
Abstract
Background:
Cold ischemia protects organs and tissues by slowing their metabolism, but it also causes ischemic injury. Minimizing cold ischemia has been an important goal in parathyroid auto- and allotransplantation, as well as the transplantation of other major organs. Parathyroid glands are responsible for calcium homeostasis by releasing parathormone (PTH) into the blood circulation. Functionality of a new parathyroid transport solution (NPTS) and effects on cell viability, PTH secretion, and calcium-sensing receptor (CaSR) levels during cold ischemia were evaluated.
Materials and Methods:
A NPTS was prepared, and the pH was adjusted to a range of 7.2–7.4 and kept at +4°C until use. Seven patients with parathyroid hyperplasia secondary to chronic renal failure who were scheduled to undergo subtotal parathyroidectomy were enrolled in the study. Glands were cold-preserved in NPTS with different time intervals (0, 6, 12, 18, and 24 hours), and then parathyroid cell viability before and after cryopreservation, PTH secretion, and CaSR levels were determined.
Results:
The mean cell viability before cryopreservation was 92.7% (range 89.2%–97.2%). There were no significant differences in cell viability rates before and after cryopreservation (p = 0.1168 and p = 0.4085, respectively), and CaSR levels (p = 0.5446) were not significant.
Conclusions:
NPTS is a solution designed specifically for parathyroid tissue transplantation. This patent pending product can support cellular viability and PTH release, as well as protect CaSR functionality for up to 24 hours of cold ischemia.
Introduction
O
Cold ischemia protects organs and tissues by slowing their metabolism. However, it has harmful effects on the tissues due to oxidative stress and inflammation. These effects are physiopathologically defined as ischemia–reperfusion injury in organ transplantation.3,4 ATP levels are maintained constantly in metabolically active cells. During cold storage of tissues, several metabolic pathways led to a breakdown of membrane-associated ion homeostasis, thus causing cell death by either apoptosis or necrosis.3,5,6 The most widespread methods to preserve organs for transplant usually involve cooling in specific solutions. The process introduces numerous variables affecting the state of the organ, such as molecular changes, cellular injury, and edema.5,7
Recently numerous biopreservative solutions such as the University of Wisconsin (UW) solution, Histidine-tryptophan-ketoglutarate (HTK), Celsior, Euro-Collins, and Perfadex have been commonly used during perfused or static storage of organs.3,5 The UW solution is the gold standard solution; it substantially improves graft preservation and consequently increases graft survival.4,8
Parathyroid glands are responsible for calcium homeostasis by releasing parathormone (PTH) into the blood circulation. Minimizing cold ischemia has been an important goal in parathyroid auto- and allotransplantation, as well as the transplantation of other major organs. Parathyroid allotransplantation appears to be a promising option for the treatment of permanent hypoparathyroidism.9–11
Parathyroid transportation with UW has a high cost and is single use, and the nonreusable option of the UW solution led us to design new parathyroid transport solution (NPTS). The parathyroid gland is relatively simple unlike other organs such as kidney and liver, and is easy to work with in vitro for transplantation. During transportation of parathyroid glands, 5 mL of preservation solution is sufficient.
The parathyroid glands consist of three different cell types, water clear, oxyphil, and chief cells. The calcium-sensing receptor (CaSR) is expressed abundantly in the chief cells.12,13 CaSR is expressed at lower levels in other tissues and is likely to play roles unrelated to mineral ion homeostasis. Receptors also play a crucial role in regulating PTH secretion, 13 which means control over calcium-dependent systemic ion homeostasis. In contrast, the pathways connecting CaSR to parathyroid proliferation are not known yet, and patients with primary or secondary hyperparathyroidism exhibit reduced CaSR expression.14,15
The aim of this study was to evaluate functionality of a NPTS (patent pending) and assess its effect on cell viability, PTH secretion, and CaSR levels during cold storage of parathyroid glands.
Materials and Methods
This study was conducted after receiving approval from the Local Human Ethics Committee (Approval No. 30112016-19444) and also registered by the clinical trials registry (NCT02978287). All of the protocols conformed to the ethical guidelines of the Helsinki Declaration, and written informed consent was obtained from all subjects.
