
Abstract
In 2011, Watson and Barnes proposed a schema for classifying biobanks into 3 groups (mono-, oligo-, and poly-user), primarily based upon biospecimen access policies. We used results from a recent comprehensive survey of cancer biobanks in New South Wales, Australia to assess the applicability of this biobank classification schema in an Australian setting. Cancer biobanks were identified using publicly available data, and by consulting with research managers. A comprehensive survey was developed and administered through a face-to-face setting. Data were analyzed using Microsoft Excel™ 2010 and IBM SPSS Statistics™ version 21.0. The cancer biobank cohort (n=23) represented 5 mono-user biobanks, 7 oligo-user biobanks, and 11 poly-user biobanks, and was analyzed as two groups (mono-/oligo- versus poly-user biobanks). Poly-user biobanks employed significantly more full-time equivalent staff, and were significantly more likely to have a website, share staff between biobanks, access governance support, utilize quality control measures, be aware of biobanking best practice documents, and offer staff training. Mono-/oligo-user biobanks were significantly more likely to seek advice from other biobanks.
Our results further delineate a biobank classification system that is primarily based on access policy, and demonstrate its relevance in an Australian setting.
Introduction
B
The Canadian Tumour Repository Network (CTRNet) system has since been elaborated upon,11,12 and describes three categories of biobank, namely mono-user, oligo-user, and poly-user biobanks.10–12 Mono-user biobanks support a single research project, and feature small-scale biospecimen accrual, and a correspondingly smaller workforce. Oligo-user biobanks support several research groups or projects, but like mono-user biobanks, do not distribute biospecimens to external researchers. In contrast, poly-user biobanks support unspecified research projects undertaken by external researchers, and feature larger biospecimen collections, and greater access to resources.10–12 This user-type system is proposed as a framework for a new phase of biobanking that focuses both on end-users, and serves as an evidence base. 12 In addition, user-type biobank classification has been cited as a basis for proposed improvements to biobank financial sustainability,13–16 certification, 17 and operational/regulatory guidelines,18,19 as well as to usefully describe the diversity between biobanks.20–22
Australia's biobanking sector might be expected to be similar to that in Canada, as Australian and Canadian primary medical research funding bodies have comparable annual budgets, and similar goals.23,24 National funding via the Canadian Institute of Health and Research has led to a well-established and successful nation-wide biobank network, 25 where individual biobanks are funded by host institutions, non-profit organizations, grants, and cost recovery. 15 In contrast, Australia's national medical research funding agency, the National Health and Medical Research Council (NHMRC), did not renew national biobank enabling grant funding beyond 2014. 26
Australia is divided into eight individual states and territories, with New South Wales (NSW) featuring the largest population of 7.5 million people. 27 The NSW cancer control agency (Cancer Institute NSW) first investigated the operations of NSW cancer biobanks through a report published in 2009. 28 This report described highly variable operations across 17 cancer biobanks. 28 which have been echoed in more recent NSW and national reports on biobanking,26,29,30 Despite these recent descriptions of the biobanking landscape in Australia, it is currently unknown whether Australian biobank operations differ significantly according to biospecimen access policies, or other attributes. We therefore used the results of a recent comprehensive survey of biobank staff within NSW cancer biobanks, to investigate the relevance of the CTRNet biobank classification schema10–12 in a different national setting.
