
Abstract
Background:
High-quality biospecimen collection from consented patients is crucial for cancer research activities. Patients' attitudes and willingness toward specimen donation influence high-quality biospecimen collection for cancer research activities.
Methods:
We carried out a cross-sectional study among randomly selected patients from 11 cancer departments of Tianjin Medical University Cancer Institute and Hospital between August 2014 and August 2015. A total of 784 patients were included to complete a 30-item self-administered survey. We evaluated the patients' willingness to consider providing leftover samples and additional samples for cancer research purposes.
Results:
Among 784 patients, 683 (87.1%) and 653 (83.3%) were willing to donate leftover tissue and surplus blood after diagnosis, respectively. Six hundred thirty-one (80.5%) were favorably disposed to consider donating both tissue and blood samples for future cancer research. Female patients showed less willingness to donate biospecimens or related clinical data for research. First-hospitalized or older patients were less willing to provide leftover biospecimens or additional blood samples or even clinical data for research. By contrast, patients with a higher education level were more likely to donate leftover tissues after biopsy or surgery for research activities.
Conclusions:
Most Chinese cancer patients were willing to consider donating blood and tissue samples for cancer research. Several factors, including age, gender, first hospitalization, and education level, can influence their willingness to donate biospecimens. We need to provide proper education to increase understanding of patients in biobanking activities.
Impact:
This study provides novel empirical data on the likelihood of donating surplus and additional biospecimens and clinical health information among Chinese cancer patients.
Introduction
H
Disease-specific biobanks have been developed in several countries, including the United States, the United Kingdom, Australia, and most European countries. 1 Since 2003, Tianjin Medical University Cancer Institute and Hospital (TMUCIH), as one of the largest cancer centers in China, has established an international standardized cancer biobank to respond to the challenges of cancer. This biobank is a major resource for investigators at TMUCHI and across China.4–6 However, some ethical and legal issues exist, such as attitudes and perceptions of patients toward biobanks, which could present serious obstacles for international medical research efforts in China. 2 Participation in a biobank involves risks. A host of ethical concerns are raised when disease-related genes are identified in those samples, which may alter the risk of developing certain conditions. The results of genetic research can cause great psychological pressure on donors about future genetic information, which may be used against them, resulting in discrimination due to their health situation and that of their children. Moreover, if studies reveal people who are genetically inclined to develop certain diseases, and this information is disclosed to insurance companies or prospective employers, it could harm patients' access to insurance and employment and cause considerable upheaval in their lives. 3 Prior research suggested that a number of demographic factors, including age, sex, education level, and level of trust of medical institutes, are associated with patients' willingness to donate biospecimens for research.2,4–6 These concerns all hinder the development of biobank and translational research.
This study aims to assess whether patients would consider donating leftover samples, additional samples, and clinical data to biobanks for research and to evaluate the factors that are associated with collection of samples and clinical data. Understanding patients' attitudes may help us improve strategies to further increase patients' understanding to consent to research biopsies.
Methods
Survey cohort
We conducted a cross-sectional study on attitudes and perceptions of patients toward donating human biospecimens for research purposes. Participants were enrolled from 11 cancer departments of TMUCIH. One of the top cancer centers in China, TMUCIH is located in Tianjin, North China, which is one of four Chinese municipalities. The patients who received treatment at TMUCIH came not only from Tianjin but also from all over north China. In the survey, qualified respondents must meet the following criteria: (1) Chinese northern citizen; (2) diagnosed with cancer; and (3) age greater than or equal to 18 years old. Between August 2014 and August 2015, eligible participants were invited to attend face-to-face interviews in an independent unit without any other patients or medical personnel involved. We ensured the privacy of patients and high-quality information collection. Research staff conducted comprehensive training with investigators on the study objective, criteria of participation, data collection, privacy protection of participants, and the long-term contribution to society.
Before the interview, we had informed participants of not only the purpose of our survey and the value of sample donation for cancer research but also the privacy risks of participating in our biobank and the methods we used to protect their personal information. Well-trained investigators interviewed 811 patients and 27 of them declined to participate in the survey. Finally, a total of 784 individuals were included in the study. Data collection and data processing activities proceeded almost simultaneously.