Preparation of NPTS
NPTS consists of five main components that are essential for the parathyroid gland, namely, amino acids (both essential and nonessential), inorganic salts, vitamins, fetal bovine serum (FBS), selenium, and 4-(2-hydroxyethyl)-1-piperazineethanesulfonic acid (HEPES). HEPES is included as a pH indicator. The pH was adjusted to a range of 7.2–7.4. All components were combined under sterile conditions and kept at +4°C until use. The contents of the solution are described in Table 1.
Values are shown as mmol unless otherwise indicated.
HEPES, 4-(2-hydroxyethyl)-1-piperazineethanesulfonic acid; NPTS, new parathyroid transport solution.
Donor recruitment
Seven patients (three male, four female, mean age 37 years, range 31–54 years) with parathyroid hyperplasia due to chronic renal failure, who were referred from the nephrology outpatient clinic to the general surgery department for surgical approach, were enrolled to the study. Patients had been scheduled for subtotal parathyroidectomy. Patients who had their parathyroid tissue damaged during surgery or who had hepatitis B, hepatitis C, or human immunodeficiency virus were excluded from the study. Primarily, tissues were evaluated morphologically; then half of each of the resected glands was delivered to the pathology department for diagnosis. The remaining parts of the glands stored in ice-cold NPTS were transported to the parathyroid cell culture laboratory unit.
Preservation solution treatments and isolation of parathyroid cells
The tissue samples were removed from cold storage after 0, 6, 12, 18, and 24 hours. First, cell isolation of tissues was started after the frozen tissue examination approval. Approximately 25–30 minutes of cold ischemia in NPTS was accepted as zero time point. At each time interval around 100 mg tissue was cut and washed with 1 × phosphate-buffered solution (Thermo Fisher Scientific, MA) (pH 7.4) and minced in a Petri dish on ice. The minced preparation was combined with 2 mL for a total 100 μg/mL bovine serum albumin (Merck Millipore, Germany), 215 μmol collagenase type II (Thermo Fisher Scientific), 0.32 μM DNase I (AppliChem, Gatersleben, Germany), and 1 mL Ham's F-10 Supplement (Thermo Fisher Scientific). Samples were transferred to an incubator (CCL-170B-8; ESCO, Singapore) at 37°C with humidified atmosphere containing 5% CO2, where they were incubated overnight. Each sample was filtered into a 15-mL conical Falcon tube using a sterile cell strainer (70 μm, Falcon; BD Biosciences, NJ). The solution was centrifuged at 306 g for 15 minutes to obtain a pellet. Cells were suspended in 1 mL of culture medium. Parathyroid cell viability was assessed before cryopreservation using a Muse Cell Analyzer (Merck Millipore) with a Muse Count & Viability Assay Kit (Merck Millipore). The cells were mixed with 10% DMSO (dimethyl sulfoxide), 10% FBS, and suspended in cryotubes, kept at −80°C, and then transferred to a liquid nitrogen tank for storage.
Cultivation
The cells in the nitrogen tank were removed after 30 days of cryopreservation and cultivated in flasks with McCoy's 5A (Modified) Medium (Thermo Fisher Scientific) with 1% sodium pyruvate, 1% penicillin–streptomycin, and 10% FBS and placed in an incubator (CCL-170B-8; ESCO) at 37°C with 5% CO2 humidified atmosphere, where they were kept overnight. After cultivation for 24 hours, cell viability was assessed after cryopreservation, and supernatant samples were removed and stored for PTH measurement. The cell pellet was prepared for total protein extraction.
PTH enzyme immunoassay
PTH levels of cell culture supernatant samples were determined with commercially available Human Enzyme Immunoassay Kit (RayBiotech, Inc., Norcross, GA). Absorbance was determined at 450 nm using an iMark Microplate Absorbance Reader (Bio-Rad).
