
Abstract
Human heart valve allografts continue to represent almost perfect substitutes for heart valves. They have optimal hemodynamic characteristics and are highly resistant to infections. The first clinical use of allograft heart valves was as homovitals being transplanted after antibiotic incubation without any preservation. Since 1968, relatively standardized frozen cryopreservation (SFC) has been employed, including storage in vapor-phase liquid nitrogen. Disadvantages, particularly in pediatric patients, are limited availability due to organ scarcity, inability to grow, degeneration, immune response, and long-term failure. However, in contrast to alternative prosthetic or bioprosthetic heart valve replacements, they represent the best pediatric and juvenile replacement options for the pulmonary valve. Application of multiphoton imaging analysis for three-dimensional visualization of elastin and collagen by induction of autofluorescence without chemical fixation, embedding, and staining has revealed partial destruction of elastic and collagenous matrix in SFC valves. As the overall amount of collagen and elastin remains unchanged, the observed destruction is attributed to freezing-induced extracellular matrix damages due to ice crystal formation during SFC. The objective of this review is an assessment of current allograft preservation methods and the potential of novel preservation techniques to avoid ice formation with accompanied better long-term function.
Historical Development
Anatomical basics
S

Histology of the pulmonary valve (Movat pentachrome staining): a, atrial aspect; f, pars fibrosa; s, pars spongiosa; and v, pars ventricularis.
The cusps are covered with a confluent endothelial monolayer. Innervation and nutritional support of valve tissue are achieved by vasa vasorum in the root and by diffusion in the leaflet region.1,2
First clinical applications of allografts
Transplantation of human allogeneic aortic and pulmonary heart valves, known as homografts or allografts, started over 50 years ago. 3 They revealed exceptionally good initial hemodynamics, minimal thromboembolic events without anticoagulation, and better resistance to endocarditis compared with either bioprosthetic or mechanical valves.4,5 Allografts have especially benefited children with congenital heart disease. They have also been used in young adults, women of childbearing age, older patients with poor medical compliance, and in adult patients who requested them due to awareness of the potential longevity of these valves.
Initially, the heart valves were procured aseptically, but not cryopreserved or treated otherwise. They were kept in nutrient solutions, with or without antibiotics, and transplanted as soon as possible, as so-called homovitals.6–8 Due to the logistic issues associated with having the right-sized valve available for patients when they needed them, grafts were subsequently banked by storage at 4°C in a tissue culture medium with antibiotics for up to 6 weeks before implantation. 9 Frozen cryopreservation with dimethyl sulfoxide (DMSO) and fetal bovine serum was introduced for longer-term storage and to allow more time for donor screening and microbiological assessment, including virology. 10 There was also significant work performed on ways to minimize microbial contaminants on the heart valves. Beginning in the 1960s, experimentation in sterilization and alternative storage methods was performed.11–13 Alternative storage techniques included freeze-drying and flash-freezing by submersion in liquid nitrogen, followed by frozen storage at −70°C. Barratt-Boyes et al. 14 reported that flash-freezing resulted in poor clinical results and laboratory evidence of altered biomaterial properties. Merin and McGoon 15 obtained poor results with frozen irradiated valves. Concerns about disease transmission led to aggressive sterilization techniques, including highly concentrated antibiotic incubation, irradiation, and chemical pretreatment. As early as 1966, Hudson 12 had documented the use of radiation methods for heart valve sterilization. The studies of Heimbecker et al. 11 also demonstrated that pretreatment with gamma radiation or beta-propiolactone markedly diminished the in vivo durability of valves. The use of radiation was subsequently confirmed by others to have deleterious effects on valve performance and was abandoned. 16 Kosek et al. 17 recognized the damaging effects of such sterilization techniques and suggested that the use of fresh (refrigerated) valve grafts was clinically superior. Subsequently, aseptic heart valve procurement was combined with antibiotic treatment before either refrigeration at 4°C (less than 6 weeks) or frozen cryopreserved storage below −135°C, and these emerged as the methods to minimize microbial contamination and heart valve storage. 18 For more than 20 years, frozen cryopreservation after antibiotic treatment with storage below −135°C in vapor-phase nitrogen has been the choice for preservation of human heart valves. 19 Both refrigerated and frozen cryopreserved methods resulted in allografts containing viable fibroblasts at the time of transplant.
