
Abstract
Brain banks continue to make a major contribution to the study of neurological and psychiatric disorders. The current complexity and scope of research heighten the need for well-characterized cases and the demand for larger cohorts and necessitate strategies, such as the establishment of bank networks based in regional areas. While individual brain banks have developed protocols that meet researchers' needs within the confines of resources and funding, to further promote collaboration, standardization and scientific validity and understanding of the current protocols of participating banks are required. A survey was sent to brain banks, identified by an Internet search, to investigate operational protocols, case characterization, cohort management, data collection, standardization, and degree of collaboration between banks. The majority of the 24 banks that returned the survey have been established for more than 20 years, and most are affiliated with a regional network. While prospective donor programs were the primary source of donation, the data collected on donors varied. Longitudinal information assists case characterization and enhances the analysis capabilities of research. However, acquiring this information depended on the availability of qualified staff. Respondents indicated a high level of importance for standardization, but only 8 of 24 considered this occurred between banks. Standard diagnostic criteria were not achieved in the classification of controls, and some banks relied on the researcher to indicate the criteria for classification of controls. Although the capacity to collaborate with other banks was indicated by 16 of 24 banks, this occurred infrequently. Engagement of all brain banks to participate toward a consensus of diagnostic tools, especially for controls, will strengthen collaboration.
Introduction
P
The operation of these banks is influenced by many factors, including scientific and technological advances, researchers requesting more complex and larger cohorts, and a global decline in autopsy rates. 7 Brain bank networks have developed in different continents (e.g., Australian Brain Bank Network and BrainNet Europe) to enhance collaborations, optimize protocols, and increase the ability to fill researchers' requests for tissue.
There have been a number of publications about how brain banks should be operated, the data sets that should be collected, tissue quality markers, and the ethical and legal framework within which they operate.8–11 Despite the work to date, more needs to be done to achieve a sustainable brain banking model.12,13 This study begins the dialogue and aims to assess what subject data brain banks are currently collecting and what standards are currently being used.
Methods
Participants
A contact list was identified by a Google search using the term “international brain banks.” This search generated links to the Registry of the International Brain Bank Network (IBBN), BrainNet Europe (BNE), and Australian Brain Bank Network (ABBN) websites. A preliminary list was collated from these sites. A follow-up Web search of the listed brain banks was conducted. The banks that had no accessible contact details on their Web page were excluded.
The final list included 60 brain banks from 19 countries. The Qualtrics© Web-based survey tool was used to invite participants to take part and develop the survey. The e-mail sent to participants contained a hyperlink to the survey. The survey was approved by The University of Sydney Human Research Ethics Committee (2013/425).
Survey design
The survey consisted of a maximum of 50 questions in six sections. Skip logic technology (Qualtrics, Provo, UT) was used to allow subsequent nonapplicable questions to be omitted. Survey sections were related to details on the operation of the brain bank, data collection and methods used, data analysis for classification, how control–cases are classified, how research cohorts are created, and opinions on standardization and collaboration of brain banks.
The design included a list of answers for selection with the inclusion of the option “other, please specify” and allowed for multiple answers. The section relating to the control classification criteria were free-text answers to allow the banks to provide a detailed response. Questions relating to the tissue quality markers were select and comment options. An additional comment option was provided as the last question.
Analysis
Survey data were collected using Qualtrics© software, version 2013 (Qualtrics). A report of the response frequency, percentage and mean for each question, and free text was generated. The data were further analyzed using SPSS version 22.0 (SPSS IBM).
Results
A total of 24 brain banks responded from 3 geographical regions (n = 10 [42%; United Kingdom/Europe], n = 5 [21%; Australasia], and n = 9 [37%; United States and Canada]). Although there was only an overall 40% response rate, there was representation of banks from multiple countries within these regions. The response rates of the banks per region were 10 of 20 (50%; United Kingdom/Europe), 5 of 10 (50%; Australasia), and 9 of 30 (30%; United States and Canada). The majority of the banks were established in the 1980s (n = 13, 54%) or 1990s (n = 8, 33%), with only 8% (n = 2) commencing operation since 2000.
Diagnostic groups collected
The research collection size ranged from 150 to 3000 cases. The mean number of diagnostic groups collected by each bank was four, with the most collection groups given as 12. Control tissue was collected by 92% (22/24) of banks. Figure 1 shows the diagnostic groups collected, and Figure 2 displays the exclusion criteria used.

