
Abstract
Background:
Molecular research is increasingly dependent on high-quality biobanked biospecimens. Preanalytical variables in tissue processing and preservation may influence the RNA quality and research results. Hence, the effect of long-term storage and clinicopathological parameters on RNA quality needs to be elucidated.
Methods:
Ninety gastric cancer tissue samples were collected and fresh-frozen in a −80°C freezer for 12 years (2006–2017). The histology was assessed and RNA integrity number (RIN) was detected by an Agilent 2100 Bioanalyzer. The impact of storage duration on RNA integrity and histomorphology was analyzed. The difference between RIN values and clinical variables was analyzed. Correlations between pathological parameters such as tumor cell percentage, stroma percentage, necrosis extent, cellularity, and RIN were assessed, respectively.
Results:
Long-term storage at −80°C for 12 years did not adversely affect RNA integrity and histomorphology. RNA integrity was also not influenced by tumor location, estimated blood loss, cold/warm ischemia time, and surgical approach. However, RIN values were significantly correlated with the tumor cell percentage and stroma percentage. Gastric cancer tissues with higher tumor cell percentage or lower stroma percentage had higher RIN values.
Conclusions:
RNA quality of fresh-frozen gastric cancer tissues is influenced by clinical and histological parameters. Standard tissue collection procedure and histological quality control remain essential for tissue biobanking.
Introduction
W
To collect high-quality biospecimens, standard operating procedures (SOPs) describing how to collect, operate, store, transport, and use biospecimens must be adhered to, and the quality of the samples assessed as a routine procedure. Ordinarily, a tissue biobank focuses on molecular integrity and tissue morphology. 5 In the current study, the integrity of fresh-frozen tissues was evaluated using the RNA integrity number (RIN) obtained using the Agilent 2100 Bioanalyzer. The RIN value was determined by the entire electrophoretic trace of the RNA sample, with a RIN of 10 representing the best quality, and a RIN of 0 indicating the most degraded RNA.6,7
In recent years, the impact of preanalytic variables on the quality of biological samples has gained more and more attention. The preanalytic phase involves all procedures from tissue sampling to gene expression analysis. These preanalytic variables may potentially affect the biospecimen quality and reproducibility of experimental results.8–10 Knowledge of these preanalytical variables is important to improve the reproducibility of experimental results and the consistency of sample application studies. However, very few studies have evaluated the influence of preanalytical parameters such as cold ischemia time, tumor location, estimated blood loss, and surgical approach on RNA quality of gastric cancer biospecimens.
The aim of the current study was to determine the impact of long-term storage on RNA quality and tissue morphology and to identify clinicopathological parameters that might influence RNA quality in gastric cancer tissues frozen in a −80°C freezer for 12 years (2006–2017).
Materials and Methods
Tissue samples
Tissue samples were collected from 90 patients who underwent surgery for gastric cancer at Taizhou Hospital of Zhejiang Province. The samples were frozen in the Taizhou human tissue bank (renamed Biological Resource Center since 2018) from January 2006 to December 2017. Eighty-four patients were not treated with chemotherapy or radiotherapy and six patients were treated with neoadjuvant chemotherapy before their operation. The informed consent for donation was obtained before surgery. The banking and use of the procured specimens were approved by the Tissue Bank Management Board and Ethics Committee of Taizhou Hospital of Zhejiang Province.
Tissue banking procedures
As soon as gastric resection was completed by the attending surgeon, the specimen was immediately transported in prearranged containers at room temperature to the pathology facility near the operation facility. After the personnel made a gross examination, the tissues were collected via the mirror image method. Ordinarily, collected tumor tissues were divided into three pieces: two for biobanking and one for mirror histological control.11–13 The mirror tissues were formalin fixed and paraffin embedded (FFPE) and then underwent routine histopathological processing. The results of histological examination were used to assess the other two corresponding tissue samples, which were stored in labeled cryovials, snap-frozen in liquid nitrogen, and transferred to a −80°C freezer for storage.
