
Abstract
Background:
A blood sample containing circulating tumor cells (CTCs) may serve as a surrogate for metastasis in invasive cancer. Cryopreservation will provide new opportunities in management of clinical samples in the laboratory and allow collection of samples over time for future analysis of existing and upcoming cancer biomarkers.
Methods:
Blood samples from healthy volunteers were spiked with high (∼500) and low (∼50) number of tumor cells from culture. The samples were stored at −80C with cryopreservative dimethyl sulfoxide mixed with Roswell Park Memorial Institute 1640 medium. Flow cytometry tested if cryopreservation affected specific biomarkers regularly used to detect CTCs, i.e. cytokeratin (CK) and epithelial cell adhesion molecule (EpCAM) and white blood cell specific lymphocyte common antigen (CD45). After various time intervals (up to 6 months), samples were thawed and tumor cell recovery (enumeration) was examined. Clinical samples may differ from cell line studies, so the cryopreservation protocol was tested on 17 patients with invasive breast cancer and tumor cell recovery was examined. Two blood samples were drawn from each patient.
Results:
Biomarkers, CK, CD45, and EpCAM, were not affected by the freezing and thawing procedures. Cryopreserved samples (n = 2) spiked with a high number of tumor cells (∼500) had a ∼90% recovery compared with the spiked fresh samples. In samples spiked with lower numbers of tumor cells (median = 43 in n = 5 samples), the recovery was 63% after cryopreservation (median 27 tumor cells), p = 0.03. With an even lower number of spiked tumor cells (median = 3 in n = 8 samples), the recovery rate of tumor cells after cryopreservation did not seem to be affected (median = 8), p = 0.09. Time of cryopreservation did not affect recovery. When testing the effect of cryopreservation on enumeration in clinical samples, no difference was observed in the number of CTCs between the fresh and the cryopreserved samples based on n = 17 pairs, p = 0.83; however, the variation was large. This large variation was confirmed by clinically paired fresh samples (n = 64 pairs), where 95% of the samples (<30 CTCs) vary in number up to ±15 CTCs, p = 0.18.
Conclusions:
A small loss of CTCs after cryopreservation may be expected; however, cryopreservation of CTCs for biomarker characterization for clinical applications seems promising.
Introduction
T
Water crystals are dynamic in nature and will burst or shrink cells when they form during freezing. This may, however, be minimized by cryoprotective additives such as buffering intracellular salts or forming hydrogen bonds with extracellular water molecules to reduce osmotic pressures and crystal formations. 9 Numerous applications for cryopreservation have previously been described, including for peripheral blood cells.9–11 This includes dimethyl sulfoxide (DMSO) mixed with Roswell Park Memorial Institute (RPMI) 1640 medium at −80°C, which was tested in the present study.
CTC-derived biomarkers are used for characterization and, depending on the applied methodology, also for their detection and/or enumeration.2,8 CTCs detected by the CytoTrack™ system stain positive for nuclear DNA and cytokeratins (CKs) in the cytoplasm, and they are differentiated from other nucleated blood cells by being CD45 negative—a transmembrane glycoprotein expressed in hematopoietic cells.2,6 Freezing of CTCs for biobanks, scientific, or clinical investigations requires long-term preservation of cell morphology and relevant biomarkers for compatibility with the CTC characterization methodology. 11
In this study, 20% DMSO in RPMI 1640 for cryopreservation of CTCs at −80°C was assessed for CTC enumeration and biomarker characterization using the CytoTrack instrumentation platform and reagents. The cryopreservative abilities were evaluated for samples cryopreserved for variable time intervals. Various tumor cell lines spiked into blood from healthy volunteers (i.e., MCF-7, SK-BR-3, MDA-MB-231) as well as paired clinical blood samples from 17 patients with invasive breast cancer were tested.
Methods
Study design
In summary, we combined the CytoTrack-based CTC analysis with a cryoprotective protocol, that is, DMSO mixed with RPMI 1640 medium at −80°C, as illustrated in Figure 1. In this study, the cryopreservation method was assessed in blood from healthy volunteers spiked with human cancer cell lines with respect to biomarker staining intensity and recovery of the spiked tumor cells (see the Tumor cell line studies section). Subsequently, the cryopreservation method was tested on clinical specimens with regard to recovery of CTCs (see the Clinical CTC studies section, Fig. 2).