Study questionnaire
The questionnaire was designed with reference to previous related studies,4–8 which involved demographic information and other correlative items, such as donating human biospecimens. Three reviewers independently evaluated the questionnaire and then reached a consensus on all the items to be investigated. The questionnaire was first administered in a pilot survey among 50 breast cancer patients to ensure patients' understanding of the survey items and to obtain clear answers. After revision and improvement, the final questionnaire comprised two parts with various topics (Fig. 1). Chinese is the primary language of the questionnaire, with a matching English version. One section was entitled “Survey of Patient's General Characteristics” and the other section surveys public attitudes toward donating human biospecimens for research purposes. Collected information included age, sex, race, education, marital status, insurance, cancer family history, benign tumor history, prior clinical trial participation, prior biopsy, medical workers among the family members, residence, mental status, and first hospitalization. These variables were used to analyze the relationship between sociodemographic factors and willingness to donate biospecimens.
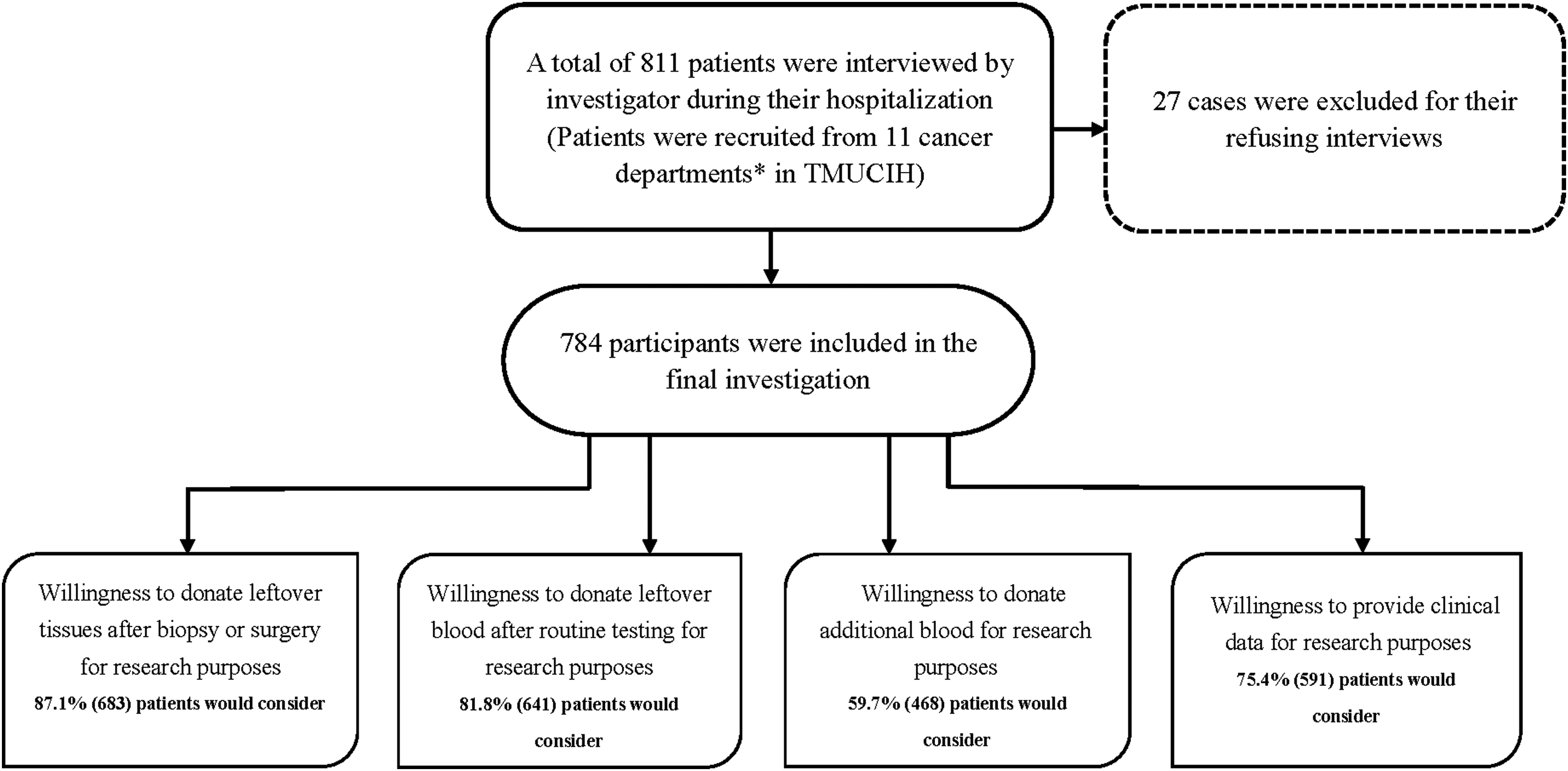
A cross-sectional survey cohort. *Eleven cancer departments, including Department of Maxillary Facial and Otorhinolaryngology, Department of Gynecological Cancer, Department of Hepatobiliary Cancer, Department of Bone and Soft Tissue Tumor, Department of Lung Cancer, Department of Colorectal Cancer, Department of Urogenital Oncology, Department of Breast Cancer, Department of Esophageal Cancer, Department of Gastroenterological Cancer, and Department of Pancreatic Cancer. TMUCIH, Tianjin Medical University Cancer Institute and Hospital.
