
Abstract
Background:
Ex vivo cold storage of red blood cells (RBCs) for transfusion has long been associated with hypothermic storage lesions. It has been proposed that liposomes can be used to mitigate hemorheological elements of RBC membrane storage lesions. This study aimed to determine the appropriate liposome treatment time and assess the effects of liposome treatment on RBC's hemorheological and metabolic profiles.
Materials and Methods:
Unilamellar liposomes were synthesized to contain a bilayer of 1,2-dioleoyl-sn-glycero-3-phosphocholine (DOPC):cholesterol (7:3 mol%). Packed human RBCs (n = 4) were divided into untreated control (HEPES-NaCl solution) and liposome-treated samples (2 mM DOPC liposomes) and treated at days 2, 21, and 42 of hypothermic storage. RBC quality assessment included percent hemolysis, deformability, aggregation, hematological indices, microvesiculation, supernatant potassium, adenosine triphosphate (ATP), and 2,3-diphosphoglycerate (2,3-DPG).
Results:
Among the parameters affected by liposome treatment time were deformability, aggregation amplitude (Amp), mean corpuscular hemoglobin, mean corpuscular hemoglobin concentration, and microparticle mean fluorescence intensity. After 6 weeks of storage, aggregation index (AI) and Amp were significantly increased in liposome-treated RBCs (AI: 45.38 ± 1.92% vs. 41.54 ± 4.10%, p = 0.020; Amp: 16.38 ± 2.17 arbitrary units [au] vs. 12.22 ± 3.29 au, p = 0.019). Despite comparable hemolysis levels at 3 and 6 weeks, DOPC-treated RBCs showed significantly increased potassium levels for the same time points (3 weeks: 31.2 ± 2.7 mmol/L vs. 30.8 ± 2.7 mmol/L, p = 0.007; 6 weeks: 45.0 ± 3.0 mmol/L vs. 43.8 ± 3.4 mmol/L, p = 0.013). ATP and 2,3-DPG levels were comparable throughout storage.
Conclusions:
Liposome treatment seemed to be more beneficial when performed at the beginning of storage up to day 21. DOPC liposome treatment resulted in an improvement in human RBC hemorheology upon storage, with no significant impact on metabolic profile.
Introduction
E
Studies of HSL have concluded that the most significant changes start to happen between 2 and 3 weeks of storage (∼21 days), period after which, some changes become irreversible. For example, RBCs change shape after loss of membrane (discoid shape to spherocytes),3,4 and 2,3-diphosphoglycerate (2,3-DPG) is also no longer detectable after 2 weeks, although studies have shown that normal levels are restored within 72 hours of transfusion.5,6 Additive solutions provide RBCs with an excess of nutrients, substrates for metabolism, and membrane stabilizers that help maintain cellular structure and metabolism for longer periods (up to 6 weeks) during ex vivo storage. 7
One important topic of HSL not addressed by additive solutions and metabolic rejuvenation is the loss of phospholipid asymmetry that culminates in membrane loss. The loss of RBC membrane phospholipid asymmetry ultimately leads to phosphatidylserine (PS) externalization, which culminates in microparticle (MP) formation and release.8,9 Several mechanisms can be attributed to MP shedding from RBCs, including protein oxidation, 10 adenosine triphosphate (ATP) depletion,11,12 and increased intracellular Ca2+ concentrations. 13 Current strategies to preserve in vitro RBC quality before transfusion do not adequately address the loss and remodeling of the RBC membrane. Numerous studies using RBCs as membrane models have utilized liposomes as means for modifying the composition of membranes and have documented the effect of these manipulations.14,15
Liposomes have been shown to influence membrane fluidity and thermal phase behavior16,17 of human RBCs, but no studies have evaluated the effect of liposomes as a strategy for decreasing MP concentration or changing their composition during hypothermic storage (HS). The intent of liposome treatment is to provide a source of phospholipids for membrane renewal and conservation of phospholipid asymmetry since RBCs are not able to synthesize phospholipids and their in vivo source (lipoproteins) do not remain in the collection bag after whole blood is processed into packed RBCs. 18 Considering these facts, it is important to evaluate when the liposome treatment should be performed on human RBCs, so the cells would most benefit by the liposomal supply of phospholipids.