The CytoTrack CTC analysis protocol combined with cryopreservation of the CTCs. The isolated buffy coat with CTCs is diluted in 20% DMSO in RPMI 1640 and stored at −80°C. CTC, circulating tumor cell; DMSO, dimethyl sulfoxide; RPMI, Roswell Park Memorial Institute.
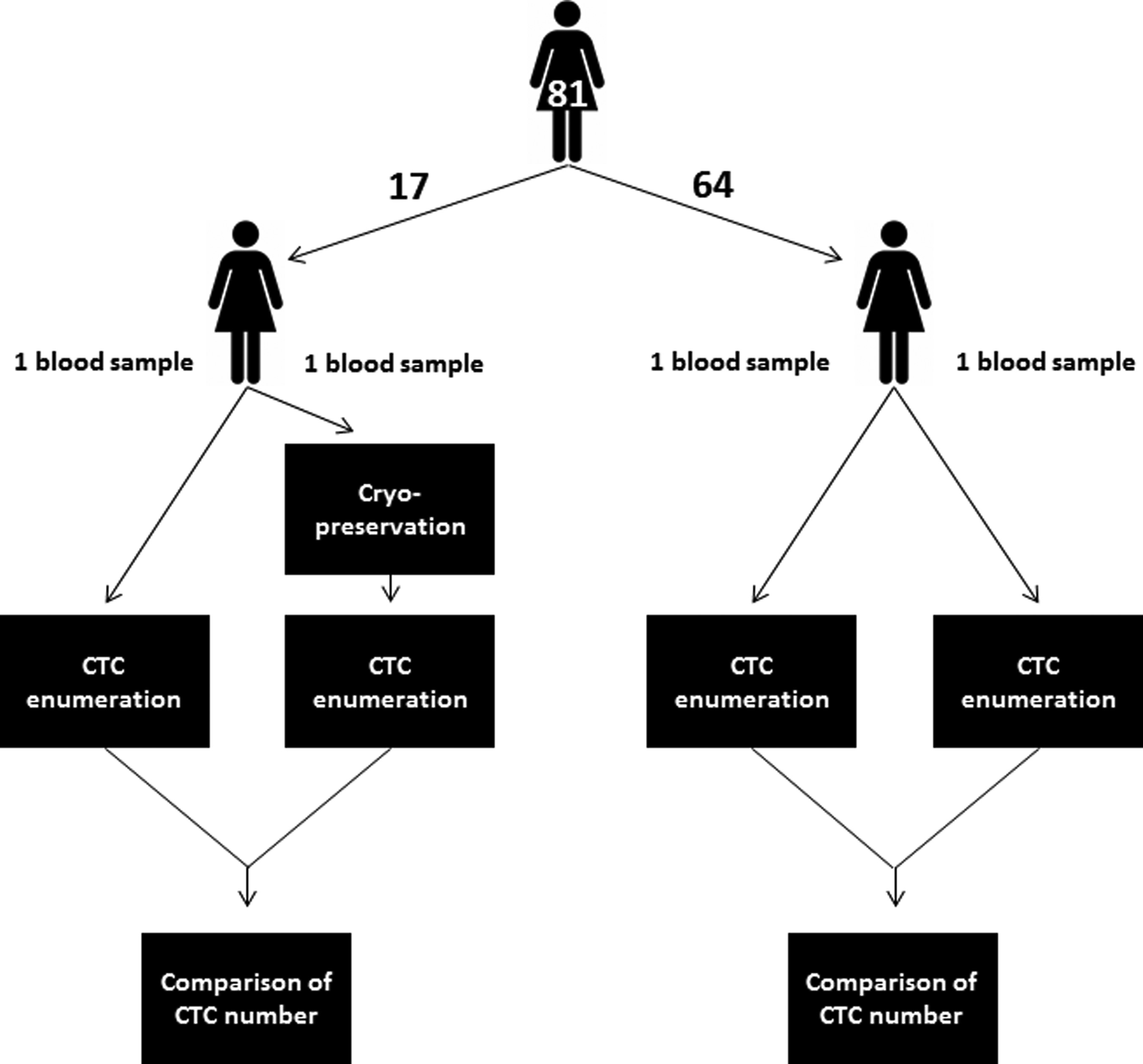
A flowchart of the clinical studies. Paired blood samples from 81 patients with invasive breast cancer were tested for number of CTCs. Samples were taken consecutively. For fresh/fresh paired samples, the inclusion period was November 5, 2012, to September 25, 2014, with the objective to test the biological variation of CTC enumeration within sampling. For fresh/cryopreserved paired samples, the inclusion period was October 16, 2014, to May 18, 2015, to test the effect of cryopreservation on CTC enumeration.