Histopathological assessment
For the histological assessment, 61 FFPE mirror blocks of malignant tissue samples were randomly selected and cut by a microtome into four-micrometer-thick sections, and the sections were placed on slides. The slides were baked for 30 minutes at 70°C in an oven and stained with hematoxylin and eosin (H&E). The stained slides were reviewed and assessed independently by two pathologists blinded to the patients' information. Cases with discrepancies were discussed together until a consensus was reached.
Tumor cell percentage was calculated as the percentage of tumor cell nuclei to all cell nuclei. Stroma percentage was calculated as the percentage of stromal cell nuclei to all cell nuclei. Necrosis percentage was evaluated and recorded as the percentage of necrosis among all cells on the slide. Cellularity was assessed as a semiquantitative analysis. On the basis of cellular density (including malignant and nonmalignant cells) of the entire section, cellularity was divided into three groups: low, moderate, and high, referring to the method reported by Galissier et al. 14
Total RNA isolation and RNA integrity detection
Ninety frozen gastric cancer tissue samples were used for total RNA isolation and RNA integrity detection. Each tissue sample was quickly removed from the −80°C freezer and weighed. Then, the sample was immediately placed in a mortar preloaded with liquid nitrogen. The tissue was ground to a fine powder using a pestle under liquid nitrogen. Then, the suspension was transferred (tissue powder and liquid nitrogen) into a liquid nitrogen-cooled, appropriately sized tube and the liquid nitrogen was allowed to evaporate without allowing the sample to thaw. Then, 1 mL of TRIzol reagent (Invitrogen, Carlsbad, CA) per 50–100 mg of tissue sample was immediately added in the tube and homogenized using a power homogenizer and violent shaking by hand.
RNA extraction was performed by the addition of chloroform for phase separation and isopropanol for RNA precipitation according to the manufacturer's instructions. Finally, RNA was eluted in RNase-free water. The extracted RNA was quantified by ultraviolet spectrophotometer (Eppendorf BioPhotometer, Germany) and analyzed using the RNA 6000 Nano Kit on the Agilent 2100 Bioanalyzer. RIN values were calculated by Agilent software, and RNA integrity was determined by the entire electrophoretic trace of the RNA sample.
Statistical analysis
Statistical analysis was performed with SPSS 23.0 software (SPSS, Chicago, IL). One-way ANOVA was applied to determine the difference between RIN and storage periods or tumor location or cellularity. The difference of RIN values and other clinical parameters was evaluated with the independent-sample t test. Correlations between histological parameters and RIN values were evaluated by Pearson's correlation tests. Statistical significance was defined as p < 0.05.
Results
Effect of storage duration on RNA quality and histomorphology
RNA integrity was assessed from 90 gastric cancer tissue samples fresh-frozen in a −80°C freezer for 12 years. None of the samples had undergone a freeze/thaw cycle. The mean RIN of 90 tissue samples was 6.58 ± 1.71 and median 7.0 (2.0–9.0). Overall, 81.1% (73 of 90) of all samples had an RIN of ≥6 and 86.7% (78 of 90) had an RIN of ≥5. As can be seen in Figure 1, there was no correlation between storage times and RIN values (p = 0.755).
