
Abstract
Background:
The effects of preanalytical variables in tissue processing and storage periods on RNA quality of tissues have been well documented in each type of cancer. However, few studies have been performed on a comparative assessment of the impacts across different cancer tissues, even though it is well known that RNase activity is highly variable in various tissue types and RNase-rich tissues have been found to yield low-quality RNA.
Methods:
We investigated the impacts of cold ischemia times and long-term storage on RNA integrity in various types of cancer tissue, which had been fresh-frozen and collected at the Samsung Medical Center Biobank. RNA quality was also evaluated with regard to histopathological variables. We analyzed RNA integrity number (RIN) data, which had been obtained from our quality control (QC) processes over the last 7 years. Approximately 2% of samples were randomly selected and processed to measure RIN quarterly and after 6 years of storage for QC purposes.
Results:
Fresh-frozen tumor tissues yielded high-quality RNA regardless of tumor type and histopathological features. Up to 1-hour cold ischemia times and up to 6-year storage times did not adversely influence RNA integrity. Only 3 samples showed RIN of <7 out of a total of 396 analyzed tumor tissues.
Conclusions:
Tissue quality was not adversely affected by long-term storage or limited variations of cold ischemia times. The low-quality samples could be correlated with the structural composition or intratumoral heterogeneity of tissues. The strict application of standardized protocols for tissue collection is the key for high-quality biobanking.
Introduction
T
High-quality biospecimens are critical in cancer research utilizing unique or limited resources. Therefore, it is highly recommended that biospecimens are collected and processed following standard operating procedures (SOPs) drafted according to best international practices by, for example, the International Society of Biological and Environmental Repositories or the U.S. National Cancer Institute, and quality control (QC) processes need to be implemented as a routine biobanking procedure.5–7 Biospecimen research should also be conducted to develop and update evidence-based SOPs. The quality of fresh-frozen tissues has been assessed by measuring RNA quality of tissues, and in the recent decade, RNA quality has been determined as RNA integrity number (RIN) values using the Agilent's Bioanalyzer 2100.
Various studies have been conducted to examine the effects of processing temperature, ischemia time, and storage parameters on RNA integrity in a specific type of tumor tissue.8–11 Little research has investigated whether long-term storage and varying preanalytical factors have different effects on RNA quality across various types of tissues, even though it is well known that the RNase activity varies dramatically in a variety of tissues; nonetheless, it has been thought that RNase-rich tissues yield low-quality RNA.
In this study, we aim to analyze the impacts of cold ischemia times, histopathological parameters, and storage periods on RNA integrity across different types of cancer tissues banked with a standardized protocol. More than 2000 fresh-frozen tumor tissues are collected each year at the Samsung Medical Center (SMC) Biobank and about 2% of these samples are randomly tested every 3 months for RNA integrity using our standard QC processes. Cold ischemia time is defined as the period between surgical removal of tissue and snap-freezing. This study was conducted using RIN values that had been obtained from our QC processes at the SMC biobank over the past 7 years.
Materials and Methods
Tissue samples
Various cancer tissue samples and matched normal tissues were collected from patients who signed a consent form for the donation of specimens and underwent surgery for cancer at the SMC from July 2008. Less than 10% of the patients had neoadjuvant chemotherapy and/or radiotherapy before surgery. At the time of resection, tissue samples were collected by attending biobank personnel in an operating room under supervision of a pathologist. If possible, matched normal tissue was also collected in the adjacent tissue at the same time. Tissues were then transported in an icebox maintained at 4°C to the SMC biobank. Upon receipt, the tissues were dissected into ca. 0.2-g (ca. 5 × 5 × 3 mm3) samples and each piece of sample was immediately placed in a labeled cryovial, snap-frozen in liquid nitrogen, and stored in the vapor phase of liquid nitrogen. The time from tissue excision to cryopreservation was kept under 60 minutes and the cold ischemia time was recorded starting in mid-2013.