Standardized Frozen Cryopreservation
The long-term storage and stabilization of viable cells and tissues require the application of cryobiology.20,21 This may be defined as the effect of temperatures below the normal physiological ranges upon biological systems. However, simply freezing cells or tissues results in dead cells and loss of functions dependent upon cells. In 1949, Polge et al. 22 discovered the cryoprotective properties of glycerol for biological material during freezing. Ten years later, Lovelock and Bishop 23 discovered that DMSO is also a cryoprotectant. Since the discovery of these first cryoprotectants, methods for cryopreservation of many biological materials have been established and many other cryoprotectants have been identified. Cryoprotectants and their mechanism of action have been demonstrated in a number of excellent studies.24–26
Currently standardized frozen cryopreservation (SFC) of heart valves for clinical applications is performed with minor variations as previously described 27 in 10% dimethyl sulfoxide (DMSO) in a culture medium with 10% fetal bovine serum and controlled-rate frozen at −1°C/min to below −40°C. The valves are then placed and stored in the vapor phase of a liquid nitrogen storage freezer at or below −135°C. Immediately before implantation, valves are removed from their storage freezer and rapidly thawed in a warm water bath, followed by extensive rinsing to remove as much DMSO as possible.
In the last century, cryopreserved human heart valves were used in ∼20% of the tissue heart valve procedures performed annually.28–30 They are currently less utilized because of new xenogeneic valves, which are impacting aortic valve utilization, and because of failures in young patients, 31 particularly infants. 32 The pathophysiology of allograft heart valve failure is not fully understood.33,34 A variety of reasons for pediatric allograft heart valve failure were discussed in the past and most investigators have emphasized immunologic issues.35,36 We have previously proposed the hypothesis that the rapid deterioration observed in some allograft heart valve recipients may also be due to disruptive interstitial ice damage that occurs during cryopreservation, resulting in an accelerated valve degeneration and calcification upon implantation.18,37
Potential Limitations of SFC Heart Valves
Structural degeneration and calcification
Human aortic or pulmonary valves are obtained from cadavers or from diseased hearts, removed during transplantation of a replacement heart, and then transplanted from one individual to another. They are preserved without the chemical cross-linking employed for xenogeneic, porcine, and bovine heart valves. Variable loss of viable cells (endothelial and interstitial cells) occurs before and after procurement due to ischemia, the cryopreservation method employed, and damage due to handling. The tissue structure of SFC heart valves demonstrates some disruption, but routine histopathology methodologies are not sufficient if a detailed tissue state characterization is required. Multiphoton-excited autofluorescence and second-harmonic generation (SHG) microscopy are powerful imaging tools that provide the unique ability to detect deep tissue cells and extracellular matrix (ECM) components such as elastic and collagenous fibers in situ without the need for any fixation or invasive processing. Schenke-Layland et al. 38 demonstrated that cryopreserved valve leaflets had substantial ultrastructural deterioration and disintegration of most collagenous structures by laser-induced autofluorescence imaging and, in contrast to fresh leaflets, second-harmonic signal generation was not inducible. As in chemically cross-linked bioprosthetic valves, the ECM is incapable of remodeling in the absence of viable interstitial cells. So, implanting SFC valves with damaged ECM is obviously not the best way to go since the quality of the valve will only get worse not better.