The impact of liposome treatment on hemorheology of rat RBCs has been previously described by our group 19 with an observation that 1,2-dioleoyl-sn-glycero-3-phosphocholine (DOPC) liposome treatment resulted in an overall improvement in rat RBC hemorheology upon storage. Therefore, it is important to evaluate if those effects remain true for human RBCs. In addition, there are no reports on the effect of membrane manipulations using liposomes on the metabolic profile of cells. With those observations in mind, the aim of this study was to evaluate the effect of liposome treatment time on human RBCs and to assess the effect of liposome treatment on hemorheology and metabolic profile of human RBCs using the same liposome formulation that rendered significant changes to rat RBCs. 19
Materials and Methods
RBC collection and manufacturing
This study was reviewed by both Canadian Blood Services (CBS) and the University of Alberta Research Ethics Board. Ten leukoreduced packed RBC units processed from whole blood collected in citrate-phosphate-dextrose and stored in saline-adenine-glucose-mannitol were obtained from the CBS Network Centre for Applied Development. 20
Liposome synthesis and treatment of RBCs
Multilamellar liposomal vesicles were prepared by the technique of Bangham and Horne 21 using phospholipids from Avanti Polar Lipids (Alabaster, AL) and cholesterol from Sigma-Aldrich (St. Louis, MO). Dry lipids were hydrated in HEPES-NaCl buffer containing 135 mM NaCl and 20 mM HEPES (pH 7.4, 276 mOsm/kg of H2O). Small liposomal unilamellar vesicles were obtained by extrusion using a Lipex™ extruder (Northern Lipids, Inc., Vancouver, BC) with 200 nm pore size Nuclepore® polycarbonate membranes (Whatman, Clifton, NJ). The mean Z-average size (nm) of the liposomes used in this study was determined using a Zetasizer Nano ZS (Malvern Instruments, Malvern, UK).
To examine the effect of liposome treatment time on human RBC in vitro quality, four leukoreduced Rh and ABO-matched packed RBC units were pooled and subsequently split to produce four equivalent RBC products. RBC aliquots (three sets of untreated controls and liposome-treated samples, n = 4 each) were treated at days 2, 21, and 42 of HS with a final assessment at day 45. The packed RBCs were incubated at 37°C with either HEPES-NaCl solution (untreated control) or 2 mM lipid DOPC liposomes. The in vitro quality of DOPC-treated RBCs and untreated RBCs was analyzed immediately after the liposome treatment and at days 42 and 45 of HS, as described below. To examine the effects of DOPC liposome treatment on RBC hemorheology, packed RBCs were incubated for 1 hour at 37°C with either HEPES-NaCl solution or 2 mM lipid from DOPC liposomes. The in vitro quality of DOPC RBCs (n = 6) and untreated RBCs (n = 6) was analyzed immediately after the liposome treatment and upon 3 and 6 weeks of HS, as described below.
In vitro RBC quality assessment
Hemolysis was measured using a Drabkin's-based method. 22 Percent hemolysis was calculated as a ratio of the supernatant hemoglobin (Hb) to the total Hb, with the hematocrit (Hct), measured by a microhematocrit method. 23 RBC hematological indices, including RBC count, the mean corpuscular volume (MCV), mean corpuscular hemoglobin (MCH), mean corpuscular hemoglobin concentration (MCHC), and Hb were determined using a cell counter (Coulter AcT; Beckman Coulter, New York, NY). 24 Supernatant potassium concentrations were measured by indirect potentiometry using ion-selective electrodes on a biochemistry analyzer (DXC 800; Beckman Coulter, Inc., Fullerton, CA). 24 ATP and 2,3-DPG concentrations were determined enzymatically using commercially available kits (DiaSys Diagnostic Systems GmbH, Holzheim, Germany and Roche Diagnostics GmbH, Germany, respectively), as previously described.25,26
RBC deformability was measured using a laser-assisted optical rotational cell analyzer (LORCA; Mechatronics, Zwaag, The Netherlands), as previously described. 27 RBCs were diluted 1:100 in a polyvinylpyrrolidone solution and subjected to increasing shear stress at 37°C. Deformability curves were linearized using an Eadie–Hofstee transformation to determine the maximum elongation index (EImax) as a measure of deformability and the stress required to reach half of the maximum elongation as a measure of rigidity (KEI).27,28