Histological assessment
All tissue biospecimens were histologically evaluated by preparing hematoxylin and eosin (H&E) slides using a mirror image piece of the fresh-frozen tumor tissues. An experienced pathologist evaluated the tissue for the following parameters: tumor, fibrosis, necrosis, mucin, inflammation, and normal tissue. Approximately 5% of H&E slides were randomly selected annually and the data were validated by two other pathologists, confirming that there were no significant differences between two assessments. Samples with ≥10% tumor cell content were collected at the SMC biobank and included in this study. The tumor cell content is defined as the percentage of tissue area occupied by tumor.
RNA quality
As a part of the QC program of the SMC biobank, ∼2% of recently biobanked tissue samples were randomly selected on a quarter-yearly basis for RNA assessments. RNA was isolated from frozen tissue samples and the RIN was measured. Tissues banked for 6 years were also randomly chosen and the RNA quality of the samples was assessed to investigate the impact of long-term storage on RNA integrity. The RNA quality of 15 tumor tissue samples was verified according to a project's requirements before distribution and the RIN scores from this evaluation were also included. A total of 549 tissue samples (396 tumor samples and 153 matched normal tissues) were analyzed in this study. Each tissue sample was ground to a fine powder under liquid nitrogen using a mortar and pestle. RNA was then isolated using an RNeasy Mini kit (Qiagen) according to the manufacturer's instructions. The quality of RNA was evaluated by measuring RIN on an Agilent 2100 Bioanalyzer.
Statistical analyses
Statistical analyses were conducted using an R package (version 3.0.2). To determine whether RIN measurements were significantly different between tumor samples and their matched normal tissues, paired t-tests were performed, and one-way analysis of variance (ANOVA) tests were used to determine whether there was a difference among different types of cancer tissues. Correlations between cold ischemia times and RIN measurements were evaluated by Pearson's correlation tests. A p-value of <0.05 was considered statistically significant.
