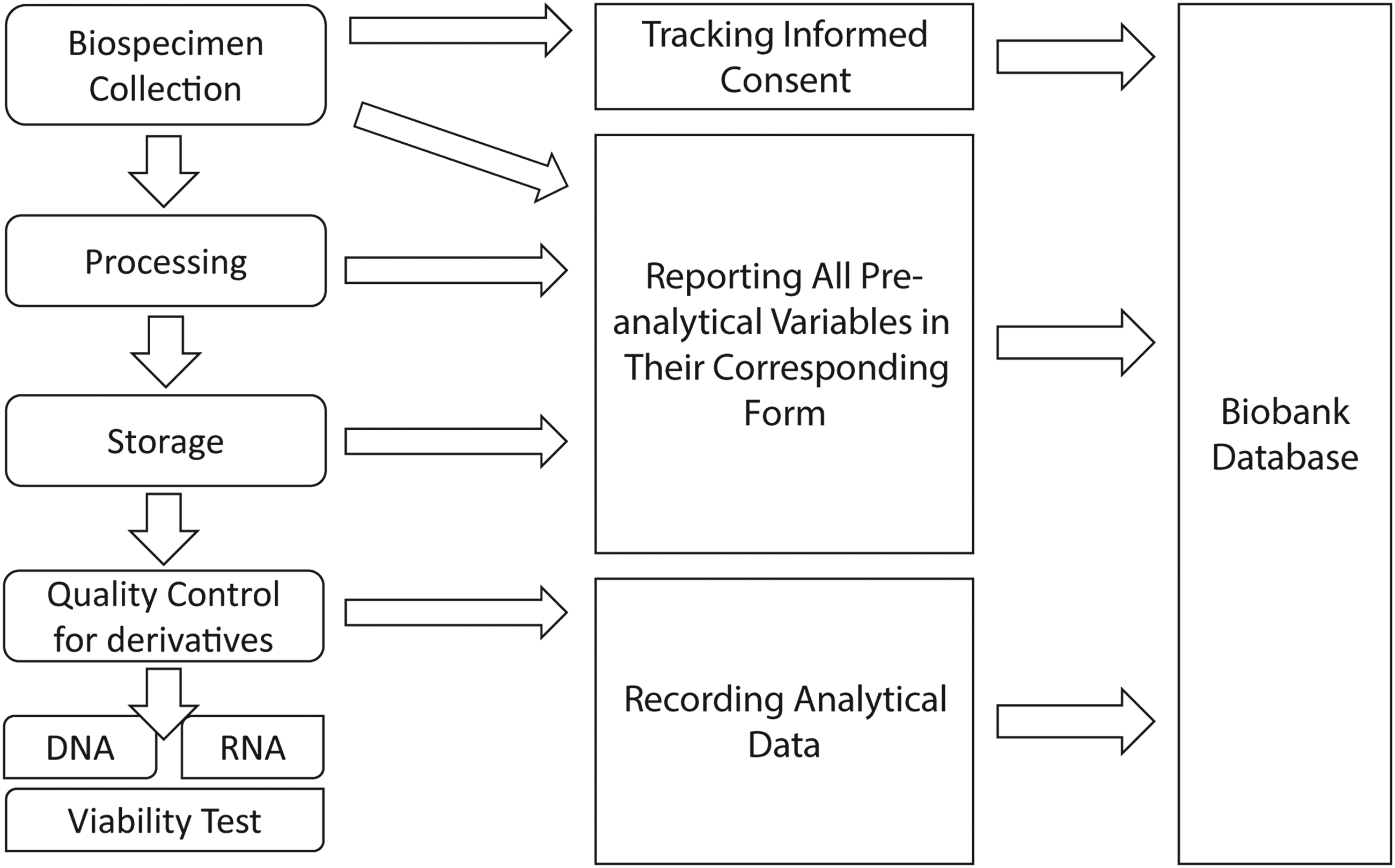
Quality in workflow.
Documentation and reporting management system
Underlying the document management system, we continuously document the data regarding different pre-analytical variables in the specific form, and reporting any incidents or SOPs violations. All sample-related events are documented to manage the criteria of their inclusion and exclusion to specific research studies when requested. In addition, external audits are performed by the BCC.
Specimen management system
We plan to have a quality check for derivatives in the startup phase. Nucleic acids (DNA and RNA) are widely used in most downstream applications. We have chosen to measure the concentration, purity, and integrity of nucleic acids extracted from biofluids and tissue as our gold standard. We used Nanquant® to assess the quantity of nucleic acids at 260 nm and the purity by the OD 260/280 ratio, which must be in the designated range (1.6–2.0). 8 Integrity and fragmentation of nucleic acids is verified by running 50 ng by agarose gel electrophoresis. For the cryopreserved cells, quality is evaluated by the cell viability assay. 9
Access rules/redistribution
Our SOPs ensure that researchers follow the policies for sample requests and that sample retrieval can be performed easily, quickly, and efficiently, while eliminating the risks of contamination and maintaining high integrity and quality of samples. This approach also guarantees adherence to all the ethical and legal requirements. To date we have not released any samples, as agreed to by the committee (i.e., not to distribute samples in the start-up-phase).
Results
We have recently monitored the effectiveness of our biobanking consent process, studying over 5438 patients in a 24-month period. The overwhelming majority of our patients (n = 3812, 70.2%) supported banking, and signed to donate samples from patients/parents for multi-purpose research (unpublished data). Our dedicated research interviewers made a huge effort to achieve this high acceptance rate and played a role in changing the culture. They are building public trust by simply explaining the importance of research and the rationale for banking human biospecimens for research, and alleviating the donors' fears. Tailoring SOPs based on our infrastructure led to standardizing our activities in an easy, fast, accurate way. SOPs are revised/updated every 6 months to ensure adherence to the best practice guidelines.
Conclusion and Lessons Learned
• We overcame the ethical barriers by training our interviewers, who reassured parents.
• Choosing the best evidence-based SOPs that fit with our workflow prevents flaws in the biobanking process.
• IT is an important aspect in biobanking, and choosing software that is easy, flexible, and customizable is crucial.
• Quality is critical in every process.
• Harmoniziation and support from different hospital departments will help in operating and sustaining a biorepository with minimal expenditures.
Phase III: Future Projects
The following will be developed:
• Quality Control Program • Biospecimen Research Program • Microorganisms Bank Section • Cell Line Bank Section
Conclusion
This is a practical, feasible guide to establish a high quality biorepository to support research with minimal resources. This can be done by integrating the biorepository management and workflow with the hospital clinical setting, exerting a minimal extra burden on staff. Having a reliable biorepository can contribute to advances in research and help researchers find a cure.
Footnotes
Acknowledgments
Special thanks to the Biorepository team of interviewers, to Mr. Ahmed Abary and Mrs. Kamar Maged for their dedicated work, and to Mrs. Samar Saied our administrative secretary. We would like to thank the members of the Biorepository Committee for their collaborative spirit. Also, much appreciation goes to Eng. Reda Atta, Head of Medical Engineering Department, and the IT Department for their support. A training grant was provided from Sustainable Science Institute (SSI) as well as funds from the National Bank of Egypt and Terry Fox Marathon.
Author Disclosure Statement
No conflicting financial interests exist.