Tumor cell line studies
Cell cultures
The human breast cancer cell lines, MCF-7, SK-BR-3, and MDA-MB-231 (American Type Culture Collection [ATCC], Manassas, VA), were cultured in Dulbecco's modified Eagle's medium-GlutaMAX™ (Gibco, Grand Island, NY), supplemented with 1% penicillin–streptomycin (Gibco) and 10% heat-inactivated fetal bovine serum (Gibco). The cancer cell lines were grown in a humidified atmosphere containing 5% CO2 at 37°C. The cells were washed with Dulbecco's phosphate-buffered saline (DPBS) without calcium and magnesium (Gibco), followed by harvesting with TrypLe™ Express (Gibco).
Healthy volunteers
For the spiking experiments, peripheral blood (7.5 mL) from healthy volunteers (Nordsjællands Hospital, Hillerød, Denmark) was used. The blood was collected in EDTA tubes for analysis within 4 hours or CellSave™ preservative tubes (Janssen Diagnostics, LLC, Raritan, NJ) for analysis within 96 hours. Before analysis, the blood samples were stored at ambient temperature. A written informed consent in accordance with the Declaration of Helsinki was obtained from each participant before sample collection.
Clinical CTC studies
The clinical XeNa study (clinicaltrials.gov, XeNa study, identifier: NCT01941771) included blood samples from 120 patients with invasive breast cancer collected in CellSave preservative tubes (7.5 mL).
The present study used blood samples from the XeNa study, with the following exclusion criteria: (1) samples not taken in duplicate, (2) nonsuccessful samples (coagulation, postage issues, or other errors), (3) samples taken for long-term storage (currently still frozen).
Please see flow chart in Figure 2.
From November 2012 to September 2014, paired blood samples were collected to examine the variation of the number of CTCs between samples taken consecutively from the same patient. From 86 patients, 64 were approved using the exclusion criteria. The samples (n = 128) were analyzed for CTC enumeration within 96 hours as prescribed by CellSave instructions. All samples were analyzed fresh without cryopreservation and all samples were included for analysis whether they had no or one or more CTCs.
From October 2014 to May 2015, another collection of 25 paired samples was taken to examine the effect of cryopreservation. Only CTC-positive samples were included, that is, one of the paired samples (fresh or cryopreserved) should have one or more CTCs. Thus, of the 25 patients in total, only paired samples from 17 patients were included for analysis. The fresh samples (n = 17) were analyzed for CTC enumeration within 96 hours as prescribed by CellSave instructions, and the matched samples (n = 17) were cryopreserved by storage at −80°C for 3–90 days before analysis. A written informed consent in accordance with the Declaration of Helsinki was obtained from each participant before sample collection.
Procedures equivalent for both tumor cell line studies and clinical CTC studies
Isolation of nucleated cells
All blood samples—both clinical blood samples and spiked blood samples from healthy volunteers—were centrifuged at 2500 g at 4°C for 15 minutes for isolation of nucleated cells. The buffy coat layers containing all nucleated cells were isolated manually (∼1–2 mL) and transferred to 15-mL Falcon tubes. The Falcon tubes were either prepared for cryopreservation or proceeded immediately to CytoTrack analysis, as described below.
Cryopreservation
For cryopreservation of nucleated cells, a chilled medium of 20% DMSO in RPMI 1640 was used. To each isolated buffy coat, 5 mL of the cryopreservation medium was added and mixed with the cells by inverting the Falcon tubes. The samples were immediately stored at −80°C. Before analysis, the samples were thawed in a water bath at 37°C for ∼3 minutes. The samples were then centrifuged at 2500 g at 4°C for 15 minutes and the supernatants were discarded. The samples were then stained and analyzed according to the CytoTrack protocol as described below.