Results
RNA integrity in different tumor types
Approximately, 20,000 tumor tissues have been collected since the establishment of SMC biobank and RIN measurements have been performed on about 2% of the collected samples. In this study, RIN values were obtained from 396 tumor tissues. The number of samples and the average RIN value per tumor type are shown in Table 1. Tumor types having more than 10 samples were selected and their RIN values were analyzed by ANOVA (Fig. 1). The results showed that there was no significant difference in RIN values across various types of tumors (p > 0.05).
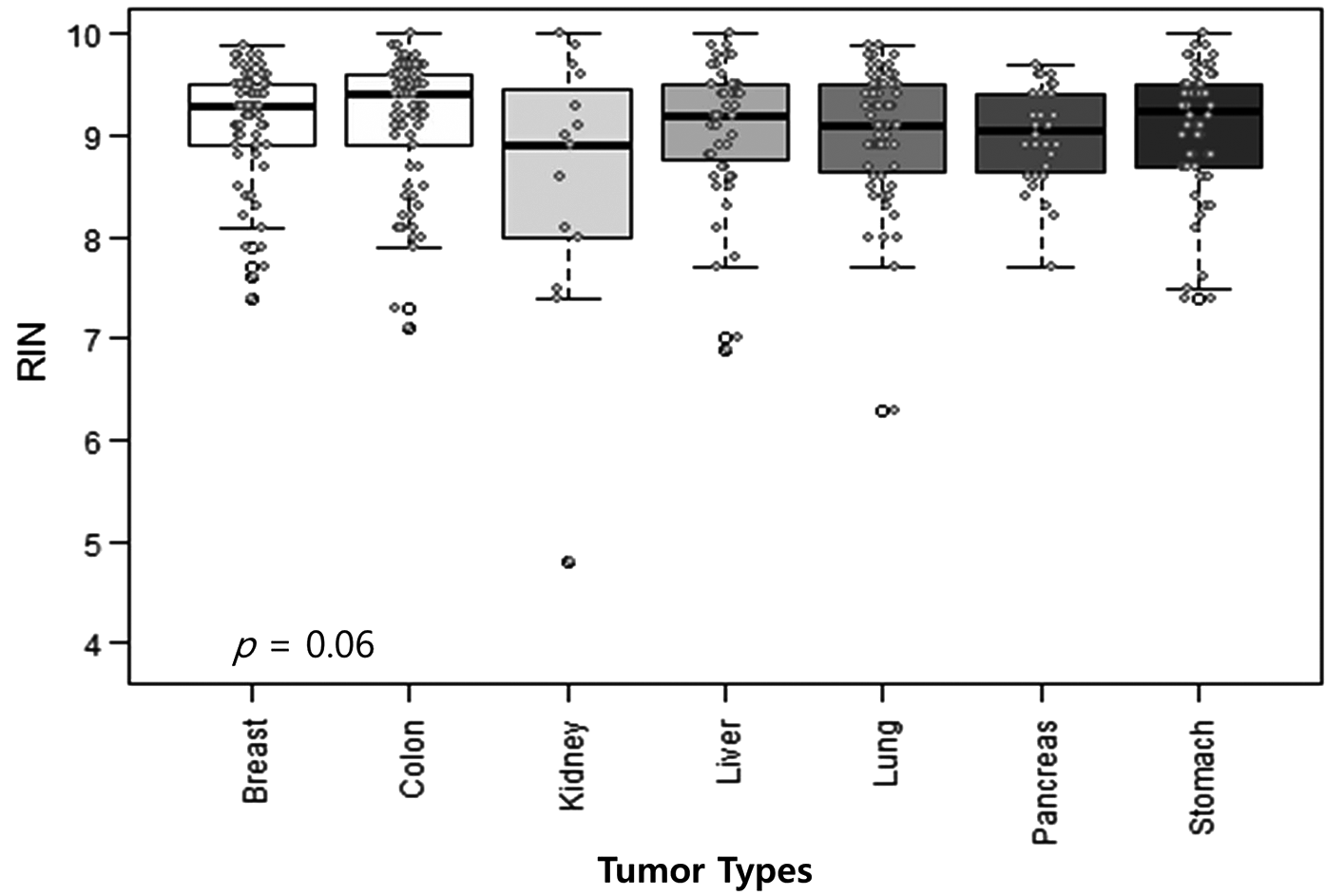
One-way ANOVA was used to compare differences in RIN values across tumor types. Tumor types having ≥10 samples were included in the analysis and a total of 373 samples were used (breast: 69, colon: 73, stomach: 58, kidney: 15, liver: 55, lung: 71, pancreas: 32). The dots denote the RIN scores of samples. ANOVA, analysis of variance; RIN, RNA integrity number.
RIN, RNA integrity number.
Impact of cold ischemia times and storage periods on RNA quality of tissues
For tissue collections, cold ischemia times did not exceed 1 hour, which was in compliance with our SOP; however, accurate records existed only for 126 samples collected in the last 3 years, out of a total of 396 cancer tissues included in this study. The influence of cold ischemia times on RNA quality was evaluated in these 126 cancer tissues and it was found that cold ischemia time periods of <1 hour did not negatively affect RNA quality (p > 0.05, Fig. 2A). The samples were also divided into two groups: cold ischemia times of ≤30 and 31–59 minutes, and the RIN values were compared between the two groups. No statistically significant difference was detected (p > 0.05, Fig. 2B). The total samples analyzed in this study were grouped into three categories according to their storage periods: less than 6, 17–56, and ≥72 months. The relationship between RNA integrity and storage periods was assessed (Fig. 2C). The results indicated that there was no significant impact of storage periods on RNA integrity of tissues (p > 0.05).