Distribution of different diagnostic groups. Multiple responses permitted.
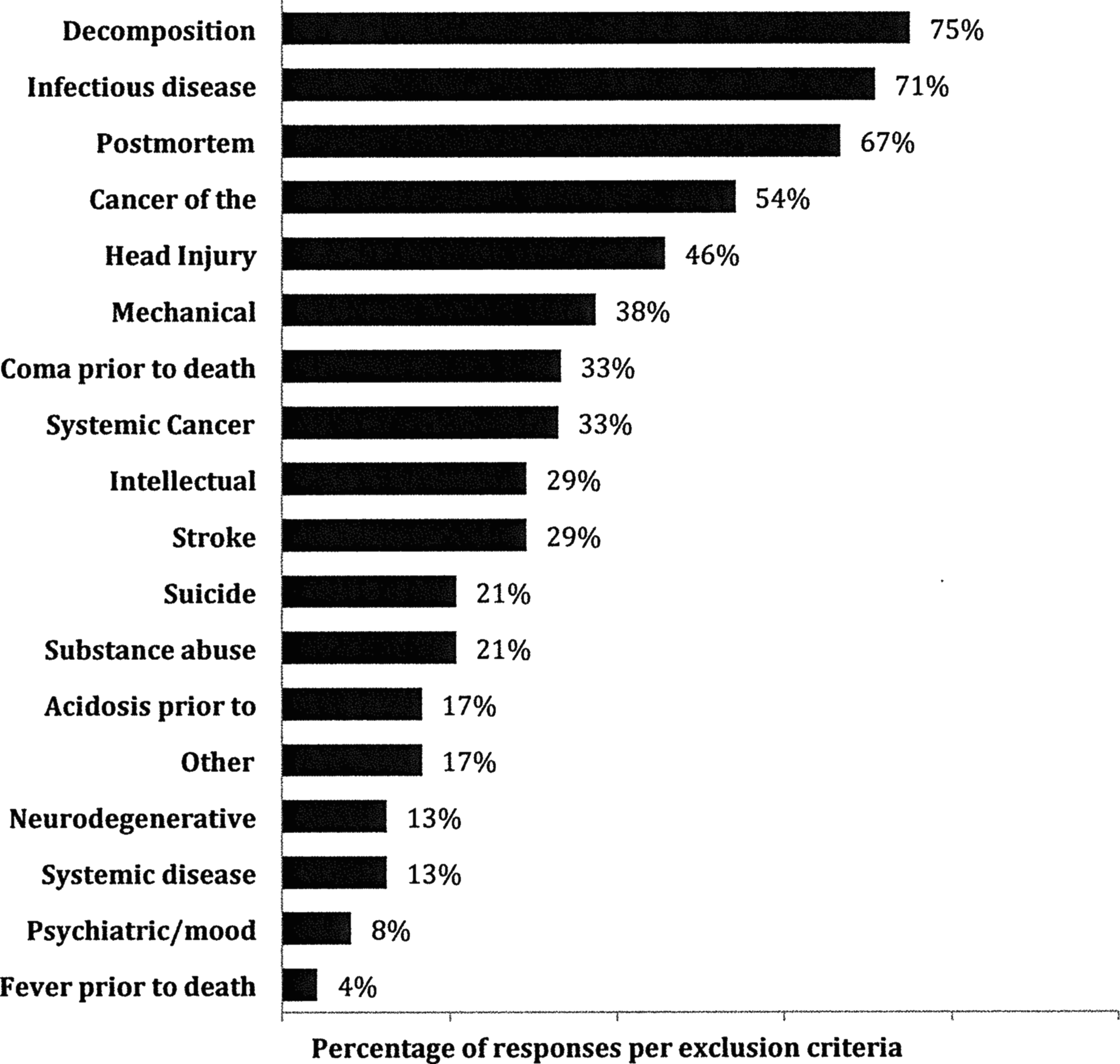
Variety of exclusion criteria applied by respondents (n = 24). Multiple responses were permitted.
Consent for donation
Seventy-nine percentage of banks have a preregistration donor program. The primary sources of donation were donor programs (58%) and autopsy centers (42%). The majority of banks required both the donor and next of kin (NOK) to consent (63%). Other sources of donation included family and specialist referrals.
Data collected
Donor information was primarily sourced from the treating physician or NOK via interviews or questionnaires. Preregistered donor programs not only obtained this from the donor but also contacted the NOK and treating physician. Other sources approached were the medical examiners, police, and research study coordinators.