RBC aggregation was measured by syllectometry using LORCA (Mechatronics) as previously described. 28 RBCs were resuspended with 1% dextran-phosphate buffered saline (PBS) (100 kDa) solution to Hct of 42%–46%, while the controls were mixed with PBS (negative) and 3% dextran (positive). The laser backscatter intensity over time was measured for the following parameters: aggregation index (AI) in percentage (%), amplitude (Amp) in arbitrary units (au), and aggregation half-time (t1/2) in seconds (s). 29
Microvesiculation was measured by flow cytometry according to a previously described protocol. 25 Fluorescein isothiocyanate (FITC) anti-human CD235a antibody (MHGLA01; Invitrogen Life Technologies, Burlington, ON) was used as a marker for RBCs and MPs, while APC annexin V (BD PharMingen, San Jose, CA) was used to label PS. Labeled RBC samples were run on a FACSCalibur flow cytometer and data analyzed with CellQuest software (BD Biosciences, San Jose, CA). 25 Commercial isotype controls directed against glycophorin A (FITC mouse IgG1, k isotype control; BD PharMingen) were used to account for nonspecific antibody binding. 25
Statistical analyses
Statistical analyses were performed using SPSS 23.0 software (IBM, Armonk, NY). Two-way analysis of variance was used to assess the effect of treatment (untreated vs. liposome) and treatment time (days 2, 21, and 42) on in vitro quality parameters. When a significant interaction between treatment and treatment time was found, simple main effects were analyzed using Bonferroni's post hoc test. When no significant interaction was found, main effects were reported followed by Tukey's post hoc test when needed. Paired Student's t-test or Wilcoxon test was used to assess differences between liposome-treated RBCs and untreated RBCs over storage time. Data are expressed as mean ± standard deviation, and p < 0.05 was considered statistically significant.
Results
The effect of liposome treatment time on human RBC in vitro quality
The mean Z-average size (nm) of the synthesized unilamellar liposomes used in this study was 123.1 ± 2.1 nm. The effect of liposome treatment time on human RBC in vitro quality parameters is summarized in Table 1. No significant differences between treatment type or treatment time were detected overall for aggregation parameters AI (p = 0.356) and t1/2 (p = 0.321). As shown in Table 1, while there was no significant interaction between treatment type and treatment time for parameters EImax, KEI, Amp, MCH, MCHC, and microparticle mean fluorescence intensity (MP-MFI), a significant interaction between treatment type and treatment time for hemolysis, MCV, MP concentration, MP-PS%, and MP-MFI/MP-PS% was detected, so the results were subsequently reported after post hoc analysis and interpreted in the context of the interaction.
Treatment type (untreated vs. liposomes) and treatment time (days 2, 21, and 42) were fixed factors. Model p = p-value of the model, F-statistic and p-value are reported.
AI, aggregation index; Amp, amplitude; au, arbitrary units; EImax, maximum elongation index; KEI, rigidity; MCH, mean corpuscular hemoglobin; MCHC, mean corpuscular hemoglobin concentration; MCV, mean corpuscular volume; MFI, mean fluorescence intensity; MPs, microparticles; PS, phosphatidylserine; t1/2, aggregation half-time.
Table 2 summarizes RBC quality parameters affected by treatment time. Both deformability and rigidity of samples treated on days 2 and 21 were slightly lower compared to samples treated on day 42 (p < 0.001). Aggregation Amp was significantly lower on samples treated on day 2 compared to treated on day 42 (16.3 ± 0.3 vs. 17.3 ± 0.3, p = 0.037). Both MCH and MCHC of samples treated on day 2 were statistically significantly lower compared to samples treated on day 21. MP-MFI was significantly lower in samples treated at day 2 compared to day 21 (p = 0.010) and day 42 (p < 0.001) and on day 21 treatment compared to day 42 (p = 0.042). KEI was also affected by treatment type, with DOPC-treated RBCs demonstrating higher rigidity than untreated RBCs (2.25 ± 0.02 vs. 2.16 ± 0.02, p = 0.002). Aggregation Amp was affected by treatment type with DOPC-treated RBCs having higher Amp compared to untreated (17.2 ± 0.2 vs. 16.5 ± 0.2, p = 0.040).
Mean values ± standard error for samples treated on days 2, 21, and 42. Main effect of treatment time followed by post hoc analysis (Tukey's test).