Materials and Methods
Cohort identification
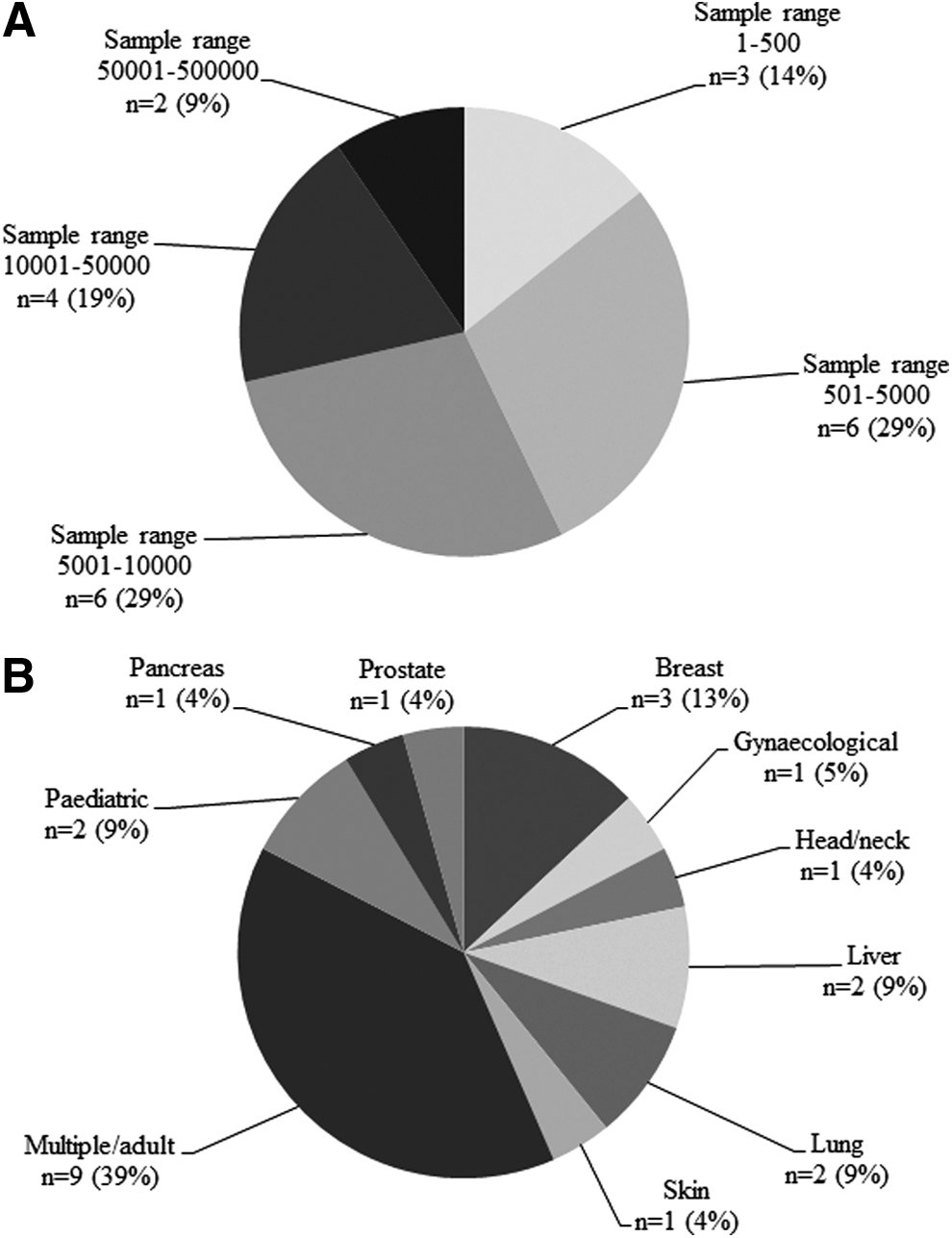
For the purpose of this study, a “cancer biobank” was defined as “a standardized, not-for-profit collection of human biospecimens with associated data records and consent process for the purpose of distribution to cancer researchers for population or disease-specific research.” NSW cancer biobanks meeting this definition were identified using publicly available data via Google,™ and by consulting with research precinct managers. This yielded a cohort of 23 cancer biobanks operating within NSW, of which 21 were fully operational, with the remaining two being actively planned at the time of interview (Table 1). The cohort included biobanks with varying sample collection sizes (Fig. 1A), that also collected different cancer types (Fig. 1B).
-, no available data.