Figure 3 outlines the donor information categories collected by the banks. The data collected within these categories varied, for example, within the demographics section (96%, 23/24), country of birth in (58%, 14/24), ethnicity (67%, 16/24), education (63%, 15/24), marital status (63%, 15/24), independence in self-care (50%, 12/24), handedness (50%, 12/24), activities in daily living (46%, 11/24), and diet and exercise (21%, 5/24). Of the brain banks that collect postmortem data, all record the cause of death and postmortem interval. Less often reported were systemic pathology (50%, 12/24), toxicology (29%, 7/24), and blood alcohol levels (17%, 4/24). Seventy-five percent (n = 18) of brain banks tested cognitive function, and of these, 78% (14/18) performed neuropsychology testing and 67% (12/18) used questionnaires.
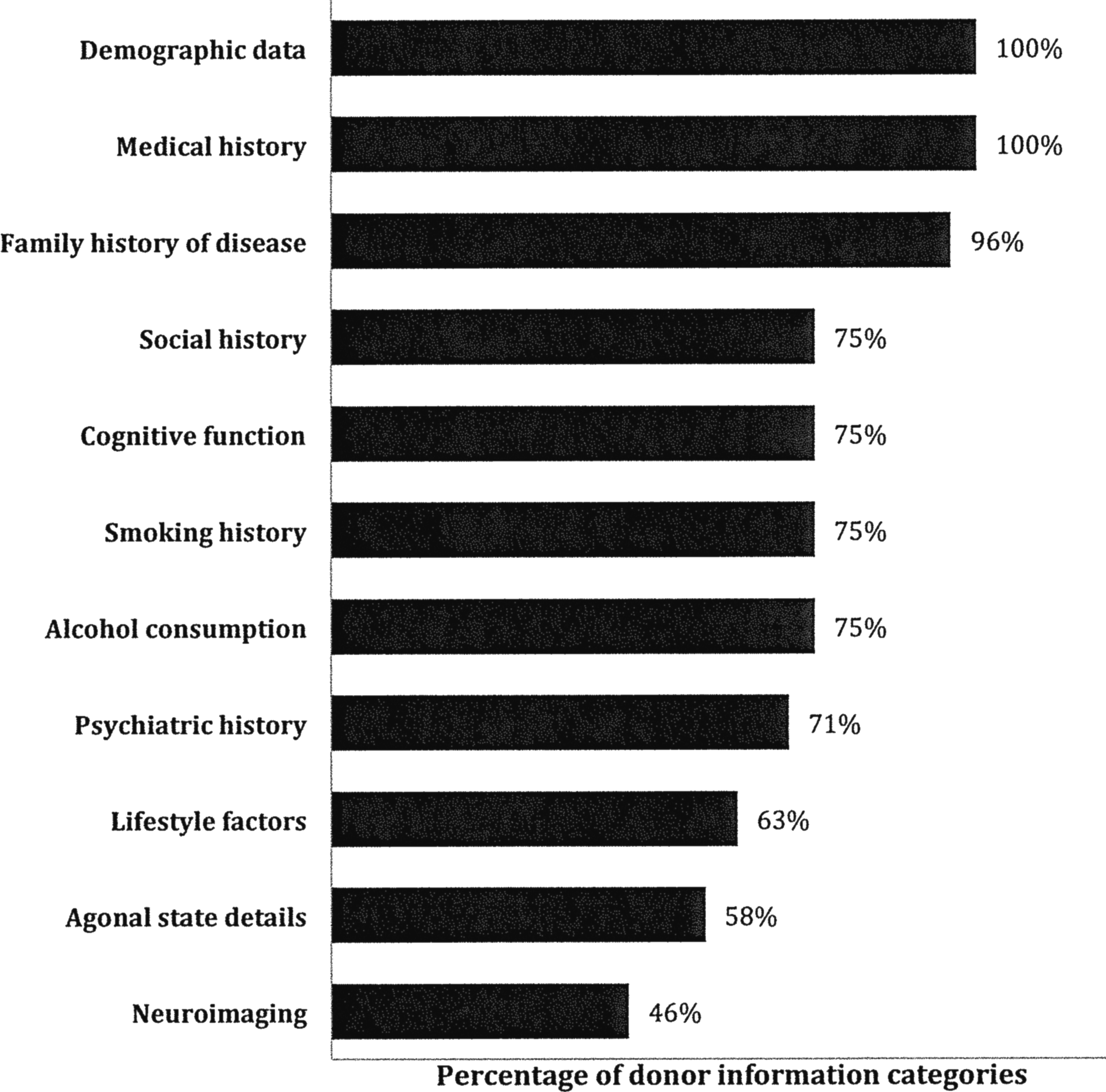
Frequency of data categories identified in classification protocols for the donor information.