Preparation of total protein extracts
Protein extraction was performed using RIPA Lysis Buffer (Santa Cruz Texas). Before lysing cells, a solution was made with 10 μL PMSF (phenylmethylsulfonyl fluoride) solution, 10 μL sodium orthovanadate solution, and 15 μL protease inhibitor cocktail solution per milliliter of 1 × RIPA. One milliliter of complete RIPA was used per 2.0 × 107 cells in suspension. The suspension was frozen overnight at −80°C. The extract was centrifuged for 15 minutes at 18721 g, and then the supernatant was collected. The total protein concentrations were measured using a Coomassie (Bradford) Protein Assay Kit (Thermo Fisher Scientific).
Western blot
A 30 μg sample of total protein extract was separated on 4%–8% gradient sodium dodecyl sulfate (SDS)–polyacrylamide gels and transferred to PVDF (polyvinylidene fluoride) membranes (Bio-Rad) in 1 × transfer buffer at 100 V for 1 hour 20 minutes with the Trans-Blot Turbo Transfer System (Bio-Rad). The membranes were blocked overnight at +4°C with TBST (Tris Buffered Saline with Tween) containing 5% nonfat milk. The primary antibody was mouse monoclonal anti-calcium sensing receptor antibody (3 μg/mL; Thermo Fisher Scientific), and the secondary antibody was anti-mouse IgG and horseradish peroxidase-linked antibody (1:3000 dilution; Cell Signaling). The membranes were washed five times (5 × 5 minute), each between antibody incubations with TBST. The blots were developed using the Electrochemiluminescence Detection Kit (Bio-Rad).
Statistics
One-way ANOVA (GraphPad Software, Inc.) was used for analysis of quantitation of the western blot and viability results.
Results
Viability assay
The viability profile of each tissue depending on their cell population profile was determined (Fig. 1). The mean cell viability of five time intervals before cryopreservation was 92.7% (mean range 89.2%–97.2%) (Fig. 2A) and after cryopreservation was 