Furthermore, dead cells and damaged ECM fibers, both collagen and elastin, can serve as nucleation sites for calcium phosphate minerals. 39 Calcification is accelerated in young patients, probably because of age-related biochemical differences in calcium/phosphate metabolism. 1
Immune response
Immune reaction to allogeneic heart valves was originally proposed as a mechanism of allograft destruction in pediatric patients by Clarke et al. 40 Fueled by further clinical studies31,32 showing accelerated degeneration in very young patients, it became accepted that allogeneic heart valves elicit a host-dependent immune response against the implanted tissue.41,42 Animal studies suggested a role of T cell-mediated inflammation (Legare). 35 Most of the patients with cryopreserved allografts developed humoral antibodies against human leukocyte antigen (HLA), a specific antibody against transplanted tissue.43–45 The presence of donor-derived dendritic cells in allogeneic tissue has been demonstrated to play an important role in the immune activation of recipient by direct antigen presentation. 46 Many reports have shown that the absence of dendritic cells (antigen-presenting cells) in cryopreserved valve allografts is compensated by the preservation of endothelial cells expressing HLA class II molecules, which may be responsible for a specific immune response against valve tissue. 47 This complex reaction represents not only a humoral or cellular immunologic response but also has graft functional consequences. Mitchell et al. 34 could not demonstrate an antibody-mediated injury in explanted allografts showing only mild to moderate mononuclear inflammatory cell infiltrate comprising T cells and macrophages in the valvular tissue. A state of immunological tolerance with induced T cell anergy of the valve interstitial cells on the host had been suggested by Batten et al. 48 Rajani et al. 49 found multiple foci of inflammatory cells of either T or B lymphocytes in valves from infants who had premature degeneration in less than 8 months, suggesting a rejection. Some reports with long-term follow-up suggested an HLA-induced alloreactivity with consecutive valve tissue deterioration.50,51 Christenson et al. 52 showed accelerated degeneration and calcification of cryopreserved allografts in children with ABO blood type incompatibility, suggesting rejection.
Decellularization has been proposed as a promising method to diminish or even abolish allograft antigenicity and thus avoid the immune response.53–56 Several methods have been developed to produce completely acellular heart valve tissue matrices using multistep detergent–enzymatic extraction, 57 Triton detergent, 58 trypsin/ethylenediaminetetraacetic acid, 59 and deoxicolic acid, 60 as well as the RNAse and DNAse procedure. 55 Meyer et al. 61 concluded that decellularization significantly reduces the cellular and humoral immune response to allograft tissue in the rats. Zehr et al. 62 and Bechtel et al. 63 demonstrated that the SynerGraft™ decellularization technology successfully removed antigens from an aortic and pulmonary allograft. Another protocol for successful heart valve decellularization, using sodium dodecyl sulfate (SDS) in the presence of protease inhibitors, was applied by Booth et al. 64 da Costa et al. 65 revealed a lower immunogenicity of decellularized allografts than cryopreserved allografts with stable hemodynamic performance up to 18 months postoperatively. They compared the immunological and echocardiographic data of decellularized (AutoTissue Ltd™, Berlin, Germany) versus cryopreserved allografts used for right ventricular outflow tract (RVOT) reconstruction during Ross operation.
The results of the longest follow-up study on decellularized pulmonary SynerGraft allografts in the Ross procedure did not show a significant improvement in terms of pressure gradients and structural deterioration compared with conventional nondecellularized allografts. These clinical observations did not solve the controversial question on whether the remaining allogeneic cells or potentially altered ECM is the cause of valve degeneration. Sodium dodecyl sulfate decellularization can be an effective alternative to decrease immunogenicity of decellularized allografts with significantly reduced numbers of epitopes for both HLA class I and II. 66
Bovine serum
Bovine serum is commonly used in cryopreservation of tissues, including cardiovascular tissues. However, bovine serum contains variable amounts of stimulatory and inhibitory molecules with unpredictable effects on cells and most significantly carries a risk of product contamination with bovine-derived infectious agents. Whereas most agents do not cross barriers between species, there have been instances where a prion has crossed over and infected a new species.67,68 The FDA guidelines for production and handling (Committee for Veterinary Medicinal Products, 2001; Food and Drug Administration, 2001) minimize the risk of transmission of bovine disease agents to humans.