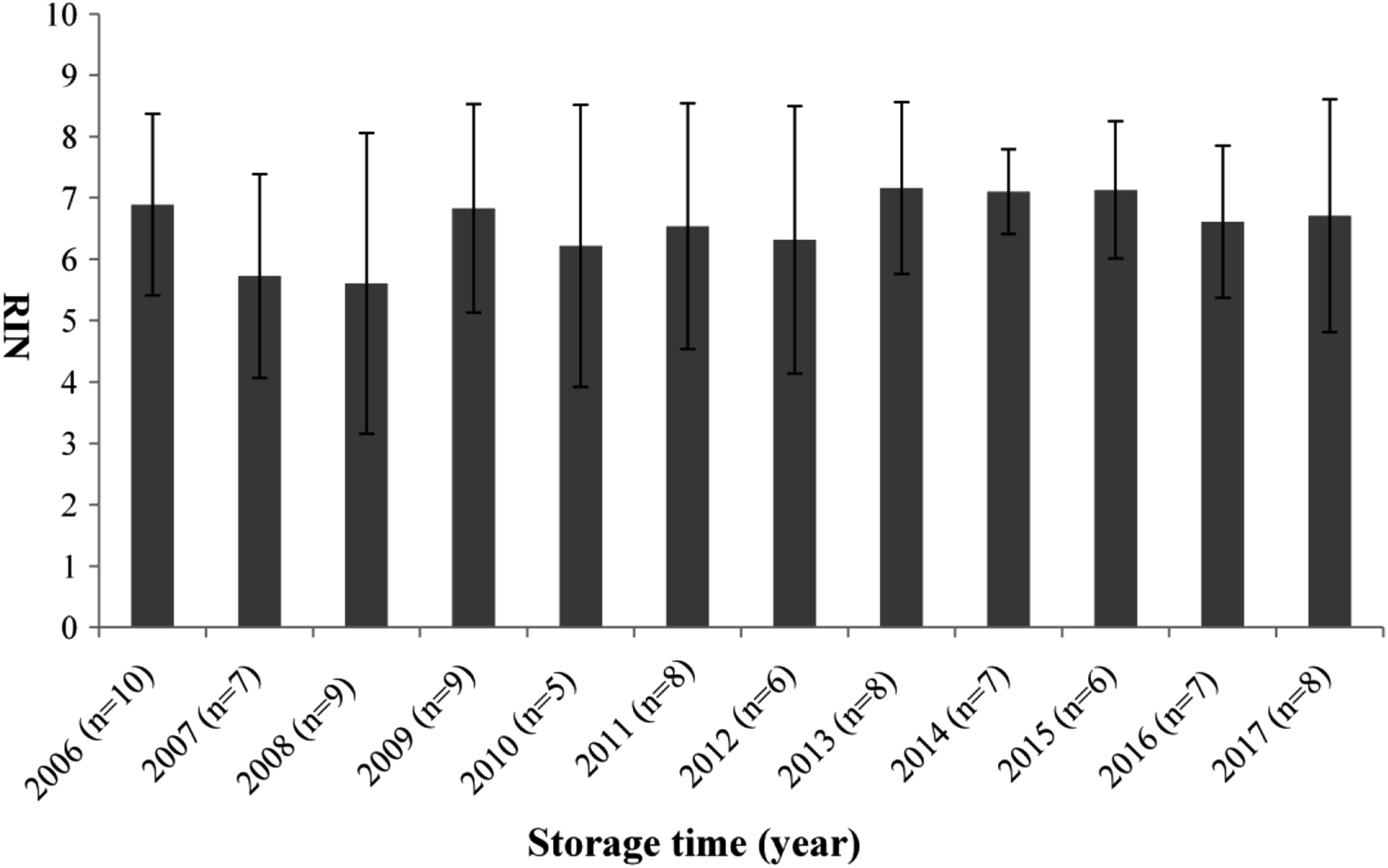
Mean RIN scores of gastric cancer tissues banked from 2006 to 2017. The error bars are standard deviation. RIN, RNA integrity number.