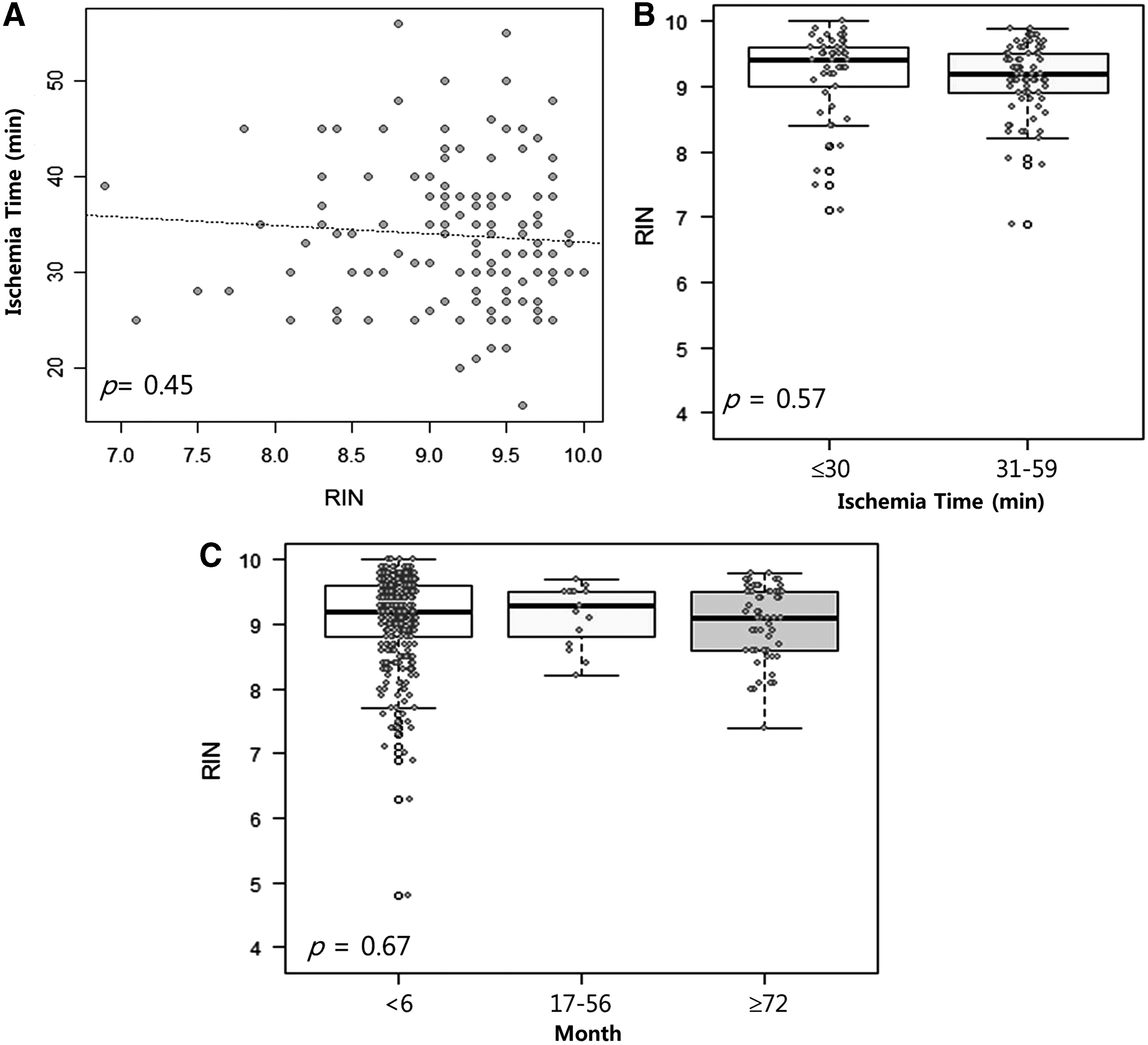
Impact of cold ischemia times and storage periods on RNA integrity of fresh-frozen tumor tissues.
Relationship between histology and RNA integrity
We investigated if there was a relationship between histological characteristics and RNA integrity. Only tumor tissues that were histopathologically evaluated by two pathologists were selected for the analysis and 310 samples were included in this study. Statistical significance was calculated using Pearson's product-moment correlation. The analysis showed that RNA integrity was neither correlated with the percentages of tumor cell nor with tumor necrosis (p > 0.05, Fig. 3A, C). The samples were also divided into two groups according to tumor cell content (≥90% and <90%) or necrosis percentage (≤10% and >10%). RNA quality was not significantly different between the two groups (p > 0.05, Fig. 3B, D).