Furthermore, Nakayama et al. 69 demonstrated that bovine serum might not be necessary for maintenance of cell viability in cryopreserved aortic valve tissues. Campbell and Brockbank 70 have previously demonstrated that bovine serum can be removed from the cryopreservation procedure without disturbance of viability using adherent myofibroblast cell cultures, providing that appropriate cryoprotectant formulation validation is performed. Further studies compared serum-free cryopreservation with cryopreservation of the heart valve utilizing bovine serum. 71 The results of this study demonstrated that fetal bovine serum can be removed from heart valve processing without significant impact on cell viability, tissue structure, or biomechanical properties. Accordingly, there is no justification for using fetal bovine serum for heart valve cryopreservation.
Ice crystal formation and freezing artifacts
A variety of reasons for allograft heart valve deterioration were discussed in the past. Brockbank et al. 72 have hypothesized that the rapid failure of the valve allograft is due to destructive interstitial ice damage occurring during cryopreservation. However, the direct impact of ice crystals on the ECM, elastic, and collagenous fibers in valve tissue cannot be displayed unequivocally using conventional visualization techniques.
Direct alterations of ECM (elastic and collagenous fibers) due to ice formation by SFC have been demonstrated by multiphoton-induced autofluorescence and second-harmonic generated imaging.38,73 These techniques demonstrated that SFC, when compared with fresh or vitrified tissues, caused more destruction of normal ECM structure, which might have contributed to eventual graft dysfunction. More recently, RAMAN spectroscopy also showed collagen damage in the SFC valves compared with native valve tissue. 74
Novel Developments
Decellularized allografts and new homovitals
Cryopreserved valve homografts have been the conduits of choice used over decades for RVOT reconstruction. 28 These valves have high resistance to infection and provide excellent hemodynamic properties. However, in the majority of reports, all patients suffered from some conduit valve regurgitation and, additionally, the homografts calcified. 75 In children and young adults, an accelerated degeneration was observed that was attributed to high immunologic competence. 76
Heart valve tissue engineering represents an upcoming alternative method to create viable, nonimmunogenic, and biologically active grafts 77 (Fig. 2).
Immunohistochemical micrographs from explants. Massive leukocyte infiltration of the CPV wall
There is strong evidence that removal of cells and cellular debris (>99%) significantly decreases immunologic responses in valve recipients. 65 In a previous study, extensive remodeling of the decellularized scaffolds in vivo by repopulation of autologous cells after implantation was demonstrated. 78 Moreover, these valves did not degenerate in the sheep model and demonstrated excellent hemodynamics.
In another study, 79 human pulmonary valve allografts were harvested under sterile conditions from mostly adult cadavers and transplant patients. Donors were tested for transmissible diseases (AIDS, hepatitis, syphilis, tuberculosis). Warm ischemic time was up to 6 hours, and during the decellularization, pulmonary allografts were treated under shaking conditions with a solution of 0.5% sodium deoxycholate (Sigma) and 0.5% sodium dodecyl sulfate (Carl Roth) for 36 hours at room temperature. Thereafter, homografts were washed in NaCl 0.9% solution and stored at 4°C (up to 3 weeks) until implantation. Fresh pulmonary homograft valves treated with this decellularization method showed very promising early results without development of relevant gradients, valve insufficiency, or necessary explantations for up to 5 years. Neumann et al. 80 have demonstrated that decellularization can provide a basis for autologous regeneration as no significant activation of the cellular immune system was observed during short-term follow-up (36 months). They have hypothesized that it occurred during a period of autologous colonization of the valves. Since early graft failure is predominately a cell-mediated process, the observed lack of early systemic cellular immune response is an important and encouraging finding.
SynerGraft technology and autologous tissue-engineered heart valves
The SynerGraft (CryoLife, Inc., Kennesaw, GA) valve, which was developed as an acellular (nonglutaraldehyde-fixed) porcine aortic prosthetic valve, 81 is the prototype of the decellularized cryopreserved valves used in the Ross procedure (Fig. 3).