CytoTrack protocol—staining
Nucleated cells (white blood cells [WBCs], spiked tumor cells, and CTCs) were stained using CTC Stain™ (CytoTrack ApS, Lyngby, Denmark) according to the manufacturer's instructions. Briefly, immediately after isolation of buffy coats (or after thawing of preserved buffy coat for the cryopreserved samples), remaining red blood cells were lysed, and nucleated cells were fixed with BD FACS™ Lysing Solution (BD Bioscience, New Jersey, NY) for 15 minutes and centrifuged at 2500 g at 4°C for 15 minutes. The cell pellets were stained using CTC Stain comprising a mixture of anti-CD45/NIR (near infrared) antibody, anti-CKs/green antibody, DAPI nuclear stain (omitted in flow cytometry analysis), and antiepithelial cell adhesion molecule (EpCAM)/yellow antibody for EpCAM expression (EpCAM is optional in the CytoTrack protocol) for 1 hour at 2°C–8°C. Subsequently, the cells were washed with PBS with 1% bovine serum albumin (VWR, Radnor, PA) and finally resuspended in 1 mL filtered deionized H2O.2,6
CytoTrack protocol—analysis
After staining, the 1 mL cell suspension was smeared onto a CytoDisc™ (CytoTrack ApS) in a MARS1200 laminar airflow fume hood (Labogene Aps, Lynge, Denmark). The smear was air-dried at ambient temperatures, mounted with mounting medium (Olink, Uppsala, Sweden), covered with a CytoCover™ (CytoTrack ApS), and sealed with rubber cement (FixoGum, Marabu Scandinavia) along the edge. The CytoDisc was inserted into a CytoTrack CT4 scanner (CytoTrack) and locked into position using the notch function. 2 Spiked tumor cells or CTCs on the CytoDisc were detected and enumerated by ultra-sensitive scanning fluorescence microscopy in the green channel (CK) using a 20× scanning objective. Scanning was performed within 1 week of smearing. Green events were recorded and listed in a hotspot table using CytoTrack software v.1.6. Each hotspot was visually inspected by the operator in the green channel. An image gallery of positions on the CytoDisc with possible CTCs was automatically generated using the DAPI, green, NIR, and optionally the yellow channel and a 20× imaging objective. The possible CTCs in the image gallery were then analyzed using the following morphologic criteria: nearly round and size >4 μm, with visible DAPI-stained nucleus and at least 50% association with the CK-positive cytoplasm, and CD45-negative cell surface. This definition resembles other methods for analysis of CTCs. 8
Procedures specific for the tumor cell line studies
Impact of cryopreservation on biomarkers—flow cytometry analysis
To study the impact of cryopreservation on the target molecules (epitopes) for CTC enumeration and characterization, breast cancer cells and WBCs were stained with anti-CD45, anti-CKs, or anti-EpCAM on both fresh (noncryopreserved) and cryopreserved samples.
Two blood samples from healthy volunteers were used to examine the CD45 staining characteristics of the WBCs before (n = 1) and after 1 day of cryopreservation (n = 1).
The staining capabilities of epithelial biomarker, CK, were tested by flow cytometry after freezing a sample with pure MCF-7 breast cancer cells for 20 days at −80°C in comparison with flow cytometry of a fresh sample of tumor cells.
MCF-7 breast cancer cells were also used to examine the EpCAM staining characteristics in a fresh and a cryopreserved (1 day at −80°C) tumor cell sample.
Analyses were performed by flow cytometry for quantitative assessment. After staining, 300 μL of cell suspension was further diluted into 2 mL filtered deionized H2O and analyzed using an FACS Calibur flow cytometer (BD Bioscience). The results were analyzed with CellQuest Pro Software (BD Bioscience).
Quantitative recovery after cryopreservation in blood samples spiked with a low number of tumor cells
Two MDA-MB-231 tumor cell suspensions were prepared from stepwise dilution of 10 million cells in 1000 μL PBS to theoretically 3200 cells in 1000 μL PBS, thus 3.2 cells/μL PBS. From each of the two cell suspensions, a set of samples was made, named Set 1 and Set 2. To all samples in each set, 15 mL of the respective cell suspension was added to blood samples from healthy volunteers (n = 5 in Set 1, n = 8 in Set 2) and to 10 control slides per set. The control slides were made to examine the average amount of tumor cells added to the blood samples (which may vary from the theoretically added 3.2 tumor cells ×15 μL). The spiked blood samples were all cryopreserved and analyzed by CTC enumeration over a 6-month period.