95.44% (mean range 93.2%–96.6%) (Fig. 2B). No significant differences between cold ischemia times (0, 6, 12, 18, and 24 hours) before and after cryopreservation (n = 7) (p = 0.1168, p = 0.4085, respectively) were determined (Fig. 2). In addition, the post-thaw cell quantity of cryopreserved parathyroid cells decreased at 13.8%.
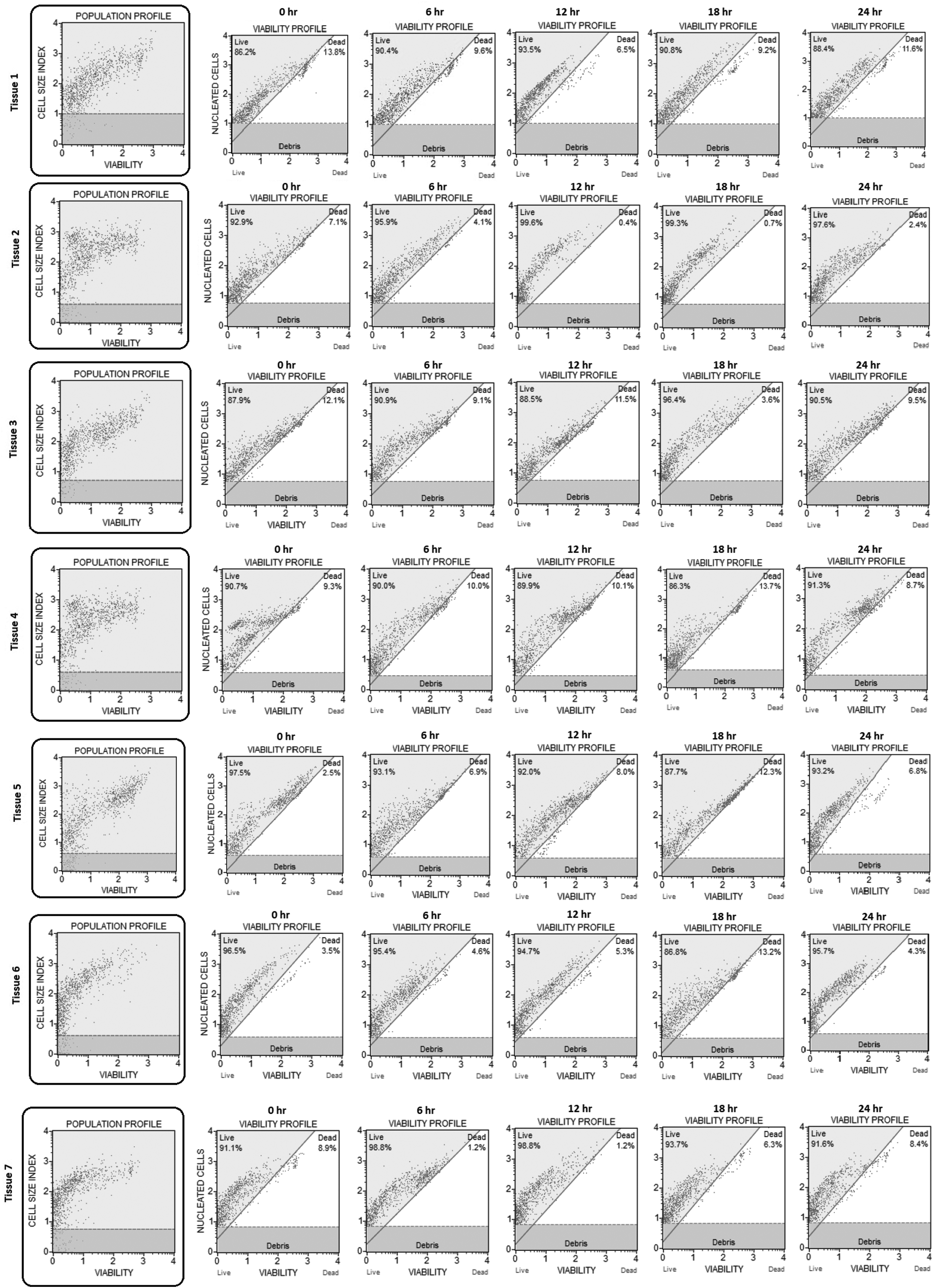
The cell viability profile of nucleated cells obtained from seven different parathyroid hyperplasia tissues. Each isolated parathyroid cell viability profile adjusted according to the cell size index ratio.
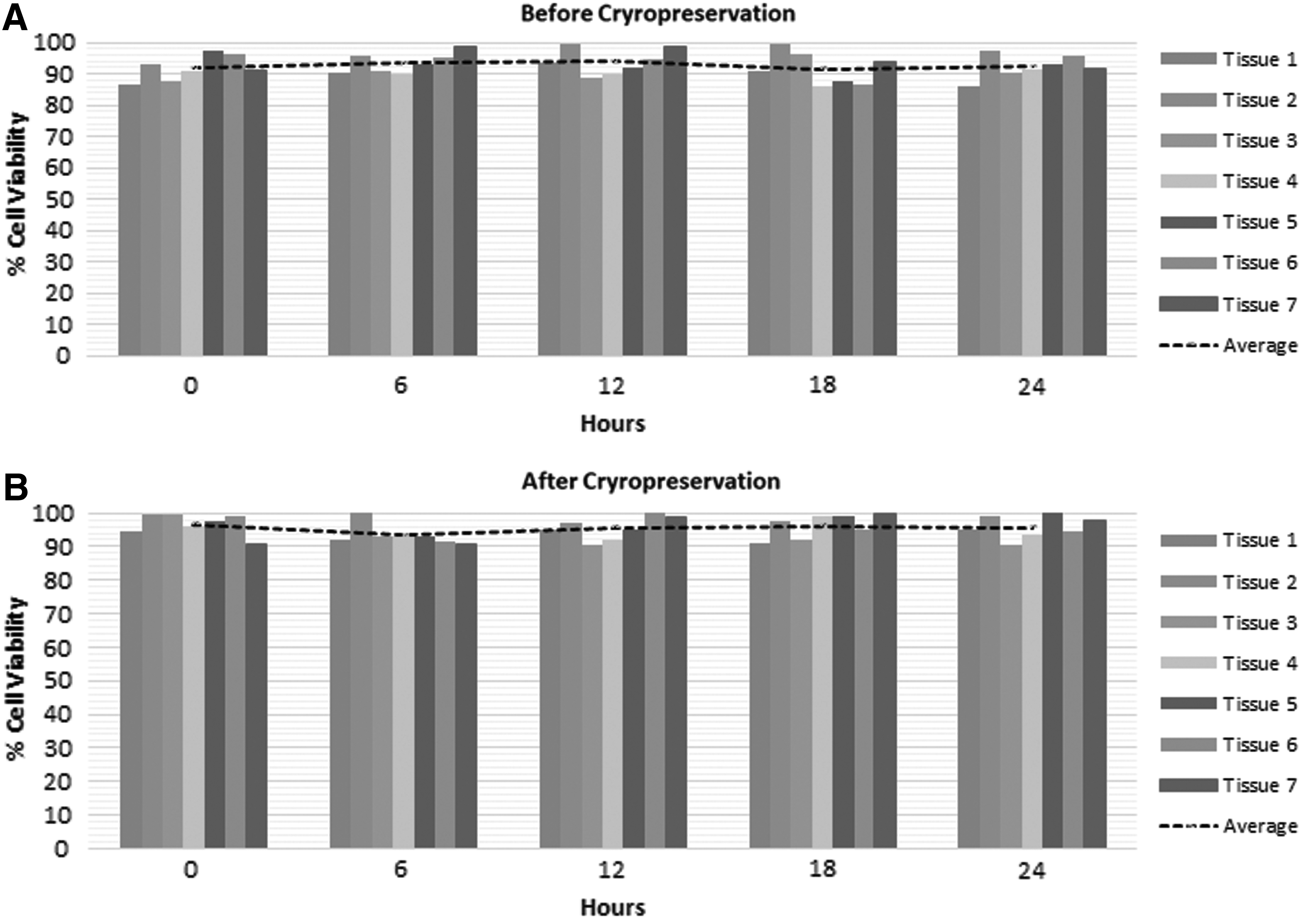
Cell viability assay of parathyroid gland cells following the treatment with NPTS during different cold ischemia times (0, 6, 12, 18, and 24 hours).
PTH release and CaSR expression
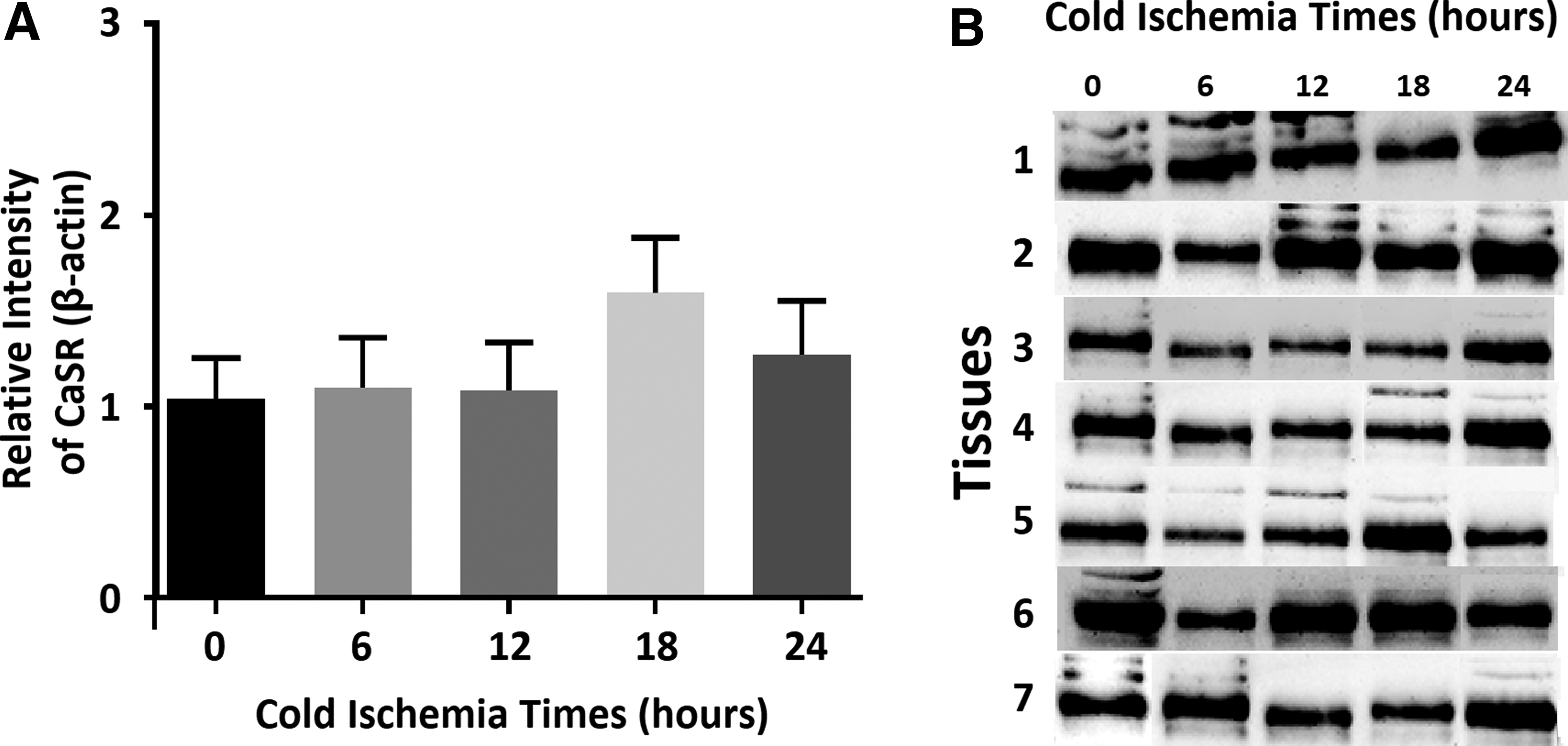