Survey of patients' opinions regarding donation of biospecimens for research
To evaluate a patient's attitudes and willingness to participate in biospecimen research, we inquired about seven items: (1) prior biopsy and details concerning sites, (2) willingness to donate leftover samples after biopsy, (3) willingness to donate leftover samples after pathological examination, (4) willingness to donate leftover blood samples, (5) willingness to donate additional blood samples, (6) patient's mental status at interview, and (7) willingness to provide clinical data for research purposes. Patients who were willing to donate biospecimens were asked one additional question about their main motivations and concerns for donating to the biobank. The additional question was formulated based on the initial literature review. With regard to motivations for donating, participants selected one or more among five closed answer choices: to help other patients, to help doctors to find treatment methods, very interested in learning more, the patients completely trust the doctor and hospital, or other reasons (explain briefly). If patients did not consider donating biospecimens, they were also asked to select one or more in the seven closed answer choices: no self-benefit, physical discomfort, anxiety related to biopsy, inconvenience of time, concerned with disclosure of genetic information that can cause harm to patients' access to insurance, concerned with disclosure of genetic information that could cause harm to patients' access to employment, or other reasons (explained briefly).
Ethics statement
The Ethics Committee of TMUCIH approved the survey protocol. All patients signed written informed consent before the investigation.
Statistical analyses
We conducted descriptive statistics to assess samples' characteristics, including percentages and frequencies. Bivariate analyses, including chi-square and Fisher's exact tests, were used to evaluate the correlation between demographic, department, and other attitudinal factors and donation willingness, that is, willingness to provide future clinical data by comparing proportions and prevalence ratios. Univariate logistic regression was used to examine the association between willingness to participate in biospecimen research and sociodemographic, cancer site, and attitudinal factors. Odds ratios (ORs) and 95% confidence intervals (CIs) were reported. Only variables identified as statistically significant at the 0.05 level in univariate analyses were included in multivariate analyses. Multivariate logistic regression modeling was used to assess cancer site and its association with patients' willingness to donate biosamples. This multivariable statistical analysis yielded the ratios of willingness adjusted for all other confounding variables (age, sex, education, and first hospitalization) included in the regression analysis. All tests were two-sided and p < 0.05 was considered significant. SAS software, version 9.2 (SAS Institute), was used for all statistical analyses.
Results
A total of 811 patients were invited to complete the questionnaire through face-to-face interviews; 784 (96.7%) of them consented to participate and 27 refused to respond. The median age of the interviewees was 55 years (range: 20–85). Patients' characteristics are summarized in Table 1. The study population comprised nearly half males (51.4%) and half females (48.6%). Approximately 94.6% of the participants were Chinese Han and 5.4% were of another race/ethnicity. More than half of the respondents (53.8%) had high school or above education. Moreover, 20.8% had a previous history of hospitalization, 25.9% had cancer family history, 6.4% had benign tumor history, and 18.9% had medical staff among their relatives. Almost half (49.5%) of the study population were living in urban areas and another half (50.5%) were living in the rural areas. Most (92.1%) of the participants were married or living together. A majority (97.1%) of the participants had health insurance. More than one-third (33.2%) of participants had undergone a prior biopsy and only 0.6% had prior clinical trial participation. About 88.0% of the respondents had no mood fluctuations at the time of the survey.
