
Abstract
It is widely accepted that endothelial dysfunction (ED) is a common feature and a risk factor for cardiovascular diseases and metabolic disorders. Cultures of human umbilical vein endothelial cells (HUVECs) are routinely used in cell-based models to study in vitro molecular and cellular mechanisms of development of different aspects of ED. The methods of the HUVEC extraction and expansion are well developed and standardized. However, when large collections of samples are needed for certain projects, or when samples from a rare population of patients should be collected for future experimental use, HUVEC samples should be transferred to a biobank to be saved in liquid nitrogen for a long period of time until the required collection is completed. This scenario is not always convenient since it requires a lot of effort, a large quantity of expensive culture reagents with limited expiration periods, and sometimes special facilities and well-trained cell biologists among the biobank staff. In this project, we evaluated a method of HUVEC cryopreservation, where the stage of cell culturing and expansion before the transfer of samples to the biobank is eliminated. A total of 55 samples of umbilical cord (UC) were obtained from women immediately after delivery. A primary endothelium pellet derived from 17 UC samples was isolated, frozen, and placed in long-term storage in a liquid nitrogen freezer. Other samples were used to obtain HUVEC cultures. We have demonstrated that cryopreservation of primary endothelium pellets from UC veins without culturing and expansion steps does not affect the physiological features of HUVECs. This new approach would improve the efficiency of biobanking logistics, especially in the case of banking of large collections of endothelial samples.
Introduction
E
Therefore, collecting and storing large number of high-quality and well-characterized HUVEC samples for future scientific and practical needs are commercially viable in biobanking practice.
Umbilical cord (UC) vein is the most accessible source of endothelial cells (ECs) because it is easy to collect in any necessary amount, free of any ethical problems, and technically simple to extract ECs by washing the vein with proteolytic enzymes.
The HUVEC immunophenotype is determined as CD45−/CD144+/CD31+/CD146+/CD105+, and the cobblestone-like morphology is specific for HUVEC colonies in long-term cultures.6–10 Their ability to produce an extracellular matrix, 3 cytoskeletal, 11 and other types of proteins, such as von Willebrandt factor (vWF),6,12,13 has been shown in some studies as the key physiological feature of HUVECs.
The standard and widely accepted methods of HUVEC extraction and expansion are well developed and include enzymatic dissociation of the umbilical vein using collagenase type III, followed by culturing of the isolated primary HUVECs in endothelial basal medium (EBM)14,15 up to passage 2 before experiments, for control of HUVECs' morphology. Therefore, these methods take a long time and must be performed by highly qualified staff.
In the situation when a large collection of samples is needed for certain projects, or when a set of samples from a rare population of patients should be collected for experimental treatment, HUVEC samples should be transferred to a biobank to be saved in liquid nitrogen for a long period of time until a required collection is completed. For long-term storage of cell samples at ultra-low temperature, chemical cryoprotectants, such as dimethyl sulfoxide (DMSO), are routinely used. 16
This protocol is not always convenient in biobanking of large number of samples since it requires a lot of effort, a large quantity of expensive culture reagents with limited expiration periods, and sometimes special facilities and well-trained cell biologists among the biobank staff to perform the cell culturing process. The HUVEC isolation and cell freezing procedures are well standardized,15,17 do not require a high level of biotechnological competence, and can be completed in one working day by the general laboratory assistant staff.
In this project, we evaluated a method of HUVEC cryopreservation, wherein the stage of cell culturing and expansion before transfer of a sample to biobank is eliminated, to increase productivity of routine HUVEC biobanking practice.
Methods
UC collection and ethical aspects
UC samples were collected from women after physiological delivery, or after cesarean section in the Specialized Perinatal Centre of Federal Almazov North-West Medical Research Centre in Saint-Petersburg, Russian Federation. All biological samples were collected according to the Declaration of Helsinki and with permission of the local ethical committee No. 119, dated July 13, 2015. An informed consent was signed by every donor.
Fifty-five samples of UC were obtained from women immediately after delivery. Up to 20 cm of UC was cut off and packed into a sterile bag, and then transferred to the biobank laboratory. Storage of the sample at +4°C for up to 24 hours before processing was allowed.