PTH levels were significantly increased during cold ischemia (p = 0.0476) (Fig. 3) (See Supplementary Table S1; Supplementary Data are available online at http://www.liebertpub.com/bio). Western blot: Protein lysates from isolated cells were separated by SDS-PAGE (polyacrylamide gel electrophoresis) and immune detection completed using CaSR (120 kDa) and β-actin (45 kDa) antibodies. CaSR protein levels were normalized to the β-actin density of each sample as a loading control (See Supplementary Fig. S1 for further details). The relative optical densities of the protein bands were measured following subtraction of the background signal. Data are reported (Fig. 4A) as the mean ± standard error of the mean. During cold ischemia, there were no significant differences between different time intervals (0, 6, 12, 18, and 24 hours) of CaSR levels (p = 0.5446, Fig. 4).
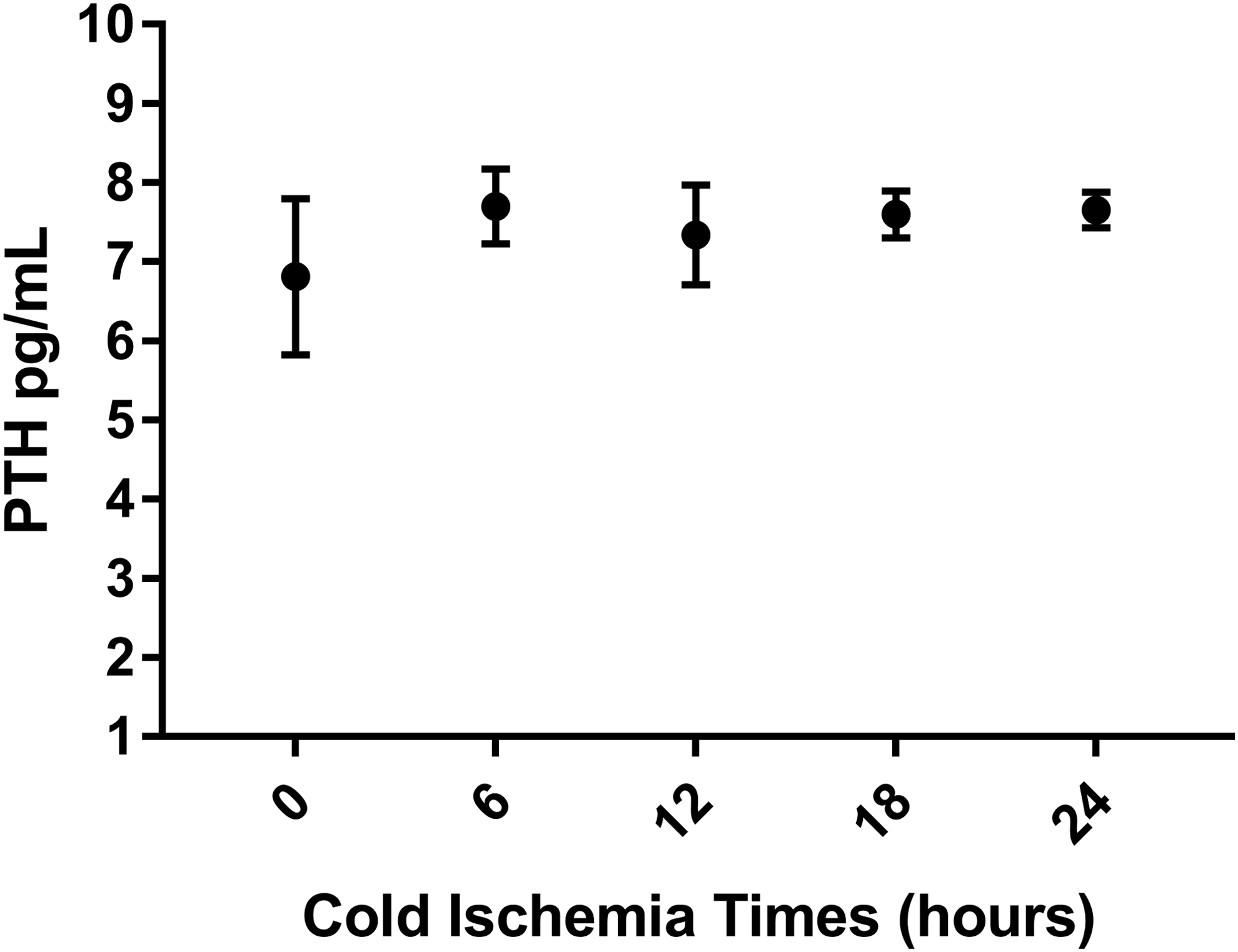
Comparison of parathyroid cell PTH release with different cold ischemia times (p = 0.0476). PTH, parathormone.
Discussion
The success of organ transplantation mainly depends on the duration of cold ischemia. 8 There are common problems with organ preservation solutions: high cost and variable survival rates. The variable survival rate usually changes depending on the type of organ being transplanted. 16 Another outcome that causes ischemic injury is cold ischemia. The impact of ischemic injury on the immune system, such as tissue damage, 17 inflammation, 18 and leukocyte adherence, 19 easily increases alloreactivity on the transplanted graft. In addition delayed graft function continues to be a persistent problem, but minimizing cold ischemia still is a significant target, despite wide-ranging research on the molecular and cellular level. 20 Considering organ-specific metabolism, important differences exist between intra-abdominal organs and endocrine glands. 8 Thus, this leads to each transplanted graft having different requirements for using cooling preservatives to slow biological deteriorations during cryopreservation.