Classification method
Consensus diagnosis by trained clinicians was the approach taken by 58% (14/24) of banks when classifying a donor. The positive use of validated instruments was selected by 13 of 19 (68%) who specified use of the following: Structured Clinical Interview for DSM-IV assessment, Diagnostic and Statistical Interview of Mental Health Disorders IV, Clinical Dementia Rating, Montreal Cognitive Assessment, Mini-Mental State Examination, Activities of Daily Living, and Uniform Data Set used by the US National Institute on Aging National Alzheimer's Coordinating Center.
The exclusive use of pathology reports in performing the characterization process occurred in n = 5 of 22 banks. Ninety percent (19/21) of banks apply the same diagnostic tools for classification of disease cases and controls.
Controls were defined by the absence of neurological and/or psychiatric illness and no neuropathological abnormalities, except age-related changes. Nineteen (79%) of the 24 banks specified the use of neuropathological criteria, including the Braak staging to define a control. 14 Suicide was an exclusion criterion for a control–case classification by 55% (12/22) of banks. Alcohol consumption was not considered in the classification of controls by half of the banks (12/23), and the majority did not consider smoking (87%, 20/23). In relation to whether other diagnostic categories could be used as “controls,” 43% (10/23) used other diagnostic groups as controls when creating cohorts for specific projects if the research design permitted.
Tissue quality markers
Figure 4 shows the results for each marker of tissue quality used to assess suitability for research. Further comments received (n = 9) on the specific cutoff values acceptable for provision of samples indicated for RIN a range >5 to >7 and pH range 5–7. Less often, banks use agonal factors (21%, 5/24) or perform protein analysis (8%, 2/24) to determine tissue quality. Furthermore, eight (33%) banks made comment that the cutoff values for tissue quality depended on the study design.

Types of tissue quality markers used by banks (n = 24). Multiple responses permitted.
Cohorts
When cohorts of cases and controls were provided, matching was determined more by the research project requirements or consideration of the above tissue quality measures (73%, 16/22) and less on a standardized age range or gender match (52%, 11/21). The most common reason for not being able to fulfill a request was the availability of the diagnostic group, followed by size of the request, and then the availability of the brain region of interest.
The majority of banks (74%, 17/23) indicated that collaboration with other banks was either very or extremely important. When questioned how often other banks were involved in filling a tissue request, only 13 banks responded positively (13/23) and indicated it was a rare (5/13) or occasional (6/13) occurrence. Two of the thirteen indicated collaboration occurred most of the time. A further two banks indicated that no collaboration occurred as tissue was only distributed to in-house researchers and formal collaborators. A standardized classification system among brain banks was also a high priority (70%, 16/23). Control–case classification was “not at all standardized” (26%, 6/23), “somewhat standardized” (39%, 9/23), or “standardized” (26%, 6/23). Only two banks indicated very (1/23) or extreme (1/23) standardization between banks.
Staffing
The number of full-time or equivalent staff members within the brain banks ranged from 0 to 15 (mean of 5 staff). Staff performing clinical assessment ranged from 0 to 10 (mean of 3), and the staff performing neuropathological assessment ranged from 1 to 6 (mean of 2). A follow-up open-ended question asking what professional qualification staff held showed 79% (18/23) referred to a neuropathologist performing the neuropathological assessment, and 29% (7/23) made reference to a psychiatrist performing the clinical assessment.