Mean differs from days 2 and 21.
Mean differs from day 2 only.
All means differ from each other (p < 0.050 Tukey's test).
Table 3 summarizes simple effect analysis for RBC quality parameters where the interaction between treatment type and treatment time was significant. DOPC-treated RBCs had significantly lower hemolysis and MP-MFI/MP-PS% than untreated RBCs when treated at day 2 (p < 0.001) and day 21 (p < 0.001), but there was no difference between treatments at day 42 (p = 0.093 and 0.771, respectively). In contrast, DOPC-treated RBCs had significantly higher MCV, MP concentration, and MP-PS% than untreated RBCs when treated at day 2 (p < 0.001) and day 21 (p < 0.001), but there was no difference in MCV, MP concentration, and MP-PS% between treatments when RBCs were treated at day 42.
Mean value ± standard error for untreated and DOPC-treated RBCs treated on days 2, 21, and 42. Simple effects of treatment time × treatment type after post hoc analysis (Bonferroni's test).
DOPC, 1,2-dioleoyl-sn-glycero-3-phosphocholine; RBCs, red blood cells.
The effects of DOPC liposome treatment on human RBC hemorheology and metabolic content
Table 4 describes the hemorheology and metabolic parameters of liposome-treated and untreated RBCs, both immediately after treatment (fresh) and after 3 and 6 weeks of HS. Ektacytometry analysis showed no significant effect of liposome treatment on EImax in any of the time points evaluated. DOPC-treated RBCs showed increased rigidity immediately after treatment (KEI: 2.08 ± 0.27 vs. 1.84 ± 0.27, p = 0.040), which stabilized after 6 weeks of storage resulting in significantly lower values compared to the untreated group (KEI: 2.27 ± 0.33 vs. 2.39 ± 0.23, p = 0.048, Fig. 1). Syllectometry analysis showed a decrease in t1/2 of liposome-treated RBCs (3.4 ± 0.4 seconds vs. 3.8 ± 0.4 seconds, p = 0.046) immediately after treatment. After 6 weeks of storage, AI and Amp were significantly increased in liposome-treated RBCs (AI p = 0.020; Amp p = 0.019) while t1/2 was lower when compared to untreated (p = 0.035, Fig. 2). Although hemolysis was significantly lower immediately after treatment in the liposome group (0.15 ± 0.13% vs. 0.18 ± 0.14%, p = 0.042), a significant difference was not detected after 3 and 6 weeks of storage. Despite comparable hemolysis levels at 3 and 6 weeks, DOPC-treated RBCs showed significantly increased potassium levels for the aforementioned time points (3 weeks: 31.2 ± 2.7 mmol/L vs. 30.8 ± 2.7 mmol/L, p = 0.007; 6 weeks: 45.0 ± 3.0 mmol/L vs. 43.8 ± 3.4 mmol/L, p = 0.013). MCH was comparable between treatments throughout storage, while MCHC was slightly increased in DOPC-treated RBCs after 6 weeks of storage (306 ± 5 g/L vs. 302 ± 7 g/L, p = 0.003) and MCV was slightly decreased (96.5 ± 6.2 fL vs. 97.3 ± 6.4 fL, p = 0.028). 2,3-DPG levels were comparable throughout storage and no longer detectable after 6 weeks. ATP levels were initially comparable in both groups, but was slightly decreased in DOPC-treated RBCs compared to untreated RBCs after 6 weeks of storage (1.3 ± 0.5 μmol/g Hb vs. 1.7 ± 0.6 μmol/g Hb, p = 0.008).