Design of the experiment
In this study, we proposed to eliminate the stage of primary HUVEC culturing and proceed to freezing of endothelial pellet immediately after its isolation from the umbilical vein. The other samples were routinely precultivated before cryopreservation and used for comparison of HUVEC culture quality, obtained using both methods (Fig. 1).
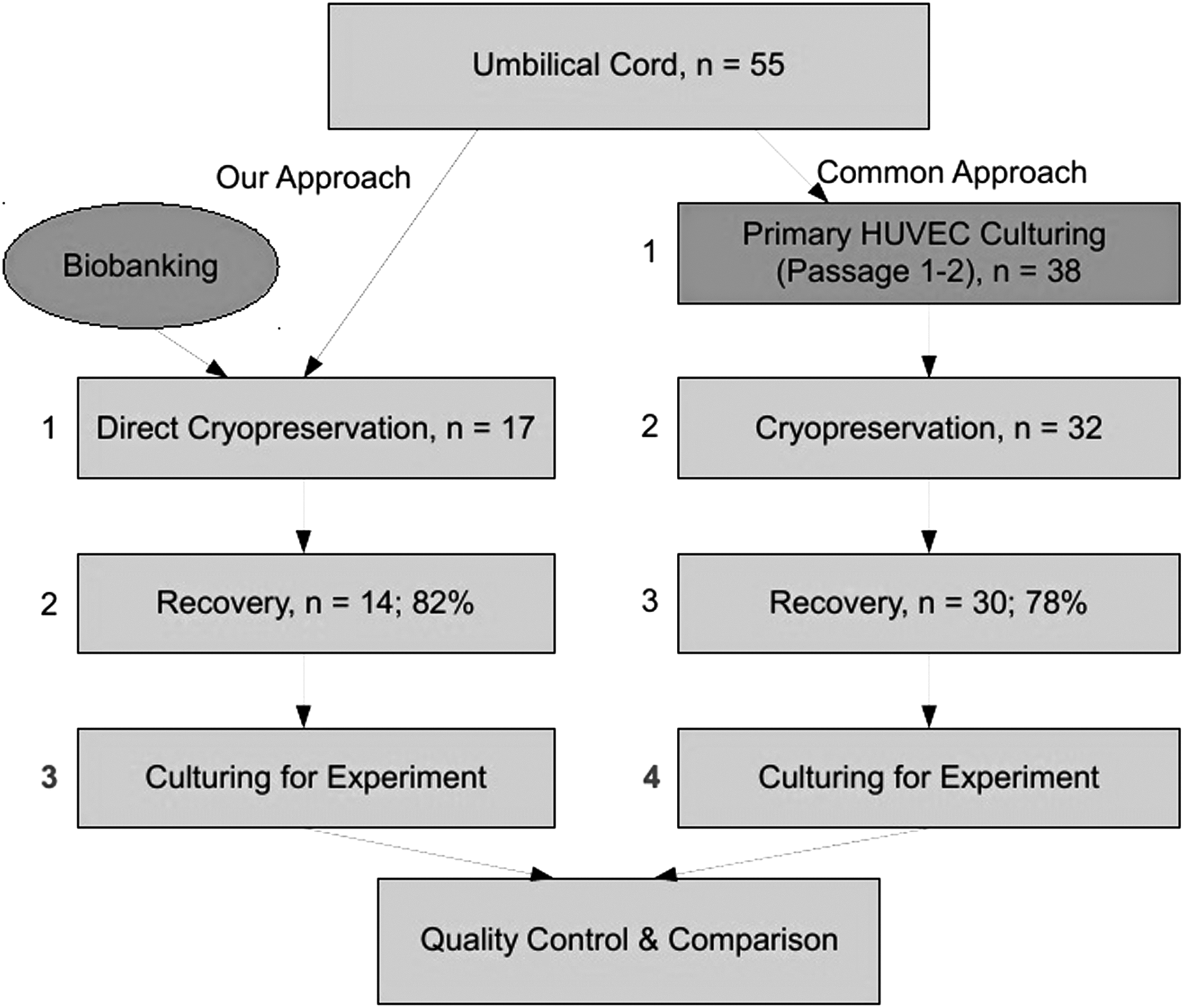
Schematic design of the experiment. HUVECs, human umbilical vein endothelial cells.