Quantitative recovery after cryopreservation in blood samples spiked with a high number of tumor cells
To determine recovery of tumor cells after freezing, three types of samples using blood from healthy volunteers were generated: fresh (nonpreserved) blood samples (n = 3, two in EDTA, one in CellSave), cryopreserved blood samples (n = 3, two in EDTA, one in CellSave), and one blood sample using PBS in an EDTA tube for cryopreservation as negative control (this negative control was not spiked with tumor cells, however WBC were counted). SK-BR-3 breast cancer cells was spiked into two of the EDTA tubes and two of the CellSave tubes (500 tumor cells were estimated and spiked after dilution from 1 million tumor cells per 100 mL to mimic a high number of CTCs in blood). One EDTA and one CellSave tube was cryopreserved, and the recovery of tumor cells after thawing was estimated as a percentage of the fresh samples. As a positive control, recovery of the abundant WBCs was tested using the remaining two EDTA tubes with blood from the healthy volunteers. Routine WBC counts were performed by Beckman Coulter ACT8 according to the manufacturer's instructions. For the negative control (sample cryopreserved in PBS), the Bürker–Türk counting chamber was used for manual WBC counting due to failure of the automated approach.
Statistical analysis
Tumor cell line studies
The median (range) describes the data and the nonparametric Mann–Whitney test was used to compare the control samples with the cryopreserved samples in Set 1 and Set 2.
Clinical CTC studies
CTCs measured in fresh versus fresh and fresh versus cryopreserved samples are illustrated in dot plots, and Deming regression analysis is applied, which considers both X and Y to be subject to measurement error. Bland–Altman plots are used to show the distribution of the CTC differences between the paired measurements. Only the differences of the fresh paired samples were normally distributed (tested on histograms; not shown), thus parametric limits were used for fresh versus fresh (mean bias, 95% limits of agreement), and nonparametric limits were applied to the fresh versus cryopreserved samples (median, 10th, and 90th percentiles). Nonparametric statistics are used for Table 2 (median, quartiles, the Spearman correlation coefficient r, and Wilcoxon paired test) to show the distribution of CTCs in the four groups and for group comparisons of the paired samples.
Data were analyzed with GraphPad Prism version 4 software and tested with a significance level of α = 0.05.
Results
Tumor cell line studies
Impact of cryopreservation on biomarkers—flow cytometry
The immunochemical properties of three biomarkers, CD45, CK, and EpCAM, were tested on MCF-7 tumor cells with flow cytometry. The biomarkers did not seem negatively affected by cryopreservation and thawing (see histograms on Fig. 3). CK fluorescence staining intensity even appeared to be slightly better after cryopreservation with the curve rightshifted for higher relative fluorescence for the cryopreserved sample compared with the fresh sample (Fig. 3B).