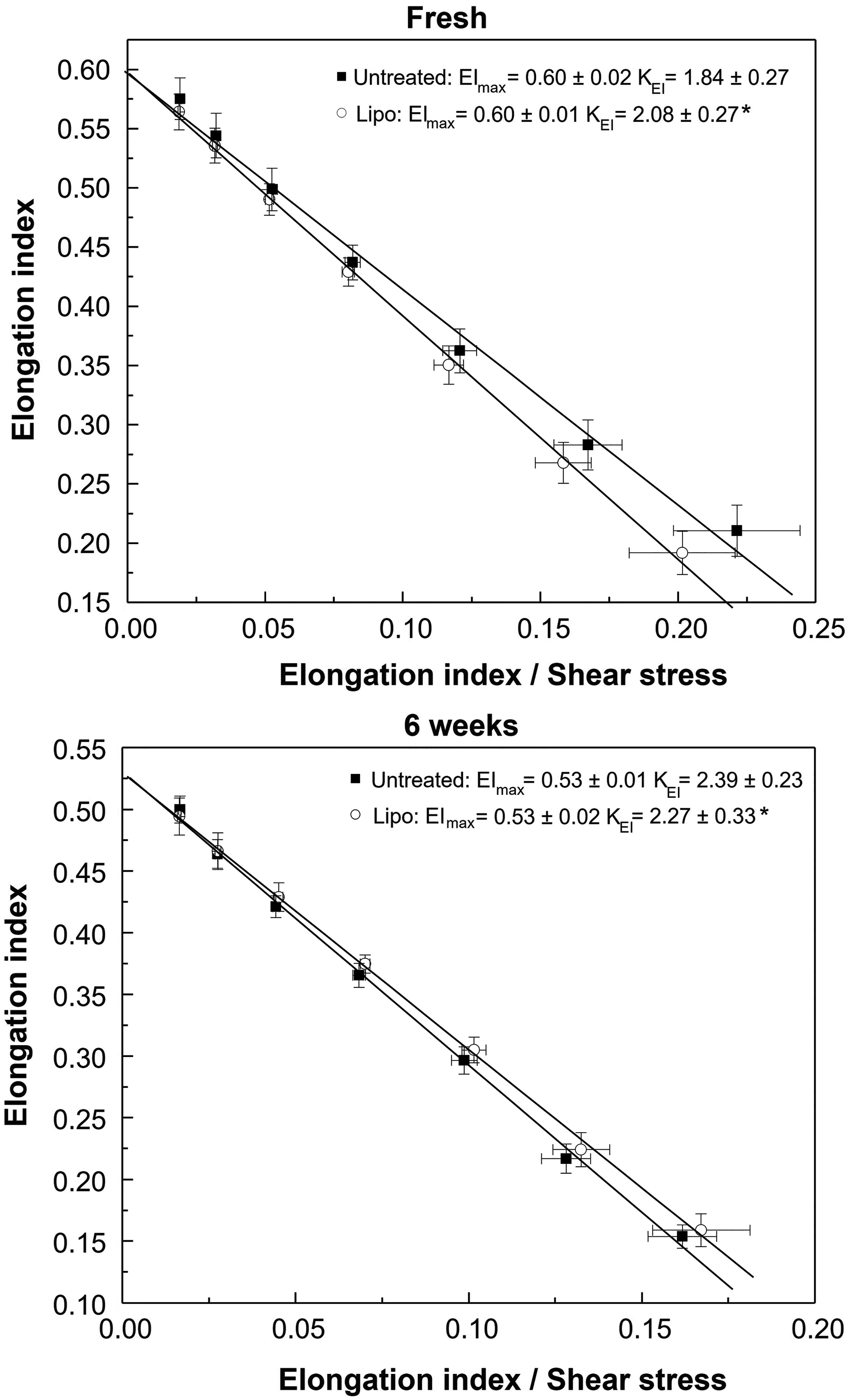
Deformability curves of fresh and stored DOPC-treated and untreated RBCs. EImax and KEI are shown (n = 6). *Significant (p < 0.05) compared to untreated RBCs of corresponding age. EImax, maximum elongation index; KEI, rigidity.