Primary endothelium extraction from umbilical vein
To isolate endothelium from UC, the umbilical vein was filled with the enzyme collagenase (type III) and incubated at +37°C followed by repeated cycles of washing with phosphate buffered saline (PBS). The primary endothelium pellet derived from 17 UC samples was isolated, frozen, and placed in long-term storage in a liquid nitrogen freezer. Other samples were used to obtain HUVEC cultures.
HUVEC culturing
A total of 38 HUVEC cultures were obtained by seeding the primary endothelium pellet onto culturing flasks in EBM. Before use, the flasks were treated with 0.2% gelatin for 5 minutes. The primary HUVEC cultures were incubated for 48 hours under standard culture conditions: +37°C and 5% CO2. After preincubation (passage 0), nonadherent cells were washed with PBS and adherent cells were cultured until reaching 80%–90% of confluence. The cells were removed from the flasks with 0.05% trypsin, washed with PBS, and seeded onto new culturing flasks in EBM (passage 1). HUVEC cultures were processed up to passage 2, and then were frozen and stored in liquid nitrogen.
Cryopreservation of primary endothelium pellet and HUVEC cultures
For cryopreservation of primary endothelium and cultured HUVECs, the same protocol was used: the pellet was resuspended in 1 mL of fetal bovine serum containing 10% of DMSO, then the tubes were placed into a container with standardized controlled rate −1°C/minute cell freezing in a −80°C freezer, followed by transfer into liquid nitrogen. The samples were stored at ultra-low (−196°C) temperature up to 12 weeks.
Primary endothelium pellet and HUVEC cultures recovery
The samples were recovered by fast thawing at +37°C, followed by immediate replacement of the cells into EBM and seeding the suspensions onto culturing flasks. The cultures were incubated under standard culture conditions for 24 hours, then nonadherent dead cells were washed from the cultures with PBS. The samples were considered successfully recovered if they produced cobblestone-like HUVEC colonies within 24 hours after seeding. The number of viable cells in samples before freezing and after recovery was overlooked since it was impossible to count the cells in endothelial tissue fragments, mixed with blood cells, after enzymatic treatment.
Flow cytometry analysis
The immunophenotype of HUVEC cultures was determined by flow cytometry, detecting the expression of HUVEC-specific cell surface markers. Cells were analyzed for human CD45, CD144, CD31, CD146, and CD105 on a flow cytometer Guava EasyCyte™ 8, followed by data analysis in Guava EasySoft V2.0. As a negative control, nontreated HUVECs in PBS were used.
Immunocytochemical assay
The expression of vWF was analyzed by immunocytochemical assay. HUVEC cultures, seeded onto cover glasses, were fixed with 4% paraformaldehyde. Fixed samples were treated with mouse antibody against human vWF and stained with fluorescent dye Alexa-546 conjugated with antimouse antibody. Simultaneously, the samples were treated with rabbit antibody against human CD146 and stained with fluorescent dye Alexa-488 conjugated with antirabbit antibody. The vWF and CD146 expression were analyzed by fluorescent microscopy.
Results
Preparation of HUVEC primary cultures
A total of 38 samples of umbilical vein were used for immediate HUVEC isolation and culturing. HUVEC cultures were successfully obtained from 32 UC samples. After passage 2, cell cultures were frozen in liquid nitrogen for up to 12 weeks.