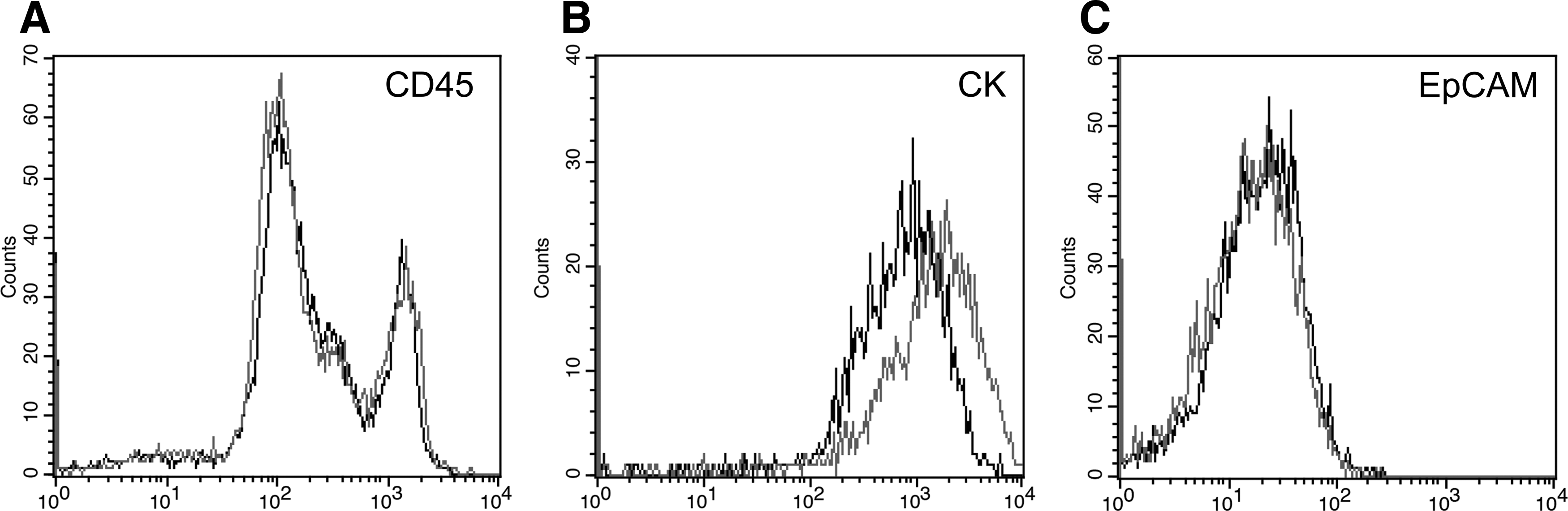
Flow cytometry was performed to examine biomarker stability after cryopreservation, and histograms with cell counts on the Y-axis and relative fluorescence on the X-axis show that all three tested biomarkers are well preserved (CD45, CK, and EpCAM).
Quantitative recovery after cryopreservation in blood samples spiked with a low number of tumor cells
The two different MDA-MB-231 cell suspensions were used in Set 1 and Set 2, respectively. In Set 1, the control samples (n = 10) showed that each sample was spiked with median (range) 43 (21–53) tumor cells. In Set 2, control samples showed that each sample was spiked with 3 (0–14) tumor cells (based on only n = 5 controls in Set 2 due to manual error and loss of five controls). Results on tumor cell recovery after freezing are shown in Figure 4 and show constant recovery during the period of 6 months with a median of 27 (13–34) tumor cells per sample in Set 1 (n = 5), which is a 63% recovery compared with the control slides on average (27/43 tumor cells). The nonparametric Mann–Whitney test showed that the tumor cell number in the control group is higher than in the cryopreserved samples (p = 0.03) for Set 1. In Set 2, no difference between control slides (n = 5) and cryopreserved samples (n = 8) was observed (p = 0.09), where a median of 8 (0–22) tumor cells per blood sample were counted. Thus, the recovery in sample Set 2 shows no loss of tumor cells. Note that a large variation in data appeared in both groups, and the groups were based on few samples.

Recovery of breast cancer cells after cryopreservation. Two breast cancer cell line MDA-MB-231 suspensions were, respectively, spiked into two sets of donor blood samples. Buffy coat with tumor cells was preserved in 20% DMSO in RPMI 1640 preservative and frozen at −80°C in different time periods over 6 months and analyzed on a CytoDisc to measure the number of tumor cells (n).
Quantitative recovery after cryopreservation in blood samples spiked with a high number of tumor cells
After cryopreservation of blood samples with ∼500 tumor cells, the tumor cell loss was ∼10% compared with fresh samples. The trend was similar for both EDTA and CellSave tubes, Table 1. The positive control, WBC count, showed an expected 100% recovery, and the negative control using PBS showed, as expected, an almost 90% loss of WBCs in the blood sample from a healthy volunteer.
Three types of samples were generated: fresh samples, one sample where the buffy coat was cryopreserved with PBS (negative control), or cryopreserved with 20% DMSO in RPMI 1640 preservative.
Estimated based on 227 from analysis of half of the CytoDisc.
Number of WBCs is in n/mL; n, the number of tumor cells detected in one blood sample smeared on a CytoDisc; %, cryopreserved sample (n)/fresh sample (n).