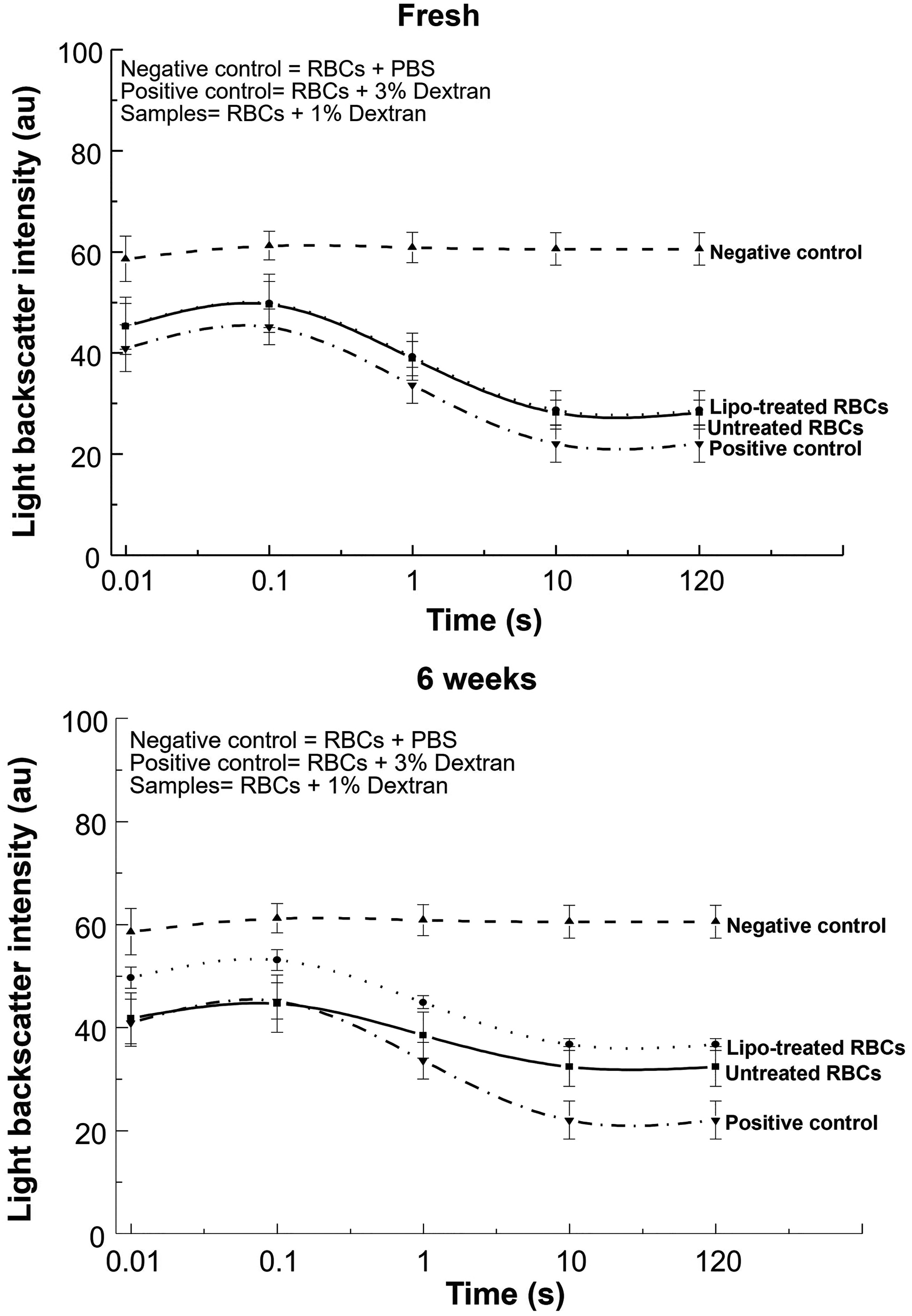
RBC aggregation in untreated and DOPC-treated RBCs (fresh and after 6 weeks of storage). Syllectograms (light scatter × time plots) showing RBC aggregation patterns (n = 6). Negative control (PBS) = no aggregation; Positive control (3% dextran) = high aggregation. PBS, phosphate buffered saline.
Mean value ± standard deviation for DOPC-treated and untreated RBCs immediately after treatment and after 3 and 6 weeks of hypothermic storage is shown.
p < 0.05 compared to untreated RBCs of corresponding age.
2,3-DPG, 2,3-diphosphoglycerate; Hb, hemoglobin.
Discussion
A liposome-based approach has been previously applied to rat RBCs, resulting in hemorheological improvements. As several elements of membrane storage lesion remain unaddressed by current RBC preservation approaches, it is important to examine the effects of liposome treatment on human RBC rheological properties and the metabolic profile.