Viability and morphology of HUVECs after recovery
Recovered primary endothelial pellets
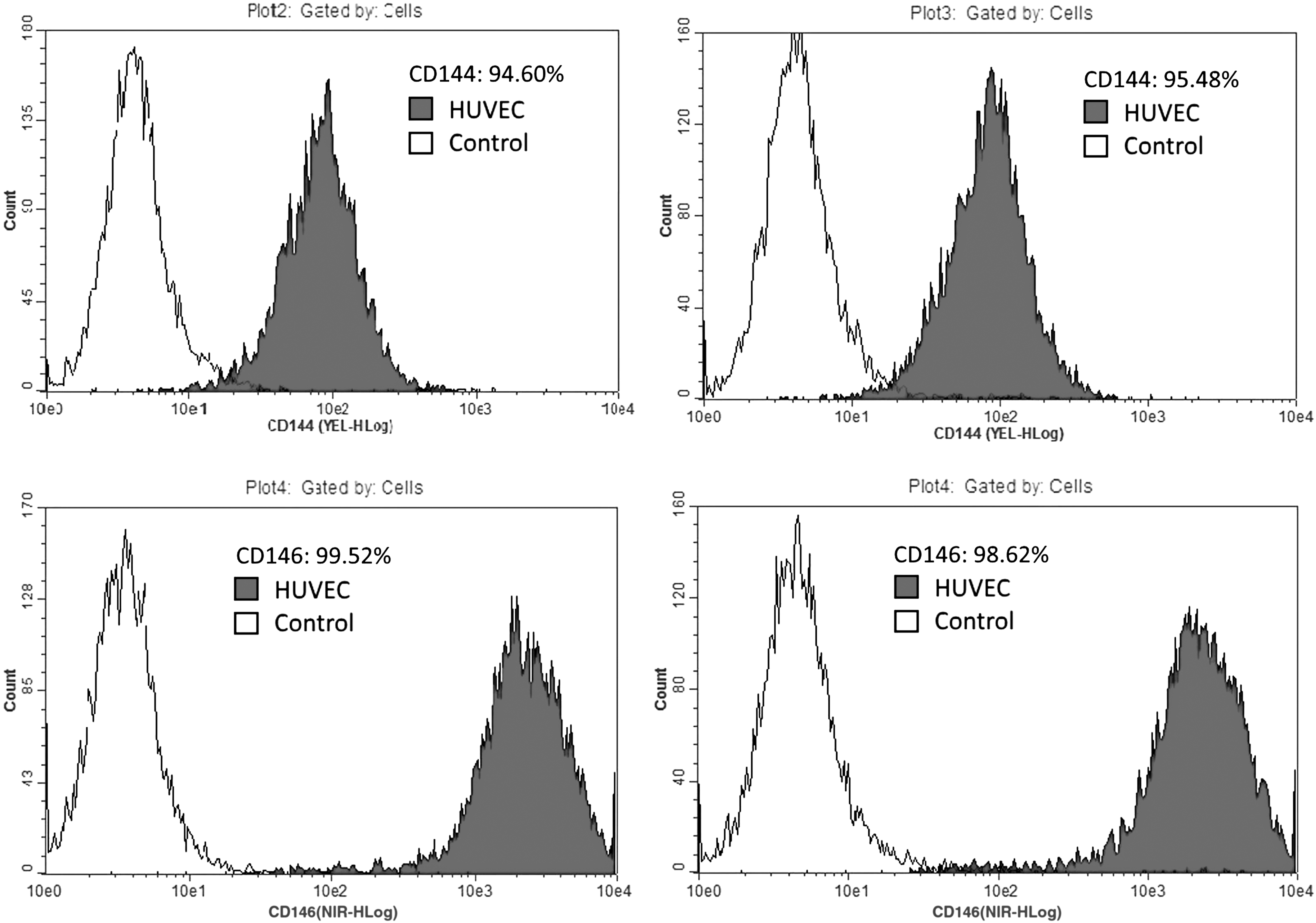
After thawing 17 primary endothelial pellets, 14 viable HUVEC cultures were successfully obtained, constituting 82%. In all cultures, we observed HUVEC-specific cobblestone-like morphology (Fig. 2) of cell colonies, immunophenotype CD45−/CD144+/CD31+/CD146+/CD105+ (Fig. 3), which strictly conforms to HUVECs' immunophenotype.