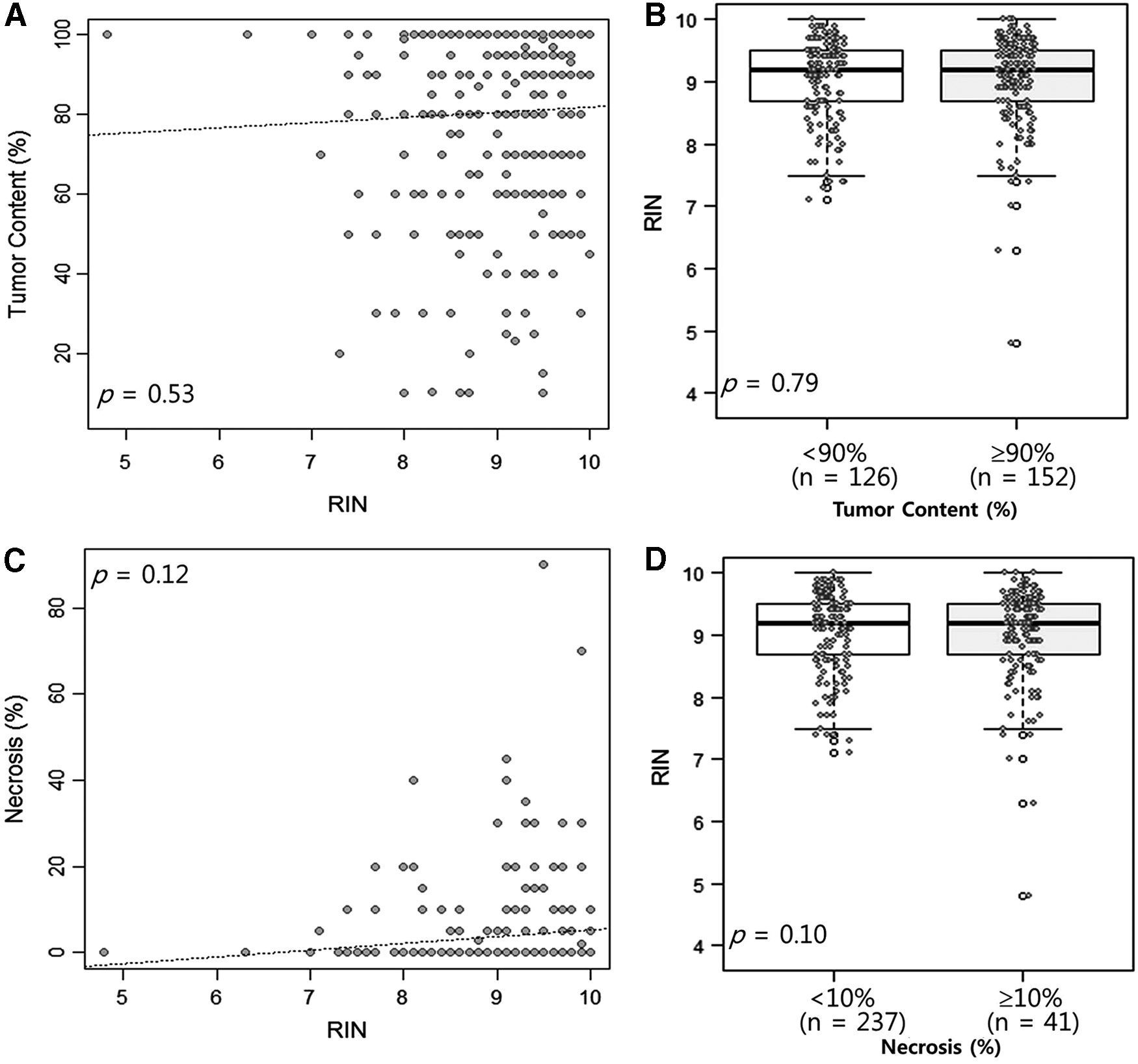
Correlation between histological parameters and RNA integrity in tumor tissues (n = 278).