CryoLife, Inc., data on file, including interim data collected from the CryoValve SG postclearance study through December 31, 2011. Reproduced with permission from CryoLife company.
In the SynerGraft process, the explanted valve or allograft is treated with antibiotic solution, then decellularized by hypotonic lysis, nuclease digestion, and sequential washing, and at the end cryopreserved and stored. CryoValve SynerGraft has been tested in many clinical studies. In the previous clinical study, three children implanted with decellularized porcine heart valve SynerGraft died because of valve rupture or early severe degeneration. Postmortem findings showed strong inflammatory response in the xenogeneic collagen matrix of the SynerGraft valve and concurrently the grafts showed poor cellularization and fibrosis. 82 Comparing a new CryoValve SynerGraft decellularized pulmonary allograft with a standard cryopreserved allograft (SCA) in patients aged 4 months to 58 years, a similar rate of reoperation in patients with Ross procedure and no significantly different hemodynamic results from SCA were observed. 83 Another decellularized porcine pulmonary heart valve, Matrix P (AutoTissue GmbH), has been tested for the reconstruction of the RVOT during repair of congenital or acquired heart disease. This valve is also nonglutaraldehyde-fixed and stored in antibiotic solution at 4°C. In a study involving 93 pediatric patients undergoing RVOT reconstruction using Matrix P and Matrix P Plus valves, conduit failure was reported in 35.5% of the patients and conduit dysfunction in 29%. 84 Failure occurred due to either dilation or stenosis of the graft, and histological analysis showed inflammation and poor cellularization. Another study with Matrix P valve implanted in 61 patients (age 9 days to 50 years) with congenital heart disease demonstrated an advantage in an intermediate-term performance. 85 The recent results from many clinical reports are more or less conflicting and call for further testing. 86
The availability of healthy homologous donor valves is limited and xenogeneic materials are associated with infectious and immunologic risks. To address such limitations, biodegradable synthetic materials have been successfully used for the creation of living autologous tissue-engineered heart valves (TEHVs) in vitro. In the recent study, 87 a decellularized TEHV (dTEHV), based on biodegradable synthetic materials and vascular-derived cells, was successfully introduced by creating a potential off-the-shelf starter matrix for guided tissue regeneration. In a nonhuman primate model after minimally invasive delivery into the orthotopic pulmonary position, an 8-week follow-up has been implemented. The results showed mild–moderate valvular insufficiency and relative leaflet shortening. However, in comparison with the decellularized human native heart valve, control dTEHVs showed remarkable rapid cellular repopulation. Given this in situ remodeling capacity, it may be postulated that human cell-derived, bioengineered decellularized materials represent a promising and clinically relevant starter matrix for heart valve tissue engineering.
Vitrification and ice-free cryopreservation
The hypothesis of a rapid deterioration of standard cryopreserved heart valve allografts due to interstitial ice damage led to development of a cardiovascular tissue preservation method that avoided ice formation by promoting vitrification. In the evolution of this method of glass formation, initially a vitrification protocol using 55% cryoprotectant formulations (VS55) and storage at −135°C was applied. 88 This protocol resulted in excellent avoidance of ice formation with retention of cell viability and matrix integrity, provided that the sample size and the geometry permitted rapid cooling and warming. During slow rewarming, ice formation was demonstrated. Brockbank et al. 27 discovered subsequently that an 83% cryoprotectant formulation could be stored at warmer temperatures (−80°C) than the 55% solution without risk of ice formation and called it ice-free cryopreservation (IFC). In brief, harvested valves will be decontaminated overnight at 4°C using antibiotics. IFC will be achieved by adding an 83%, 12.6 molar cryoprotectant vitrification formulation (VS83) in EuroCollins solution base, containing 4.65 mol/L formamide, 4.65 mol/L dimethyl sulfoxide, and 3.31 mol/L 1,2-propanediol. They will be subsequently placed in sterile polyethylene bags containing 70–80 mL of VS83, evacuated of air, heat-sealed, and cooled at 5.4°C/min to −80°C in a precooled bath of 2-methylbutane. The bagged valves will be eventually stored at −80°C. Storage at −80°C avoids risk of tissue cracking that may occur at a colder storage temperature because the solution is not quite solid and still deforms under pressure. In a sheep study with follow-up of 7 months (equivalent to 5 years in a patient), the native, standard cryopreserved, and IFC valves were analyzed (Fig. 4).