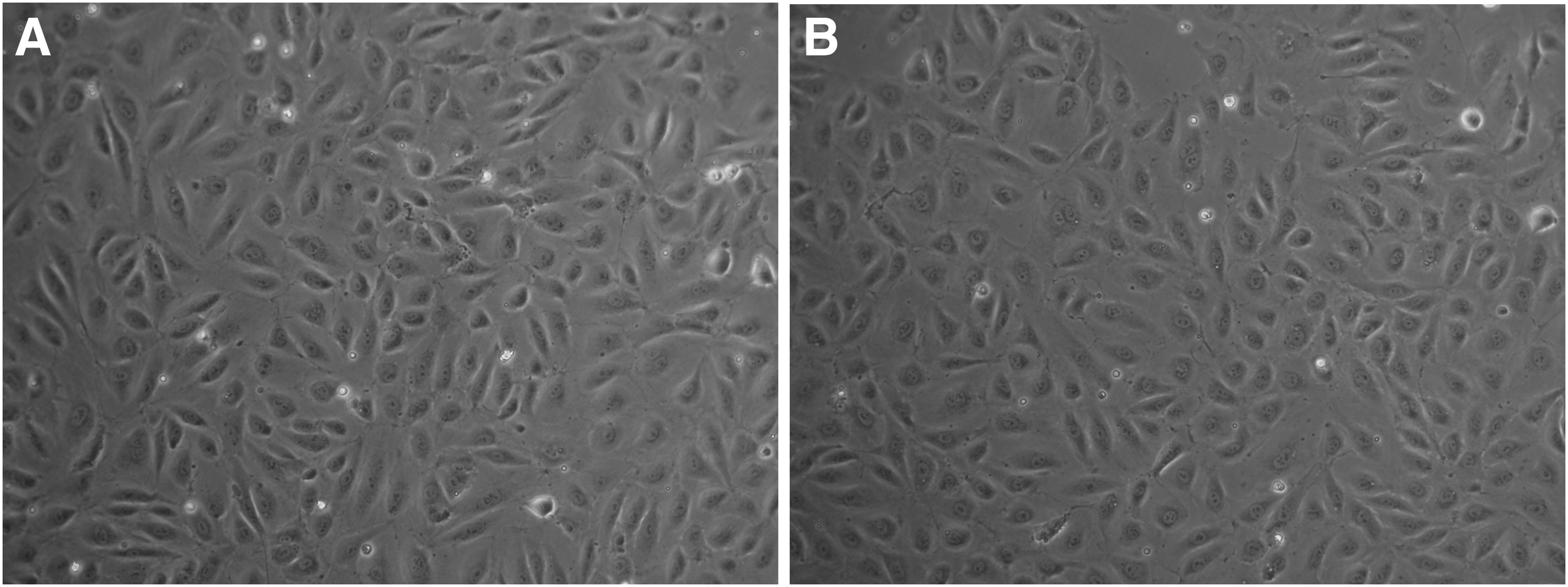
Phase contrast microphotographs of the HUVEC cultures.

Immunophenotype of the HUVEC cultures derived from recovered primary cryopreserved endothelium pellet (left panel) and from primary precultivated and cryopreserved HUVEC cultures (right panel). The percentage of positive cells for the relevant CD marker is shown.
In all examined cultures, we also detected positive expression of both vWF in cell cytoplasma and CD146 on cell membranes (Fig. 4).
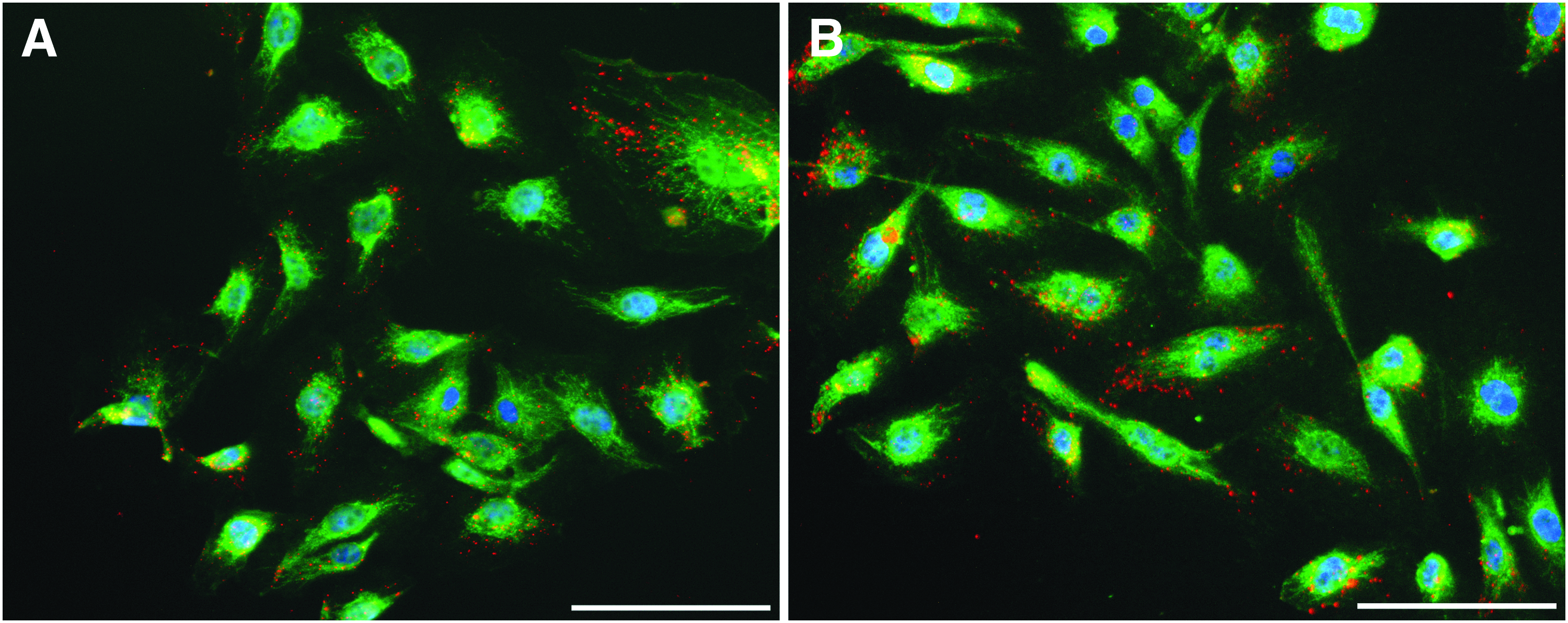
Immunocytochemical staining of the HUVEC cultures.
Recovered HUVEC cultures
From 32 frozen HUVEC samples, 30 HUVEC cultures were successfully recovered, which constitutes 78% (considering the loss of samples on the stage of primary cultivation, Fig. 1). In all cultures, as well as in primary frozen endothelial pellets-derived HUVEC cultures, we observed HUVEC-specific cobblestone-like morphology (Fig. 2) of cell colonies and HUVEC-specific immunophenotype CD45−/CD144+/CD31+/CD146+/CD105+ (Fig. 3). All samples in this group were also vWF and CD146 positive in the immunocytochemical assay (Fig. 4).
Discussion
In this study, we evaluated an alternative approach to HUVEC cryopreservation, wherein the stage of primary cultivation is eliminated before freezing and storage. In several studies, it was shown that HUVEC samples can be cryopreserved in different stages of their expansion8,18 without loss of any physiological features. In contrast, in some studies the loss of endothelial tissue in a case of a whole vessel cryopreservation, without primary endothelial pellet isolation, was shown. 19