RNA quality comparison between cancer tissues and matched normal tissues
A total of 127 paired tumor and normal tissue samples were included in this study. RNA quality of the samples was evaluated by measuring RIN and compared between cancer tissues and matched normal tissues. RIN values were statistically higher in cancer tissues when using the total sample set for the analysis (paired t-test, p < 0.001, Fig. 4A). Furthermore, the RIN values were grouped according to tumor types and compared within each group. A significant difference was observed between cancer tissues and matched normal tissues in breast, stomach, and lung cancer (p < 0.05, Fig. 4B–F). There was no significant difference in colon and liver cancer.

Comparison of RIN values between tumor and matched normal samples.
Discussion
Many national and hospital-based biobanks have been established in the cancer genome era and tumor tissues have been recognized as a valuable resource in biomedical, clinical, and translational research. The quality of molecular and genomic analyses of tumor tissues is strongly dependent on the collection, handling, and storage conditions of tissues; therefore, good quality samples have been vital to tissue biobanks. RNA quality measurement has been used as a tool for tissue quality assessment. The RIN analyzed with the Agilent Bioanalyzer is the most widely recognized measure of RNA integrity, as its performance has been shown to be higher than the conventional method measuring the ratio of 28S:18S ribosomal RNA.12–15 RINs vary between 1 and 10, with an RIN 1 denoting completely degraded RNA and an RIN of 10 denoting intact RNA. RNA samples with RIN values of ≥7 are usually considered to be suitable for most downstream applications, including gene expression arrays and transcriptome sequencing.16,17 In this study, we also used a cutoff RIN value of 7 for high-quality RNA.
Studies have been conducted by a number of researchers to investigate the effects of ischemia times and temperatures on RNA integrity of tissues from various tumor types. In most studies, authors found that there were no significant differences in RIN values during cold ischemia times of 1–4 hours in each type of tumor tissue regardless of temperature conditions10,18,19; however, Hong et al. reported that RNA quality of colorectal cancer tissues decreased after 30 minutes of cold ischemia at 4°C. 20 At the SMC biobank, all samples have been collected with cold ischemia times of less than 1 hour since its establishment. In this study, we examined if there were any negative effects of cold ischemia times of <1 hour on RNA integrity across various tissue types. Our results showed that there were no significant correlations between cold ischemia time and RNA integrity within this time frame. However, we have not evaluated cold ischemia times beyond 1 hour and are thus unable to comment on whether longer cold ischemia times would affect the RNA quality of tissues. Similarly, we have not determined whether the RNA integrity would be impacted if the samples were transported from the operating rooms to the biobank at room temperature. When we divided the samples based on cold ischemia time (≤30 and 31–59 minutes) and compared RNA quality of the two groups, there were no significant differences. Furthermore, we assessed RNA quality from various types of tissue samples banked for up to 6 years and found that RNA remained stable. Our results suggest that RNA does not degrade in tissues stored in liquid nitrogen vapor at −175°C for long periods of time. Multiple studies have also reported that long-term storage of tissues at −80°C does not negatively influence RNA quality.8,10,21,22 As mentioned above, cold ischemia times of <1 hour and 6-year storage did not affect adversely the RNA integrity of different tissues stored in our biobank.
As previously reported by other investigators, our results showed that RNA quality was higher in cancer tissues compared to their matched normal adjacent tissues (p < 0.001). 8 In this study, cancer tissues having tumor cell contents of ≥10% were analyzed; therefore, the higher RIN values of cancer tissues might not strongly reflect tumor cellularity levels. In colon cancer, Bao et al. found that the lower RIN values in matched normal tissues might be from the difference in tissue composition because matched normal samples were collected from a mucosa layer, which was rich in connective tissues. 8 Several studies have demonstrated that tissues with high contents of connective or fatty tissue have lower RINs and the structural characteristics may be the reason for low-quality RNA.13,23,24 Lower RIN values are also usually found in mucinous and necrotic tissues. 25 Another reason for this phenomenon could be that tumor cells might have higher resistance to anoxia (and therefore ischemia) than normal cells because the tumor microenvironment is anoxic. However, Mathieson et al. have reported that normal tissues have higher RINs than matched tumor samples in thyroid carcinoma. 22 In addition, we analyzed each tumor type separately as well as the entire sample set and found that the differences in RIN values between cancer and normal samples were statistically significant in breast, stomach, and lung cancer types. These types of organs are known to have high contents of connective or fatty tissue, and normal tissues of these organs may therefore yield low-quality RNA compared to other organs, which are high in epithelial cells.20,26
In our results, only 3 out of a total 396 tumor samples showed RIN values of <7. The three samples having an RIN of <7 are listed in Supplementary Table S1 (Supplementary Data are available online at www.liebertpub.com/bio) and the H&E-stained images of the samples are shown in Figure 5. Supplementary Table S2 shows the tissue samples having RINs <8 and whether the patients had received chemotherapy or radiotherapy before surgery.