The parameter least affected by liposome treatment was aggregation, with treatment time having no detectable effect on AI and kinetics (t1/2). High aggregation Amp could lead to impaired microcirculatory flow, and this hemorheologic alteration has been thought to contribute to the pathophysiology of slow coronary flow. 30 RBC deformability and rigidity (KEI) were both affected by liposome treatment time, although it is unlikely that such a small difference in deformability would have a significant clinical impact. Treatment type also had an impact on rigidity, with liposome-treated RBCs exhibiting slightly higher rigidity compared to untreated RBCs. Rigidity can be increased by the cholesterol content of RBC membrane, which is why patients with high cholesterol serum levels also present an increase in RBC rigidity. 31 The increase in RBC rigidity cannot be explained by cholesterol enrichment, as liposome formulation used in this study had a 0.4 cholesterol/phospholipid ratio, suggesting unlikely transfer of cholesterol from liposomes to RBCs.32–34 As other studies have shown the transfer of cholesterol from RBCs to liposomes, 17 the increase in rigidity could be linked to RBC membrane loss in the form of MPs or a change in the normal C/P ratio of the RBC membrane.
Hematological indices MCH and MCHC were slightly affected by treatment time, with lower MCH and MCHC values for samples treated on day 2 compared to later dates. Although a statistical significance was observed, values remained within the normal clinical reference ranges. 35 The decrease in RBC indices suggests less Hb in each RBC, regardless of their volume, which can be lost through membrane leak or bound to MPs.36,37 MCV was increased in DOPC-RBCs treated on days 2 and 21, but not day 42, while hemolysis decreased in DOPC-treated RBCs, suggesting that liposomes might have fused with the membrane or transferred enough phospholipids that caused the change in volume while decreasing hemolysis. 38 The type of liposomes used in this study would interact with RBCs by fusion, phospholipid transfer, or a combination of both, 38 so the demonstrated uptake of lipids could help stabilize cell membrane and compensate for lipid loss, translating in decreased hemolysis.
MFI of MPs increased as treatment time increased (days 42 > 21 > 2, Fig. 3). The time taken between PS exposure and MP release is not well known for RBCs, but in other cell types entering apoptosis it occurs within hours. 39 Considering that MP release is a time-dependent process, it is not surprising that samples treated at day 42 had lower MP concentration. MP concentration in DOPC-treated RBCs was significantly higher while inversely presenting higher MCV for the same treatment times.
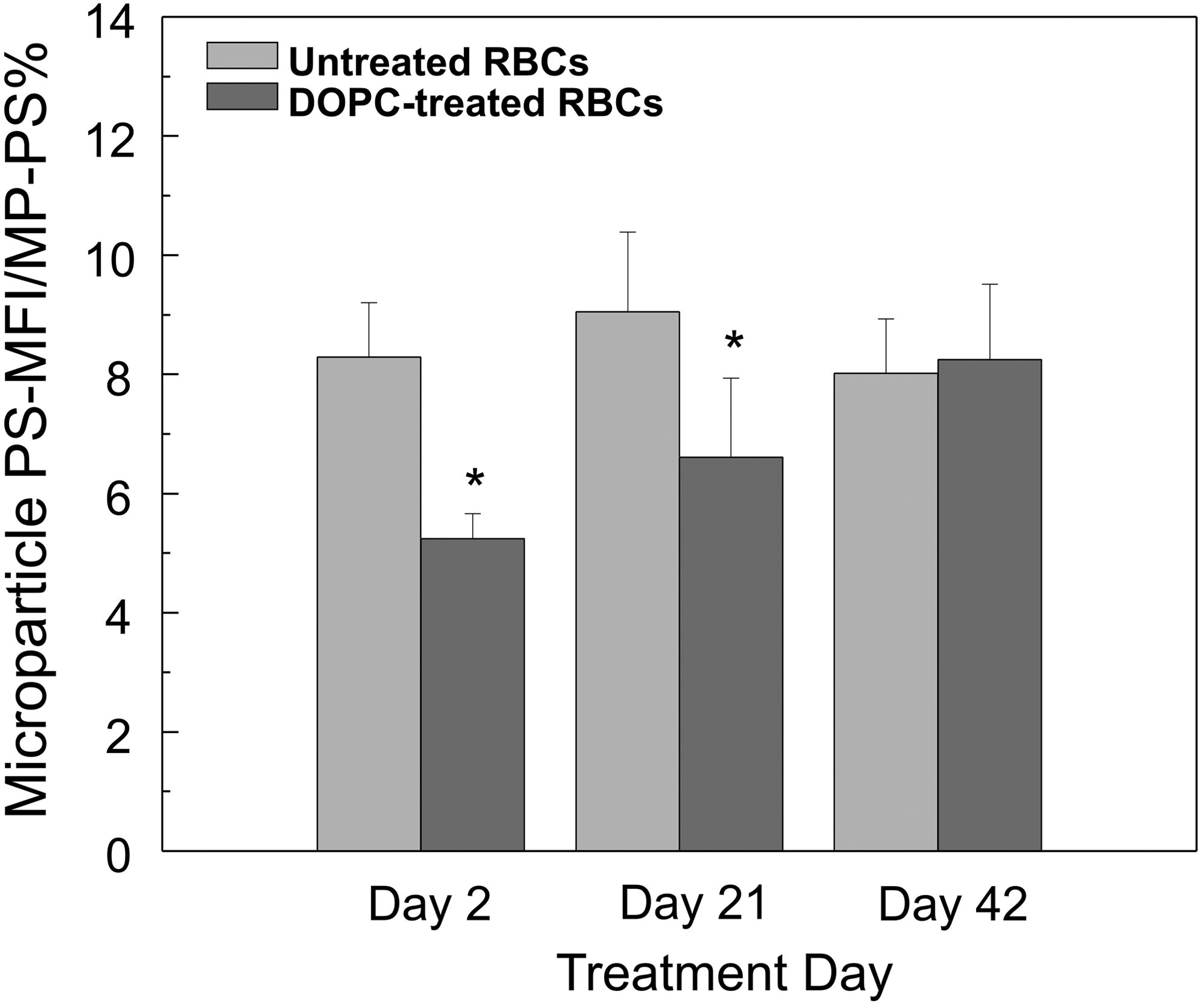