Patients' willingness to donate biospecimens for research purposes
Among the 784 participants, 683 (87.1%) were willing to donate leftover tissues after biopsy or surgery for research purposes. Moreover, 653 (83.3%), 641 (81.8%), and 468 (59.7%) patients were willing to consider donating blood samples, leftover blood after routine testing, and additional blood for research purposes, respectively. Further analysis showed that 631 (80.5%) patients were willing to think of both donating leftover tissue and blood samples. These results indicate that more than 80% of patients could potentially consent to provide paired tissue and blood samples for future cancer research (Table 2).
Donating blood, including donating leftover blood and additional blood.
Factors associated with willingness to donate leftover tissues for research purposes
A chi-square test was performed to demonstrate the relationship between attitudes toward donating surplus biopsy and demographic variables. Attitudes toward donating leftover tissues after diagnosis for cancer research were significantly associated with age, sex, education level, prior biopsy, and first hospitalization (p < 0.05). After adjusting for potential confounding factors, the willingness to donate surplus biopsy after diagnosis was still significantly associated with sex (OR = 0.64; 95% CI: 0.44–0.93, p = 0.02), education level (OR = 2.33; 95% CI: 1.45–3.76, p < 0.001), prior biopsy (OR = 1.57; 95% CI: 1.04–2.37, p = 0.03), and first hospitalization (OR = 0.58; 95% CI: 0.35–0.97, p = 0.04), except age. The participants who were male, with higher education level, prior biopsy, or not first hospitalized were more likely to donate leftover tissues after diagnosis. Attitudes toward donating leftover tissues after surgery for cancer research were significantly associated with sex, education level, residence, and first hospitalization (p < 0.05). Except for sex (OR = 0.62; 95% CI: 0.41–0.94, p = 0.02), education level (OR = 2.05; 95% CI: 1.23–3.39, p = 0.04), and first hospitalization (OR = 0.50; 95% CI: 0.28–0.89, p < 0.001), multivariate analysis indicated no significant association with any other variables (Table 3). The participants who were male, with higher education level, and not experiencing their first hospitalization were more likely to donate leftover tissues after surgery.
ORs were adjusted for age, sex, and education.
p-Values correspond to Fisher's exact test using available data.
Bold results are statistically significant at *p < 0.05; **p < 0.01.
CI, confidence interval; OR, odds ratio.
Factors associated with willingness to donate blood for research purposes
To evaluate whether demographic and other attitudinal variables were associated with willingness to donate leftover blood or additional blood for research proposes, we conducted statistical analyses. The results indicated that willingness to donate residual blood samples differed significantly with sex, education level, and first hospitalization in the study groups (p < 0.05). With the exception of sex (OR = 0.47; 95% CI: 0.32–0.69, p < 0.001) and first hospitalization (OR = 0.53; 95% CI: 0.31–0.89, p = 0.01), multivariate analysis revealed no significant association with any other variables. Respondents who were male or not experiencing their first hospitalization were more willing to donate residual blood. Willingness to donate additional blood was statistically significant with respect to age, sex, education level, benign tumor history, and residence. After adjusting for potential confounding factors, the willingness to donate additional blood samples was significantly associated with age (OR = 0.59; 95% CI: 0.41–0.86, p = 0.01) and sex (OR = 0.48; 95% CI: 0.35–0.64, p < 0.001) (Table 4). Younger male participants were more likely to donate their additional blood samples for research.
ORs were adjusted for age, sex, and education.
p-Values correspond to Fisher's exact test using available data.
Bold results are statistically significant at *p < 0.05; **p < 0.01.