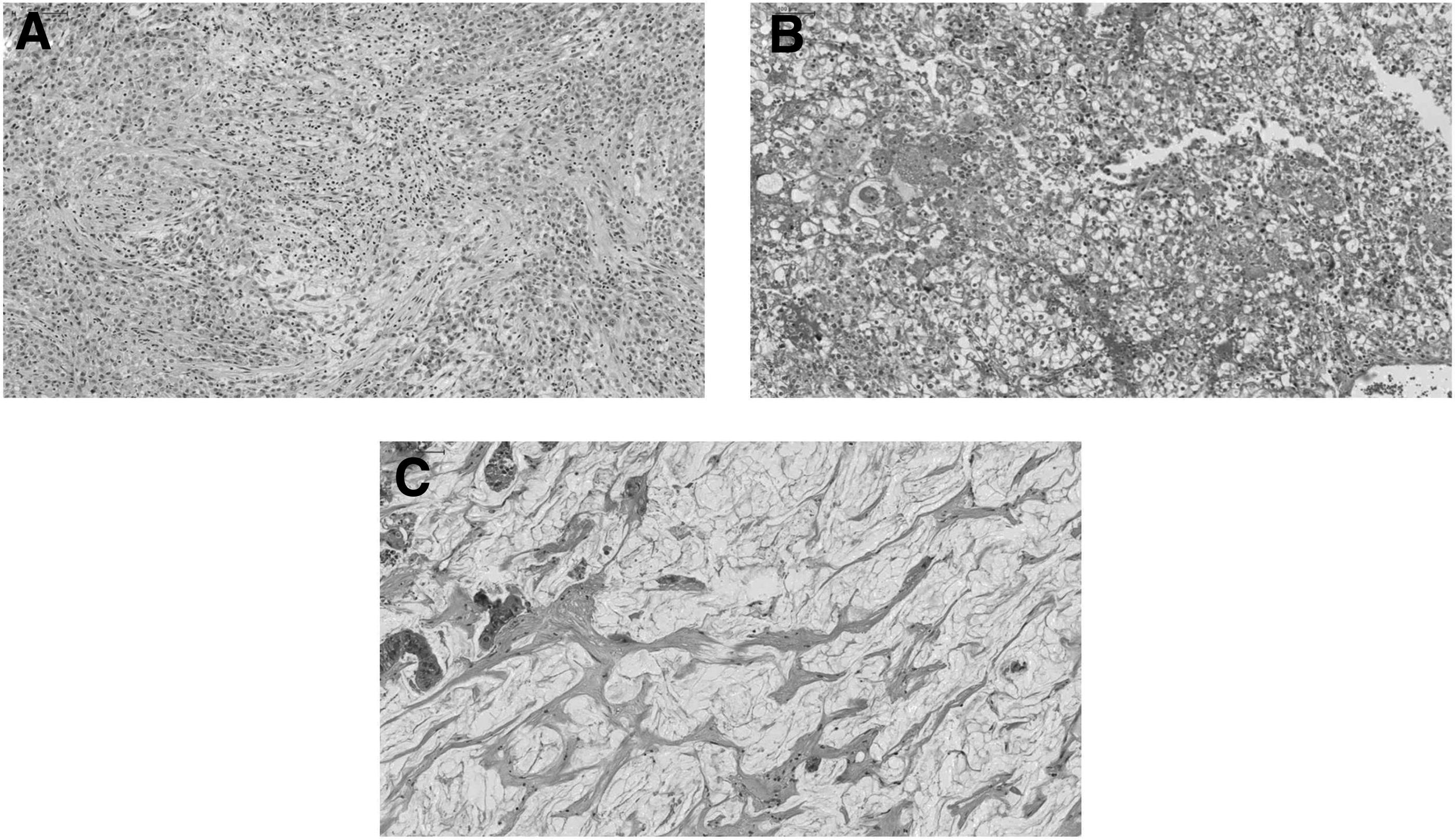
Paraffin-embedded section of mirror image samples of the tumor tissues that yielded low RIN values in our study.