PS exposure MFI divided by percentage of PS (+) MPs in untreated and DOPC-treated MPs. Mean value ± standard deviation for untreated and DOPC-treated MPs treated at days 2, 21, and 42. *Significant (p < 0.05) compared to untreated MPs treated on the same day. DOPC, 1,2-dioleoyl-sn-glycero-3-phosphocholine; MFI, mean fluorescence intensity; MPs, microparticles; PS, phosphatidylserine; RBCs, red blood cells.
The DOPC liposomes used in this study, which were small unilamellar vesicles, neutral (not charged) and fluid (always kept above the crystallization temperature of the lipid) demonstrated a similar ability as we saw in rat RBCs in our previous studies 19 to reduce hemolysis immediately after treatment, although during 3- and 6-week assessments this effect was no longer observed. Inversely, supernatant potassium levels for 3 and 6 weeks of storage were slightly increased for DOPC-treated samples but still within the clinically acceptable ranges of previously reported RBC supernatant potassium at 42-day storage expiry of 46.2 ± 4.3 and 47.4 ± 4.0 mmol/L. 26
DOPC treatment increased the percent and extent of RBC aggregation while reducing aggregation time. Aggregation behavior that usually decreases with prolonged storage time seemed to be better preserved in DOPC-treated RBCs resembling values observed in fresh control RBCs. While the increase in the extent of aggregation might not seem of advantage, it is important to point out that although the Amp was increased by liposome treatment it remained within what has been reported for healthy individuals.30,40,41 Metabolic profile was not significantly altered by liposome treatment; no differences were observed for 2,3-DPG and only a slight decrease in ATP levels was detected after 6 weeks of storage in DOPC-treated samples, correlating to post-transfusion RBC viability toward the end of storage. 42
In conclusion, this study provides novel characterization of the liposome effect on in vitro quality of human RBCs. DOPC liposome treatment resulted in modest improvements in human RBC hemorheology upon storage, with no significant impact on metabolic profile. Liposome treatment seemed to be more beneficial when performed at the beginning of HS, up to day 21. Treatment at expiry (day 42) resulted in a lack of effect of liposome treatment on in vitro RBC quality parameters.
Footnotes
Acknowledgments
This article includes original material from a thesis in fulfillment of a PhD degree by Luciana Da Silveira Cavalcante, as granted by the University of Alberta, Edmonton, Alberta, Canada. The authors acknowledge Melissa Shyian for her technical assistance. This study was funded by the Canadian Blood Services Intramural Grant “Application of Liposomes to Improve the Hypothermic Storage of Red Blood Cells,” funded by the Federal, Provincial, and Territorial Ministries of Health. The views expressed herein do not represent the views of the federal government.
Author Disclosure Statement
No conflicting financial interests exist.