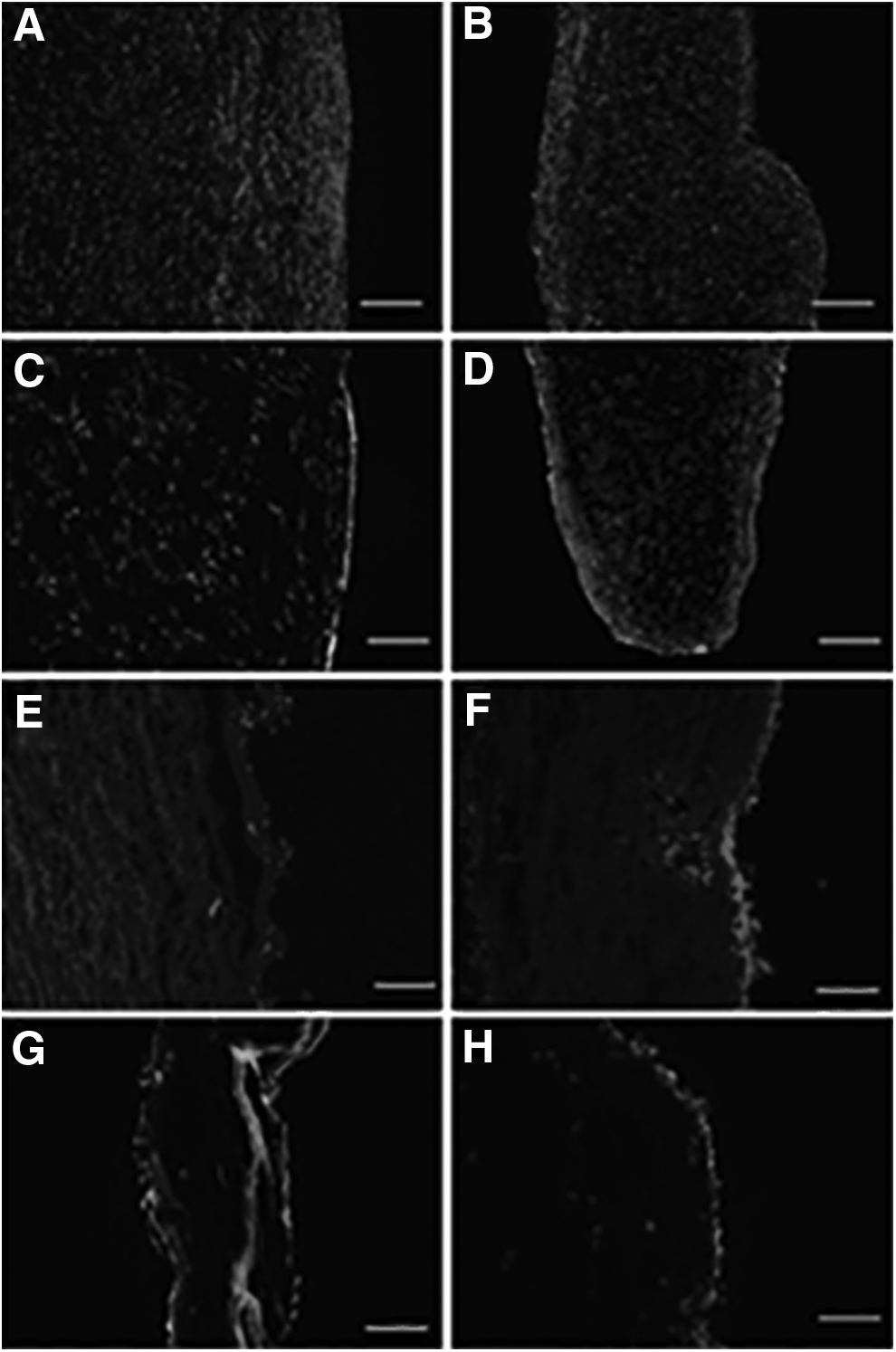
Histology of explanted pulmonary valves 7 months after implantation. FC valves are depicted in
Histology revealed leaflet thickening, chronic inflammatory cell infiltrates with CD3+ T cells in standard cryopreserved valves, but not in the IFC group. Multiphoton-induced autofluorescence imaging and SHG revealed reduced elastin autofluorescence within extracellular structures in conventional cryopreserved valve tissue in contrast to well-preserved ECM in the IFC group 89 (Fig. 5).