In this study, the samples of low-quality RNA are not unexpected when taking into account well-known tissue types yielding low-quality RNA and can be correlated with tissue composition. One sample exhibiting a lower RIN is mesothelioma, which is a connective tissue tumor and RNA isolated from this tumor tissue may have a relatively low RIN compared to one from tumors of epithelial origin. 25 The other two tumor samples showing lower RIN values are tissues of renal cell carcinoma and colorectal liver metastasis. Grizzle et al. reported that necrosis often occurs in some focal areas of large tumors such as large renal cell carcinoma and liver metastases of colorectal cancer. 27 Zaldumbide et al. also demonstrated that renal cell carcinomas larger than 3.8 cm were morphologically heterogeneous and conventional tumor sampling might not be histologically representative of the entire cancer tissue specimen. 28 The pathological grade for the renal cell carcinoma sample tested in our study was Furhman grade 4 and the tumor size was 9 cm in its largest diameter. Even though microscopic evaluation confirmed that an H&E-stained section from the renal cell carcinoma tissue contained greater than 80% of tumor cells, low-quality RNA might have resulted from intratumoral heterogeneity. 29 Histopathological assessment showed that the colorectal liver metastasis sample contained ∼90% mucin with ∼10% tumor cells, and this high proportion of acellular mucin might be the reason for the lower RIN. Our analysis using histopathological parameters showed that RIN values did not correlate with the proportion of tumor cell or necrosis in all tissue samples, indicating that tumor tissues could be heterogeneous to some degree (Fig. 3). Therefore, morphological assessment would not predict an RIN value in all cases, and detailed diagnosis information as well as histopathology data would be useful to identify tumors having intratumoral necrosis or screen biospecimens that should be checked for their RNA quality. If one aliquot of a tissues is not representative of the entire tumor, a variety of different manual and laser-based dissection tools can be used to isolate only tumor cells from complex tissues for high-quality RNA.30–32 However, low-quality RNA samples can still be a valuable research resource and utilized for technically less demanding assays.
In summary, we evaluated the quality of fresh-frozen tissue samples biobanked within a standardized protocol. The quality of samples was assessed by randomly selecting about two percent of samples and measuring RNA integrity during our routine QC processes conducted on a quarterly basis, as well as incidental quality assessments, over the past 7 years. RNA remained stable regardless of tumor type. RNA integrity was not adversely influenced by cold ischemia times of <1 hour and storage periods of ≤6 years. High-quality RNA was also obtained irrespective of histopathological parameters. Only 3 samples out of 396 tumor tissues showed an RIN of <7 and the lower-quality RNA might have resulted from characteristics of a specific tumor type, rather than preanalytical variables related with tissue collection and processing. However, it should be considered that RNA integrity alone may not be an effective measure of tissue quality. Changes in gene-level expression might not be revealed in this study because detailed molecular analyses of RNA were not conducted. Future research is needed to determine if there are any other molecular markers or tools for better representing tissue quality and to further standardize biobanking protocols.
Footnotes
Acknowledgments
This research was supported by the Basic Science Research Program through the National Research Foundation of Korea funded by the Ministry of Education, Science, and Technology (NRF-2014R1A1A2053938). This research was also supported by the K-Global ICT SW R&D support MOS program funded by the Ministry of Science, Information and Communication Technology and Future Planning in Korea.
Author Disclosure Statement
No conflicting financial interests exist.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.