Discussion
The majority of the participating banks have been established for more than 20 years, and their collections focused on neurodegenerative diseases, psychiatric disorders, and control donors. Most have preregistered donor programs for recruitment, and these are essential to maintain donations with declining postmortem examination rates throughout the world.6,15
The main findings of this study relate to the view that standardization and collaboration, as well as confidence in the use of other banks' material, are highly important. In recent years, a number of large networks of brain banks have been established to foster collaborations, mainly in geographical regions, such as BrainNet Europe, UK Brain Banks Network, Australian Brain Bank Network, and more recently the NIH NeuroBioBank. These networks have worked toward understanding the challenges encountered in brain banking, such as the requirements of various governance bodies, ethical compliance, declining autopsy rates, and sustained funding and infrastructure.9,16–19
Individual brain banks have developed protocols that meet researchers' needs within the confines of resources and funding. As these banks combine in networks to establish common protocols, standard data collection procedures, and codes of conduct, challenges may arise from variation in processing and storage methods, as well as legal and ethical concerns.17,20,21 Over recent years, progress has been made by members of these networks to address the challenges of regulatory frameworks, optimizing tissue acquisition and storage and enhancing neuropathological protocols.2,8,15,18 Support from government bodies, such as the National Institutes of Health, in the review of their funded brain banks by the newly established NIH NeuroBioBank, is timely. 19 Other institutes within the NIH, such as the National Institute on Aging (NIA), through the individual NIA-funded Alzheimer's Disease Centers (ADCs) support an infrastructure and informatics network to encourage collaboration and serve as a resource for the neuroscience research community. 2
This study indicated the overall importance of standardization, although this was not presently achieved in the classification of controls. There were differences in the pathological criteria used, such as the range in the Braak staging from below two to a maximum of four, where allocation of the higher staged cases was dependent on the project. 14 The recent article by Nolan et al. comparing the pathological diagnosis of control–cases before and after 2007 demonstrates that the implementation of new methods may require a review of previous classification criteria. 22 Their study identifies the availability of new antibodies and changes in sampling protocols to aid the pathological review of control–cases, especially for the neurodegenerative disease cohorts.
Processing protocols and the assessment of brain tissue quality have been well documented for the past 30 years.3,10,21,23–27 Various methods are used to process frozen tissue, for example, liquid nitrogen, flash freezing, and plate freezing at −80°C,10,24 and dependent on the facility management and the available infrastructure. The majority of banks use postmortem interval as the main indicator of tissue quality. Only half of the banks use RNA integrity number (RIN) and brain pH routinely, and a fifth collect associated agonal state information. The lowest acceptable RIN value varied from 5 to 7, and brain pH ideally greater than 6 was used, consistent with previous studies.28,29 Adverse agonal conditions result in lower pH and RNA quality, and many individuals with neurological disorders have prolonged agonal periods compared with neurologically normal controls.25,30
Classification of controls based on both pathological and clinical criteria occurred in two thirds of banks with respect to neurological disease, substance use, and psychiatric conditions. Psychiatrists or neurologists affiliated with the banks assessed the majority of the cases using DSM-IV or Clinical Dementia Rating. Controls with a cause of death as suicide, a history of mild depression, or alcohol use were allocated to researchers by some of the banks. A review of research outcomes relating to these conditions using various techniques may be important in terms of defining controls.31,32 The transformation in research to combine both traditional neuropathology methods and genetic screening in the same project has heightened the importance of clinical data to enable comprehensive analysis.4,33
Standardized data collection needs to reflect the research being undertaken, but this is difficult to predict in the long term due to evolving nature of research techniques. Engaging with the researchers to understand their requirements and reviewing the feasibility of obtaining data will assist in the determination of a primary data set. Reviewing medical records or interviewing the treating physician is a primary source of data for brain banks. Therefore, engaging with this community to outline the effect of various factors on the quality of data collected may assist in improving the overall usefulness of material provided to researchers. However, acquiring this information depends on the regulatory environment and the availability of appropriately qualified and trained staff. New resources, such as the NIH National Institute of Neurological Disorders and Stroke common data elements site, (www.commondataelements.ninds.nih.gov/) have templates for clinical and biological data collection for a number of neurological diseases that will aid in harmonization of the information collected.
Conclusion
Despite a modest response rate, the participants in this survey reflect the overall distribution of current brain banks worldwide. The findings of our study highlight the difficulty in defining the ideal control and how current practice is reliant on researchers to define their criteria for a control population. Donor programs underpin the recruitment for many banks and can provide a unique avenue for longitudinal data that will enhance the future case characterization. The brain bank community is keen to form collaborations and enhances their current practices to improve pathological, phenotype and clinical characterization, standardization of processes, and the ability to supply the larger cohorts.
Footnotes
Acknowledgments
This research was supported by the National Institute on Alcohol Abuse and Alcoholism of the National Institutes of Health under award number R28 AA012725. The content is solely the responsibility of the authors and does not necessarily represent the official views of the National Institutes of Health.
Author Disclosure Statement
No conflicting financial interests exist.