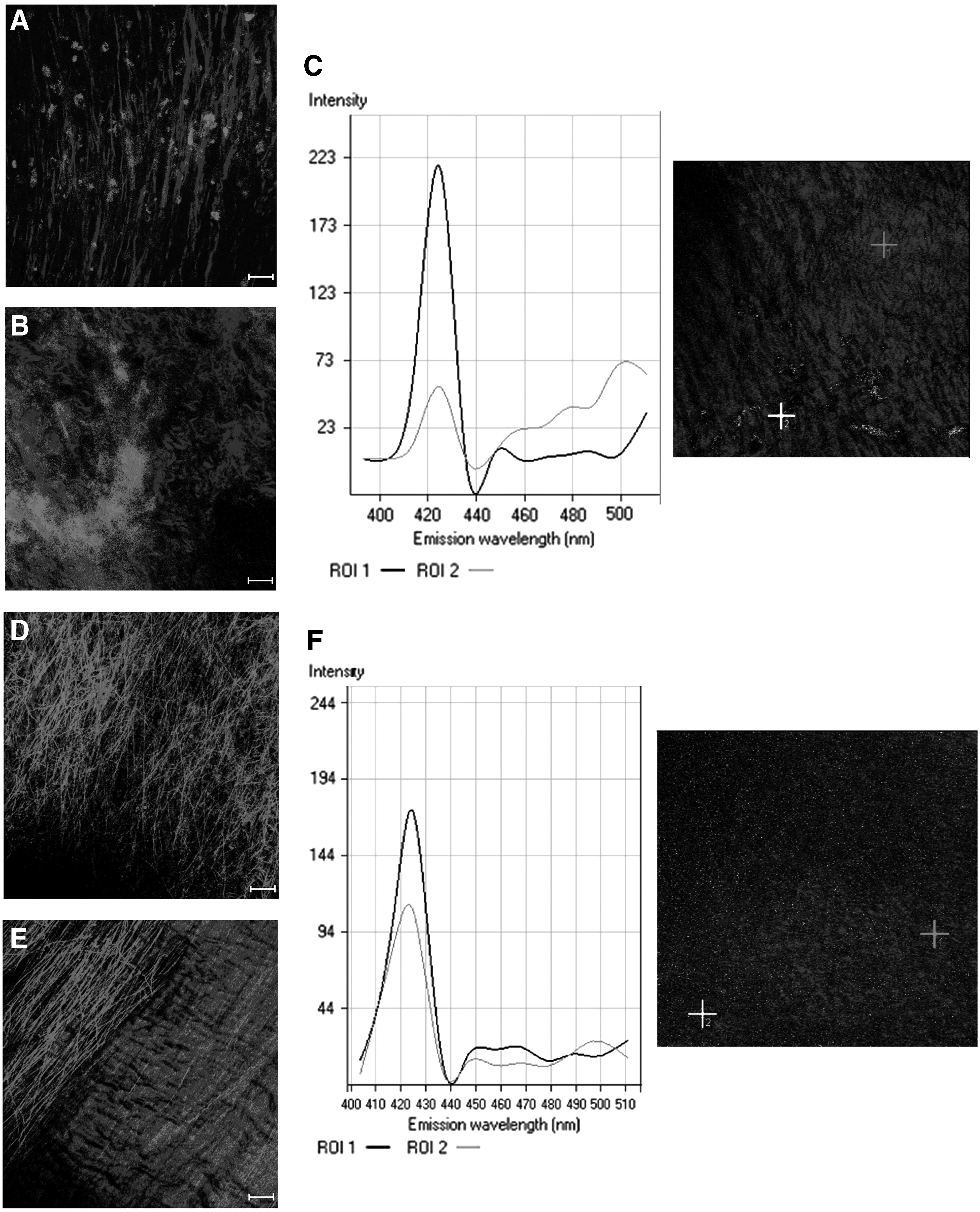
Multiphoton laser scanning microscopy of leaflet structures after 7 months in vivo. Two-photon images of SFC
These data are similar to previously published in vitro reports.38,73 Another animal study with sheep heart valves stored in the 83% cryoprotectant formulation at −80°C showed significantly reduced cell viability in the valve leaflets. 90 The observation that explanted vitrified valves were nearly devoid of active immune cells suggested that similar effect to decellularization was accomplished by IFC method. Concerns that the apparent benefits of vitrification were due to toxic cryoprotectant residuals were dismissed by demonstration that cells cultured with these tissues survived. It is hypothesized that this vitrification method is modifying or masking tissue signals perceived by responder cells. These signals representing a damage-associated molecular pattern can initiate and perpetuate immune response.
Preliminary scanning electron microscopic studies indicated that heart valve tissues exposed to 83% cryoprotectant formulation were empty of endothelial cells. 91 These results indicate that VS83-preserved heart valves can be stored and transported at temperatures in the vicinity of −80°C with retention of ECM integrity and material properties. The major difference between the traditional cryopreservation methods is simplification of the cooling and warming methods, and no liquid nitrogen is required. Storage can be in vapor-phase nitrogen, if you wish, or above the glass transition temperature (i.e., −80°C). This makes storage and transport much simpler and less expensive than traditional frozen heart valves.
Current Limitations