We compared different approaches of HUVEC cryopreservation and recovery, using standard methods of HUVEC isolation and cultivation,14,15 and cell cryopreservation, which is described as the most effective for many kinds of cells including HUVECs.16,17 Using these methods, we did not detect a difference in culture recovery rate after cryopreservation using both protocols (Fig. 1). The loss of some samples at the stage of primary cultivation we associated with low quality of some UC samples (very short fragment of cord, high quantity of thrombosis in a vein, presence of postinjectional vein perforations, etc.), and we recommend rejecting such kinds of UC from further processing.
In our study, we have demonstrated that cryopreservation of endothelium from UC before culturing and expansion steps allows obtaining viable HUVEC cultures of good quality.
This new approach would help to improve the efficiency of biobanking logistics especially in case of banking of large collections of endothelial samples. Furthermore, this approach could be tested with ECs from different sources.
Footnotes
Acknowledgments
We thank biobank technician Marina Vishnevskaya, for performing routine cryopreservation procedures, and endocrinologists of the Specialized Perinatal Centre, Dr. Alexandra Tkachuk and Dr. Yana Bolot'ko, for selection of donors and organization of UC samples collection.
The study was funded by Russian Science Foundation (project No. 15-14-30012).
Author Disclosure Statement
No conflicting financial interests exist.