DMSO, dimethyl sulfoxide; PBS, phosphate-buffered saline; RPMI, Roswell Park Memorial Institute; WBC, white blood cell.
Clinical CTC studies
CTC enumeration—comparison of paired fresh blood samples
Paired fresh samples from 64 different patients were compared. Of the 64 pairs, 35 were CTC positive in one or both of the paired samples. Regression analysis in Figure 5A, Bland–Altman plot in Figure 5C, and correlation analysis in Table 2 show a large variation in CTC enumeration of fresh samples taken consecutively from the same patient.

♦, The variation of the CTC number in blood samples taken consecutively from the same breast cancer patients is illustrated in
See also dot plot in Figure 4.
CTC, circulating tumor cell; NS, not significant.
CTC enumeration—before and after cryopreservation
The number of CTCs was either increased or decreased after cryopreservation compared with the paired fresh sample, as shown in the Bland–Altman plot in Figure 5D, and the paired test showed no difference between the two groups (p = 0.83). The Bland-Altman plot also shows that the difference between paired samples may be large. From 16 paired samples, there is no trend in data as the slope in regression analysis was not different from zero (p = 0.25), Figure 5B. Analysis was performed by excluding the 17th data point (900,803) because this was the only sample with such a high number of CTCs, which technically bias the regression. However, this specific sample shows a 10% loss of tumor cells in the cryopreserved samples compared with the fresh. This may be due to biological variation as seen from the fresh paired samples or due to the cryopreservation step as suggested in the tumor cell studies—or more likely both.
Discussion
Enumeration and characterization of CTCs have significant potential as a supplement to contemporary methods for cancer diagnostics and predictive medicine.1–5 Numerous instruments and methods for CTC enumeration and characterization have been described and may be divided into whole cells and nucleic acid-based analysis using immunocytochemical or molecular assays, respectively.2,8,12,13 All methods, however, are reasonably time-consuming requiring significant laboratory resources, and only few samples can be processed at a time. Current methods prescribe same-day analysis when using normal EDTA blood collection tubes and up to 4 days when using special tubes, such as CellSave preservative blood collection tubes. Bottlenecks may therefore occur if numerous clinical samples are received simultaneously, with the risk of samples not being analyzed within the relatively short time period for testing. Moreover, potential biobanking of samples with CTCs would allow for clinical studies of future prospect biomarkers using well-characterized samples with long-term clinical information including patient outcome. So, with the novel methods for analyzing CTCs, there is also a need for preserving blood samples in a way that does not affect the number and characteristics of the rare cells in the blood for later CTC analysis.
Certain studies that test the cryoprotective abilities of cells also focus on cell viability, which may be crucial, for example, for sperm cells or blood progenitor cells.14,15 Viability tests were not performed in this study since the CytoTrack protocol does not need viable cells and cells are formalin fixed during RBC lysis. The present study primarily focused on cell recovery (enumeration), and we also tested the immunochemical abilities for three specific intracellular and surface biomarkers that did not seem to be affected by the freezing and thawing. Other applied biomarkers may be more or less fragile and the cryopreservation and thawing should be tested for each phenotype of interest.11,16
From our tumor cell line study, we observed a tumor cell loss of ∼10% after cryopreservation when the number of tumor cells in blood was high, but in samples with a low number of tumor cells, the samples appear more prone to variations with cell loss on average up to 40% in Set 1 and with no obvious cell loss in Set 2. Time of cryopreservation did not seem to affect the recovery rate (in either Set 1 or Set 2). However, the cell loss may not necessarily be due to the freezing and thawing procedures but can also be due to the extra wash/centrifugation step for the cryopreserved samples, with a cumulative extra loss of tumor cells. Unpublished in-house data from the development of the CTC enumeration protocol showed 2%–10% loss from each extra wash/centrifugation step.