Survey design and conduct
We constructed an extensive survey using Microsoft Excel™ 2011, to be delivered to our biobank cohort through a face-to-face setting. This method was chosen to maximize both the number of responses and their completeness. Survey questions addressed aspects of biobanking activity including sample characteristics, as well as biobank networking, governance, infrastructure, best practice awareness, workforce, funding, accreditation, and operations standardization (Table 2). We included questions that would enable us to classify the cohort according to the CTRNet system.10–12
Survey conduct
The survey was piloted with three biobanks, before being rolled out to the remaining eligible biobanks (n=23 in total). The survey template was e-mailed to participants 1 week prior to each meeting. Interview timeslots were organized by telephone, and two interviewers (AR and JC or JF) were present at each interview. Interviews were recorded to obtain complete and accurate responses, and recordings were then transcribed into a single master spreadsheet. Where possible, survey data such as website information, type of biobank, disease focus, specimen types collected, sample storage, number of samples, researcher access policy, biobank governance, and length of time of operation were independently verified by accessing individual biobank websites. The study protocol was reviewed by the Sydney Children's Hospital Network Human Research Ethics Committee, and was deemed exempt from review, as the project did not fulfil the Australian NHMRC's National Statement on Ethical Conduct in Human Research's definition of research. 31
Biobank classification
Biobanks were classified according to the CTRNet system,10–12 where a mono-user biobank aims to facilitate one research project, an oligo-user biobank supports several research groups, and a poly-user biobank supports unspecified research projects undertaken by external researchers. We will refer to the latter access policy as “open-access.” Sufficient data were available to allow the classification of each biobank within the cohort, including the two biobanks in the planning phase. We then used a binary classification system (mono-/oligo-user, versus poly-user) for analyses, as poly-user biobanks differ from the former two groups by having an open-access policy.10–12 Biobank collection size was also used as a discriminator. Our cohort was divided into two groups for this purpose, using a cut point of 5000 samples. While previous studies have utilized different collection size cut points,10,12 we chose a cut point of 5000 samples to provide two similarly sized groups of biobanks for statistical analyses. Data were collated and analyzed using Microsoft Excel™ 2011 and IBM SPSS Statistics™ version 21.0. Fisher's Exact Test was used to compare two proportions, and the Mann-Whitney Test was used to compare two medians. A p value ≤0.05 was considered statistically significant.
Results
Definition of NSW cancer biobank cohort
According to the CTRNet system,10–12 cancer biobanks in NSW represented 5 mono-user biobanks (5/23, 22%), 7 oligo-user biobanks (7/23, 30%), and 11 poly-user biobanks (11/23, 48%) (Table 1). A feature that immediately distinguished mono-/oligo-user (n=12) and poly-user (n=11) biobank groups was their Internet presence, with all poly-user biobanks featuring a website, compared with 2/12 (17%) mono-/oligo-user biobanks (Fisher's Exact test p<0.001, n=23) (Table 3).
Fisher's Exact Test; bMann-Whitney Test.
ABNA, Australasian Biospecimen Network Association; FTE, Full-time equivalent staff.
Workforce
All operational NSW cancer biobanks (n=21) cited personnel as their largest expense. Poly-user biobanks employed significantly more full-time equivalent (FTE) staff than mono-/oligo-user biobanks (Mann-Whitney test, p=0.008, n=20; Table 3), and more FTE staff were employed in biobanks with a website (Mann-Whitney test, p=0.013, n=20; Table 3). Biobanks who shared staff with other NSW cancer biobanks had significantly larger sample collections than biobanks whose staff were not shared (Fisher's Exact test p=0.007, n=21; Table 3).
Most surveyed biobanks (12/22, 55%) indicated that staff received no formal biobank-specific training, with the remainder (10/22, 45%) indicating that staff training consisted of following standard operating procedures and/or was performed “on the job.” Poly-user biobanks were significantly more likely than mono-/oligo-user biobanks to offer formal staff training (Fisher's Exact test p=0.008, n=22; Table 3). Whereas most biobanks were able to send staff to conferences (15/23, 65%), typically on a yearly basis, a significant minority did not (8/23, 35%). Staff from poly-user biobanks were significantly more likely to attend biobanking conferences (Fisher's Exact test p=0.027, n=23; Table 3). Poly-user biobank staff were also more likely to belong to the Australasian Biospecimen Network Association (ABNA), an association of biobanking professionals 32 (Fisher's Exact test p=0.012, n=23, Table 3).