Factors associated with willingness to allow providing clinical data for research purposes
When patients were asked to consider providing clinical data for research purposes, 591 (75.4%) patients agreed. We therefore further explored whether demographic and other attitudinal variables were associated with patients' willingness to provide clinical data for research purposes. We performed Pearson chi-square tests between patient-level variables and the actual donation. Results demonstrated statistically significant bivariate relationships between donation of clinical data and age, sex, and mental status (p < 0.05). After adjusting for potential confounding factors, the willingness to donate clinical data was still significantly associated with age (OR = 0.61; 95% CI: 0.40–0.94, p = 0.02), sex (OR = 0.56; 95% CI: 0.40–0.78, p < 0.001), and mental status (OR = 0.55; 95% CI: 0.34–0.88, p = 0.01) (Table 5). Younger male patients who were not anxious during the interview were more likely to provide clinical data.
ORs were adjusted for age, sex, and education.
p-Values correspond to Fisher's exact test using available data.
Bold results are statistically significant at *p < 0.05; **p < 0.01.
Gender difference of willingness to donate biospecimens from different cancer types
Our data showed that gender is an important factor for donating biospecimens. Female patients were less likely to donate samples compared with male patients. Therefore, we further compared the effect of gender difference in the willingness to donate biospecimens between male and female patients based on different cancer sites. For most cancer types, no statistically significant difference of willingness was found in donating biospecimens between men and women. We only observed several statistical differences between males and females for the willingness to donate biospecimens in maxillofacial otolaryngology and lung cancer and for willingness to provide clinical data for research in liver cancer (Supplementary Tables S1–S4; Supplementary Data are available online at www.liebertpub.com/bio).
Reasons for considering or not considering donating paired samples
Patients were willing to donate paired samples (tissue and blood) because they were very interested in learning more (49.3%) and want to help doctors find treatment methods (48.3%) and help other patients (41.8%). By contrast, the reasons for patients not being willing to donate included concerns about other uses of samples (37.0%), no direct benefit (21.9%), and anxiety related to biopsy (17.8%).
Discussion
Biological samples and associated data are crucial for advancement of cancer research. Understanding the underlying reasons of patients' attitudes toward donating samples for research purposes will improve the consent process and the opportunity to break through the barriers and increase the patients' willingness to donate samples. We conducted a cross-sectional study among cancer patients at a cancer hospital to explore the attitudes of biospecimen and clinical data donation. Results indicated that about 80.5% of patients were willing to donate paired samples. This is a considerable proportion of patients who are potential donors for cancer research with disinterested reasons.
Many factors, such as age, sex, education, race, and other demographic factors, are associated with participation in biospecimen research.4–7 In this study, the results showed that willingness to donate additional blood and clinical data for biobanking was associated with age, which was consistent with findings from other studies. In Ma's study, respondents who were younger, students, company employed, or had a higher education level were more inclined to donate residual biosamples. 8 Frazier's findings showed that older adults acknowledge their lack of understanding of genetic concepts, which resulted in their nonparticipation in genetic research studies. 4 In the present study, 44% refused participation because of pain and discomfort caused by needles. Older patients may experience more medical issues than young participants, thereby feeling too weak to donate additional blood. These results indicate that future research about biobank concepts and older adult participation in biobanking may be needed. In addition, gender was correlated with a willingness to donate all samples and related data. Female participants showed fewer positive attitudes toward biospecimen research than male participants, which affected their willingness to donate blood for biospecimen research.
Stratified analysis based on gender from 11 departments showed that male patients in the maxillofacial otolaryngology and lung departments were more willing to donate samples for research purposes than females. Studies in other populations suggested similar findings. Lee et al. found that Asian American women are significantly less likely to donate compared with Caucasian women in both models, controlling for all other patient-level variables. 9 Similarly, Sanner and Frazier found that being of East Asian descent was a statistically significant predictor of nonparticipation in biospecimen banking compared with other races after controlling for age and gender. The reasons for female cancer patients declining donation are currently uncertain, but may stem from cultural preferences and attitudes toward cancer. The results from this study also showed that patients' willingness to give surplus samples was significantly associated with having a high level of education, which is similar to those studies that involve the general population and patients in China and other countries.10,11
Notably, patients hospitalized for the first time are less likely to donate surplus samples. On the one hand, we presume that first hospitalization or not might reflect the level of trust of medical institutes (hospital). Securing public trust and confidence is a necessary step to ensure long-term viability of biobanks. 12 On the other hand, some other reasons should be taken into consideration, such as those with more hospitalizations are likely to be sicker and may be more altruistic and therefore more willing to donate than others who are healthier. Further study should be performed to find the real connection between patients who are experiencing their first hospitalization and donation. This result will help us develop specific informed consent to encourage patients to donate biosamples upon their first hospitalization. This study also revealed that patients who had prior biopsies were more likely to consider donating a surplus biopsy (p = 0.03). The finding suggests that prior biopsy experiences might have a positive impact on patients. Further research may be required to investigate these patients' experiences.