In the clinical samples, a similar loss of tumor cells after cryopreservation was expected, however, this was not obvious. CTC numbers were both higher and lower in the cryopreserved samples compared with the fresh sample taken from the same individual at the same time. Therefore, paired fresh blood samples were examined in 64 patients (Fig. 2) and the results showed large variation in the number of CTCs—similar to results from other authors.8,17 Allard et al. showed that when detecting CTCs from blood samples with the CellSearch system, the difference between paired samples was within the expected statistical variation of detecting rare cells in the blood. Thus, the variation was not an analytical bias, but could be explained by the Poisson distribution. When rare cells circulate among millions of blood cells, it is statistically improbable that the CTCs are captured in similar amounts when blood samples are taken consecutively (see statistical calculations in supplementary data of Allard et al. 17 ). Thus, cryopreserved clinical samples must not only be prone to this biological variation in the blood sampling procedure, but also we expect the samples to be affected by the preanalytical variation, with a loss of cells (possibly 2%–10%) when the cryopreservation step is added to the protocol. However, it seems that our data set was too small to detect this expected preanalytical loss of CTCs in the clinical cryopreserved samples. Seven of the 17 cryopreserved samples still had a higher number of CTCs compared with the fresh sample.
Enumeration of CTCs is a prognostic tool, whereas characterization of CTCs could be a supplementary tool for tailor-made cancer therapy, for example, HER2 characterization in breast cancer patients. 3 Based on our data, we suggest that there is a loss of tumor cells after cryopreservation. We hypothesize that this is due to the extra washing steps. Hence, cryopreserved samples are presently not useful for CTC enumeration for prognostics. Existing cutoff values must be reevaluated to use for prognosis in cryopreserved samples.1,3
Importantly, the biomarker characterization of MCF-7 in this study did not appear to be affected by the freezing and thawing procedures. We have only tested the sustainability of a few CTC-specific biomarkers after cryopreservation for their use for immunocytological detection (CK, CD45, and EpCAM). The cold temperature and mechanical stress may have affected the epigenome or other phenotypical biomarkers, which we did not test in the present study. So, each biomarker of interest needs to be examined for CTC characterization. Today, the expected clinical use of CTCs is with characterization for therapy management. 18 So, as long as frozen tumor cells maintain their phenotypic and genotypic characteristics, cryopreservation is a helpful step in the laboratory setting, despite the possible cell loss. However, one has to keep in mind that clinical samples may have other viability features, compared with artificial CTCs. Cell culture cells might have a larger degree of resistance and immortality because of their long life span under culture conditions with passages occurring over decades. Thus, testing relevant biomarkers on cell culture cells after cryopreservation may not represent the effect of cryopreservation on clinical CTCs. In our clinical study, we did detect an expected amount of CTCs after cryopreservation, but perhaps the most invasive or certain CTCs or biomarkers are sensitive to freezing and will not be detected. This has to be kept in mind in CTC biomarker research on cryopreserved samples. In this study, the tool for biomarker evaluation was flow cytometry. It would strengthen the results if other methodologies were applied to confirm the status of the biomarkers of interest. Long-term storage (several years), which is necessary for biobanking, was not tested in the current study. However, such data exist from other cryopreservation applications 14 and may also be applicable for CTC analysis after we have confirmed 6 months of cryopreservation stability for tumor cells spiked in blood.
The cryopreservation protocol described in this study may be used with CTC retrieval systems other than the CytoTrack system, but this requires separate evaluation. Other methodologies for freezing may also be tested such as liquid nitrogen storage compared with −80°C storage as used in the present study. Due to the limited number of clinical specimens originating from one cancer type at one medical center, future studies should be performed incorporating other cancer types and other medical centers.
The general limitation in this study was that our clinical data set only contained 17 patients—a larger cohort may have shown an effect of cryopreservation on the number of CTCs. The Tumor cell line studies section could also have included a wider range of cell cultures and larger groups.
In conclusion, cryopreservation of CTCs may be an alternative to real-time testing with a recovery rate of tumor cells up to 90% and with no changes of tested phenotypic biomarkers, such as EpCAM and CK. Cryopreservation may facilitate the practicalities of larger clinical studies involving CTC characterization and establishment of biobanks for future studies.
Footnotes
Acknowledgments
The authors would like to thank all the patients who participated in this study. The study was funded by the EU seventh framework program and by Nordsjællands Hospitals Research Foundation. The CytoTrack® scanner was funded by Toyota-Fonden, Denmark.
Author Disclosure Statement
S.N., H.S., and M.T.N. were employed by CytoTrack Aps during the development and documentation of the cryopreservation protocol. Additional authors declare no conflicts of interests.