Funding and governance
Only a minority of cancer biobanks reported recurrent funding (6/22, 27%), with funding of many biobanks due to end in 2014 (7/23, 30%). Most biobanks reported a map or plan for sustainability (13/21, 62%), but a sizeable proportion did not (8/21, 38%). Most biobanks reported accessing local governance support (14/23, 61%), however poly-user biobanks were significantly more likely to access governance support than mono/oligo-user biobanks (Fisher's Exact test p=0.001, n=21) (Table 3).
Quality control (QC) and accreditation
Most cancer biobanks (14/22, 64%) indicated that they routinely carried out QC activities around biospecimen quality, which in some cases also included database audits (6/22, 27%). Only one biobank reported utilizing a Quality Manager (1/22, 5%), and this biobank had a complete Quality Management System. Poly-user biobanks were significantly more likely to employ QC measures than mono-/oligo-user biobanks (Fisher's Exact test p=0.001, n=23; Table 3), with all poly-user biobanks (11/11, 100%) reporting the use of QC measures in their biobank.
Standardization and biobanking best practices
Although most cancer biobanks surveyed (18/23, 78%) were aware of at least one set of biobanking best practices, a minority (5/23, 22%) were not aware of any. Awareness of best practices differed significantly when compared with type of biobank, with more poly-user biobanks being aware of biobanking best practices than mono-/oligo-user biobanks (Fisher's Exact test p=0.037, n=23; Table 3). All poly-user biobanks (11/11, 100%) were aware of one or more biobanking best practice documents, compared with 7/12 (58%) of mono-/oligo-user biobanks.
Biobank networking
Almost all biobanks (19/23, 83%) saw value in networking with other cancer biobanks in NSW, with the most frequently nominated drivers of biobank networking being common sample types (n=11), existing networks (n=7), and favorable geography or common standard operating procedures (n=5 each). Biobanks with larger sample numbers (>5000 samples) were more likely to refer researchers to another NSW cancer biobank collecting the same sample type than biobanks with smaller sample numbers (≤5000 samples) (Fisher's Exact test p=0.034, n=16, Table 3). Mono-/oligo-user biobanks were significantly more likely to seek advice from other biobanks (Fisher's Exact test p=0.037, n=23; Table 3).
Discussion
We conducted a comprehensive survey of NSW cancer biobanks, which enabled the first quantitative assessment of the relevance of the CTRNet classification schema in an Australian setting. The CTRNet schema was selected because this primarily defines biobanks according to their access policy, and ensures that biobank diversity is appreciated, biobanks are defined for researchers, and funders are assisted in their understanding of appropriate funding levels. 10 As a previous report had also highlighted operational diversity between cancer biobanks in NSW, 28 the CTRNet classification system was potentially relevant in our setting.
We divided our cohort into mono-/oligo-user, and poly-user biobanks, as poly-user biobanks differ from the other two groups in their open-access policy.10–12 To our knowledge, this binary classification has not been used in previous analyses. Binary classification resulted in an almost equal division of NSW cancer biobanks between those with samples provided to research collaborators (mono-/oligo- user biobanks, 12/23, 52%), and those with an open-access policy (poly-user biobanks, 11/23, 48%). This ratio differs substantially from a described Canadian cohort, 33 where most biobanks were described as mono- or oligo-user biobanks.
Notwithstanding the possibility of inter-study variations in biobank classification, this large discrepancy suggests substantial differences in biobank governance, funding, and/or end-user demands between Canada and Australia. These differences provided further impetus to investigate the relevance of the CTRNet classification system in a different national setting.