One of the earliest research studies about cooling transplanted grafts whole (with heparinized or diluted blood) or partially (surface cooling) concluded that successful preservation requires acellular solutions. 21 The development of a new acellular solution provided significant improvements, which aimed to stabilize the intracellular electrolyte balance of the mammalian cells. 3
The parathyroid gland plays a central role in calcium metabolism by sensing the changes in extracellular calcium through CaSR. Parathyroid glands consist of chief, oxyphil, and water clear cells as well. Oxyphil and chief cells have CaSR on their surface, and both cells have mitochondrial content due to eosinophilic cytoplasm, thus suggesting the need for energy production for PTH release. 22
Nawrot et al. used Chang's medium C solution for parathyroid gland transportation and cell culture for allotransplantation of parathyroid cells. In the same study cell viability was reported to be more than 85%. 10 Furthermore, Aysan et al. used AmnioMAX II Complete Medium for transportation. 9 Resected parathyroid glands were cryopreserved for autotransplantation as well. Shepet et al. pooled the results of eight autotransplantation studies and showed that the success rate of autotransplantation was 23%. Cryopreservation of parathyroid glands demonstrated a time dependent loss of tissue viability during delayed autotransplantation. 23 An animal study using rats determined that the parathyroid gland cell viability after 7 days of culture was >80%. CaSR levels were not changed during cell culture, but PTH release was reduced to undetectable levels after 4 days. 24
Currently, the UW solution is the gold standard of preservation for many intra-abdominal organs.3,16 The extended preservation time for the pancreas went up to 19 hours, 25 the liver from 6 to 15 hours,26,27 the intestines from 6 to 10 hours (in vivo research),7,28 and the kidney at least 30 hours 29 demonstrating that they are suitable for cold preservation.3,7 However, some limitations were identified such as high viscosity, high molecular weight compounds, microcirculatory disturbances by undissolved particles, and the high cost 3 of the UW solution. 16 In addition, during cold storage mitochondrial protection is important for organ transplant outcomes. Under hypothermic conditions metabolic demand decreases as the shift from aerobic to anaerobic respiration through glycolysis occurs. Highly viscous organ preservation solutions like UW are linked to dysfunction of energy homeostasis during cold storage. 5
On this basis, it was hypothesized that the ideal transportation solution for parathyroid gland with NPTS could create a state in which cellular function and metabolism could be preserved for a long period of time before in vitro or transplantation processes. The ingredients in NPTS are mainly composed of amino acids, vitamins, inorganic salts, and other compounds like
Every ingredient has a unique and specific aim, for instance, amino acids provide raw material to synthesize proteins. Vitamins protect cell proliferation and act as cofactors to support cellular function outside the body. Inorganic salts are responsible for preserving the cellular membrane by blocking inhibitory agents. FBS controls the osmotic pressure, reduces mechanical stress on the gland, and stimulates vitality. HEPES acts as a pH stabilizer and slows down metabolism when the gland requires extended periods of manipulation outside the body, such as the process of cold ischemia. Sodium pyruvate is a carbon and energy source for the processing of glucose. Hypoxanthine and thymidine protect cells from disruption of the salvage pathway. Lipoic acid is added as a biological antioxidant which terminates a number of reactive oxygen species and reactive nitrogen species and also chelates redox active transition metals (e.g., iron, copper). As a trace element, selenium is a metabolic detoxifier and also a cofactor. The adjusted pH range of NPTS is 7.2–7.4, and the solution can be stored at +4°C for 1 year or at −20°C for 5 years.
Our findings suggest that NPTS appears to be effective for preserving parathyroid glands for allotransplantation and cryopreservation. Through this we examined the viability before and after cryopreservation, greater than 89.2% and 93.2%, respectively. However the majority of cells lost after cryopreservation was 13.8%. Loss of viable cells compared to the cell quantity before cryopreservation resulted in a reduced amount of cells from tissue. Nonetheless, cell loss starts with the isolation process as well. Therefore, even loss of cells either during isolation or cryopreservation would not affect the transplantation process and CaSR after 24 hours of storage in ice-cold NPTS. In addition, the parathyroid hormone level was significantly increased after cold storage, which can be linked to the necessity of cooling after removal of the glands during surgery. Cooling reduces mechanical stress, prevents hypoxic injury, and reduces cellular metabolism. 3
In conclusion, our study demonstrated that NPTS, designed by the Bezmialem Vakif University Parathyroid Transplantation Unit, is a low-cost solution that can keep parathyroid tissue functioning and viable outside the body for 24 hours. NPTS should be evaluated in comparison with other cold storage solutions such as UW, HTK, Celsior, Perfadex, Somah, as well as other intra-abdominal organs in a future clinical study.
Footnotes
Acknowledgments
The authors highly appreciate the efforts of Monica Ann Malt, MSN, RN, and CPAN (Bezmialem Vakif University, Turkey) in editing this article. The authors also thank the Microbiology Research Laboratory team M. Ziya Doymaz and Elif Karaaslan for equipment support.
Author Disclosure Statement
No conflicting financial interests exist.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.