Formamide (FORM) is a widely used industrial solvent and its developmental toxicity in laboratory species has been reported previously. The known developmental toxicity NOAEL (No Observed Adverse Effect Level) is 50 mg/kg/day and LOAEL (Lowest Observed Adverse Effect Level) is 100 mg/kg/day. 21 Gross calculations estimate an amount of maximum 600 mg formamide per heart valve at the time of preservation and before washing. However, preliminary results indicate that formamide content is reduced to subcritical concentrations after two wash cycles (unpublished results Biermann et al.).
Conclusion
This review summarizes how much has been learned about heart valve allograft preservation over the past 50 years. Frozen cryopreserved heart valves have indeed been used for many years, and there may be different effects of cryopreservation on valves from different species, but no one has yet compared valves from humans and animals in the same study.
There are controversial discussions whether remaining allogeneic cells or potentially altered ECM contributed to the allograft degeneration. The literature also shows significant concerns about immune responses and inflammatory cell infiltrates in explants in studies with both large animal models and patients. This has led to the development of decellularized heart valves. It is possible that an IFC process is an alternative to both cryopreservation methods of freezing and decellularization since it minimizes the immune reaction to allogeneic valves in sheep implant studies. There are many questions still to be answered about this new method of preserving heart valves, including the effect of the process on tissue hemocompatibility, biocompatibility, immunogenicity, and concerns regarding residual cryoprotectants. On the other hand, with advances in tissue engineering, a new human cell-derived, bioengineered, decellularized valve graft will continue to be developed.
Footnotes
Author Disclosure Statement
No conflicting financial interests exist.