Statistical comparisons highlighted some reasonable or expected differences between mono-/oligo-user and poly-user cancer biobanks. For example, poly-user biobanks were significantly more likely to feature a website. As biobank websites can serve as marketing tools for the promotion and distribution of biospecimens to unspecified end-users, it was not surprising that biobank websites were a feature of all poly-user biobanks in our cohort. Increased FTE staff numbers were also identified in poly-user biobanks, confirming this aspect of the CTRNet definition of a poly-user biobank. 10 Poly-user biobanks were also described as having access to larger resources/ infrastructure, 12 which was supported by significantly more poly-user cancer biobanks accessing governance support (Table 3).
While levels of biobank funding were not directly addressed by our survey, greater FTE staff numbers in poly-user biobanks suggest that this group had more funding available than mono-/oligo-user biobanks. Other results indicate that the consequences of such resourcing differences could be far-reaching. Poly-user biobanks were more likely to undertake QC measures, and poly-user biobank interviewees were more frequently aware of biobanking best practices. Poly-user biobanks were also more likely to engage in formal staff training, to send biobank staff to conferences, and to employ staff who are members of ABNA. 32 These differences are concerning, as they could directly and/or indirectly contribute to variable biospecimen quality between and within individual biobanks. It is now well recognized that high, uniform biospecimen quality is integral for translational research,34,35 and conversely, that inadequate biospecimen quality can generate spurious results, waste already limited resources, and impede research progress. 36
Funding biobanking operations in NSW clearly remains a major challenge, with approximately one quarter of cancer biobanks reporting recurrent funding. While new investment in this sector is undoubtedly required, our results also suggest approaches to better use the limited resources available. Resource-sharing between biobanks can reduce duplication of effort, and promote more uniform operations across different biobank types, 37 potentially reducing the QC, best practice and workforce training/education variations that we have noted. Cancer biobanks with larger sample numbers, a feature of poly-user biobanks,10,14 were significantly more likely to share staff, and to refer researchers to other NSW cancer biobanks that collect the same sample type. Networking is particularly useful to poly-user biobanks, as this allows researchers to access larger biospecimen cohorts.7,38 However, mono-/oligo-user biobanks can also benefit from networking, as this could increase their access to best practice documents and procedures, shared trained staff, and other infrastructure. The fact that mono-/ oligo-user biobanks saw value in biobank networking was indicated by their being significantly more likely to seek advice from other cancer biobanks. This result suggested a self-awareness of operational limitations, and a desire to overcome these.
In summary, our results further delineate a biobank classification system that is primarily based on biospecimen access policy, and demonstrate the utility of this model in an Australian setting. While some differences between mono-/oligo- and poly-user cancer biobanks agreed with expectations, there were also unexpected differences in the undertaking of QC measures, awareness of biobanking best practices, staff training, and conference attendance. We acknowledge that these differences emerged from the study of a small cancer biobank cohort, and that analyses of larger, nationwide cohorts would be valuable. However, these findings are likely to reflect the state of biobanking at a national level.
Our results indicate that further investment will be required to achieve uniform biobanking standards and performance across the Australian biobanking sector. Our results also suggest that targeted policies may be required to improve operations within mono- and oligo-user biobanks. These could include the formalization and resourcing of biobank networks that are suited to local conditions, from which longer-term harmonized structures can be planned.
Footnotes
Acknowledgments
The authors would like to thank Dr. Liz Barnes (Kids Research Institute) for statistical advice, and Dr. Erdahl Teber and Mr. Matloob Khushi (Kids Cancer Alliance), Dr. Sonia Yip (Sydney Catalyst Translational Cancer Research Centre), Professor Nick Hawkins (Translational Cancer Research Network), Professor Anna DeFazio and Professor Christine Clarke (Sydney West Translational Cancer Research Centre), and Associate Professor Deborah Marsh (Sydney Vital) for project discussions. We also gratefully acknowledge Cancer Institute New South Wales for providing funding for this project (Grant ID: 13/BIO/1-01), and all survey interviewees for their input.
Author Disclosure Statement
The authors declare that there are no conflicts of interest arising from the publication of this work.