Another interesting finding from this study was the attitude of donating both sample and related data; 8.3% patients who were willing to donate paired samples would decline to provide clinical data. Most patients who would like to take additional commercial health insurance besides basic insurance were concerned about the disclosure of genetic information that can cause harm to their access to insurance or increase the cost of insurance. Chinese cancer patients are increasingly concerned about privacy and confidentiality of their genetic information and the possibility of adverse consequences of donating their information about their illness to a biobank. There are some related published articles that provide us valuable references. For example, Zhu's study, through a questionnaire survey and in-depth interview, investigated public cognition of genetic testing and attitudes of gene discrimination and found that 76.27% of participants declined to provide genetic information to an insurance company or employer. Preventing and protecting gene privacy and gene discrimination are significant concerns. 13 In Egypt, although not considered a major issue, several participants expressed concern with sharing information with others. 14 A consent form should completely explain the use of biospecimens and ensure the confidentiality of their clinical data.
The present study had a number of limitations. The first limitation of this analysis was the use of willingness to donate blood as a proxy for actual blood donation. We acknowledge that differences may exist among willingness to consider, willingness to consent, and actually undergoing a research biopsy. Lee et al. observed that 66% of women expressed willingness to donate blood or saliva samples at a mammography screening visit, but only 56% actually donated. 9 Another major limitation of this study was selection bias. Participants who joined in this study were selected from only one cancer hospital in a specific geographic region, which may limit the external validity of the results. Moreover, these patients may have more positive attitudes toward biospecimen research and higher willingness to donate blood for the purposes of research than those who elected not to participate in the study. The same factors that contributed to the willingness of individuals to participate in this study could affect their responses to the survey questions, which would lead to more highly and positively correlated consequences. The strength of this study is the high response rate and the integrity of the collected data from face-to-face interviews. We asked about research biopsies outside the context of a therapeutic trial, thus minimizing the potential for therapeutic misconception to some extent. The obtained findings have important implications for research utilizing human tissues.
In summary, this study provides novel empirical data on the likelihood of donating surplus and additional biospecimens and clinical health information in Chinese cancer patients. First, the overall results revealed a relatively high willingness to donate each type of biosample, but low willingness to donate both paired samples and clinical data. This finding suggests that if we would like to obtain the complete sets of samples and data, developing a specific consent is needed. We think specific consent is a suitable objective of future study. If sample collections are for some uncertain future study, we should choose broad informed consent. Meanwhile, if the biobank requested the consent for collection of samples for research in the future and introduced potential for new research methods and techniques to be used, how would researchers protect patients' privacy and guard against potential risks. Moreover, biobanks should make sure to remove any identification of personal information about the samples and dataset. In addition, we should protect the right of patients to opt out of the study at any time.
Second, sensitivity to patient's needs and concerns must be observed. The top three reasons that were cited for not participating in donating biopsies included no direct benefit, risk of other uses of biosamples, and anxiety related to biopsy. These reasons further emphasize the need for patient education and efforts from clinicians to minimize these risks.
Third, this study is the first to investigate cancer patients' attitudes toward donating different types of samples (including surplus biopsy, surplus blood, and additional blood) and clinical data in China. The results identified several factors that could enhance future recruitment efforts to increase participation of Chinese cancer patients in biobanks. Finally, further multicenter research to explore cancer patients' attitudes toward research biopsies may also improve our understanding of barriers that hinder access to human tissues for scientific research.
Footnotes
Acknowledgments
The authors thank Ling Yan and Jifang Wang for their investigation in the survey study and acknowledge the great support from the Department of Nursing in Tianjin Medical University Cancer Institute and Hospital.
Author Disclosure Statement
No conflicting financial interests exist.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.