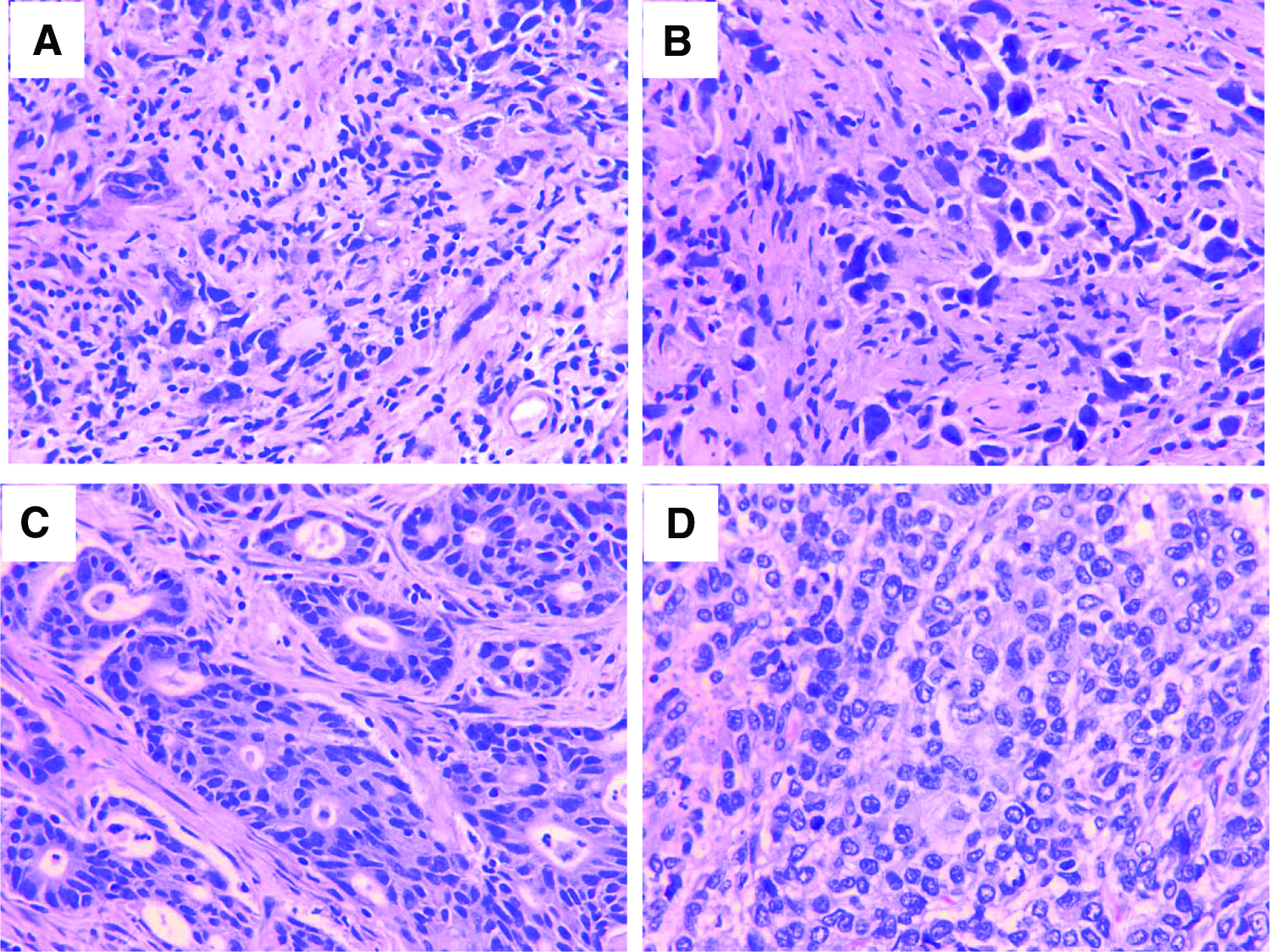
Sixty-one FFPE mirror blocks of malignant tissue samples were randomly selected, sectioned, and stained with H&E and the morphology was evaluated. All cases studied revealed “excellent” or “acceptable” tissue morphology. Representative photomicrographs of H&E-stained sections from four samples that were stored in −80°C for 2 years (RIN 3.6), 5 years (RIN 5.8), 7 years (RIN 6.3), and11 years (RIN 7.9) are shown in Figure 2. No obvious morphology changes were found in different storage times.
Clinical factors influencing RNA quality
Clinical and preanalytical factors associated with RIN are summarized in Table 1. There was no statistical difference between RIN values and the following clinical factors: age, sex, tumor location, estimated blood loss, surgical approach, and warm ischemia time.
Clinical Factors Associated with RNA Quality in Gastric Cancer Tissues
RIN, RNA integrity number.
When frozen tissues were collected, cold ischemia time of most of the samples was recorded according to our SOPs since September 2013. In the current article, cold ischemia time was recorded in 26 of 28 gastric cancer tissue samples collected from 2014 to 2017. The mean cold ischemia time of 26 samples was 22.9 ± 5.5 minutes. There was no statistical difference between cold ischemia time and RNA integrity.
Histological factors influencing RNA quality of tissues
The histology of gastric cancer tissues was evaluated, and the factors influencing RNA quality were analyzed. The correlations between RIN and histological parameters were analyzed and are shown in Figure 3.
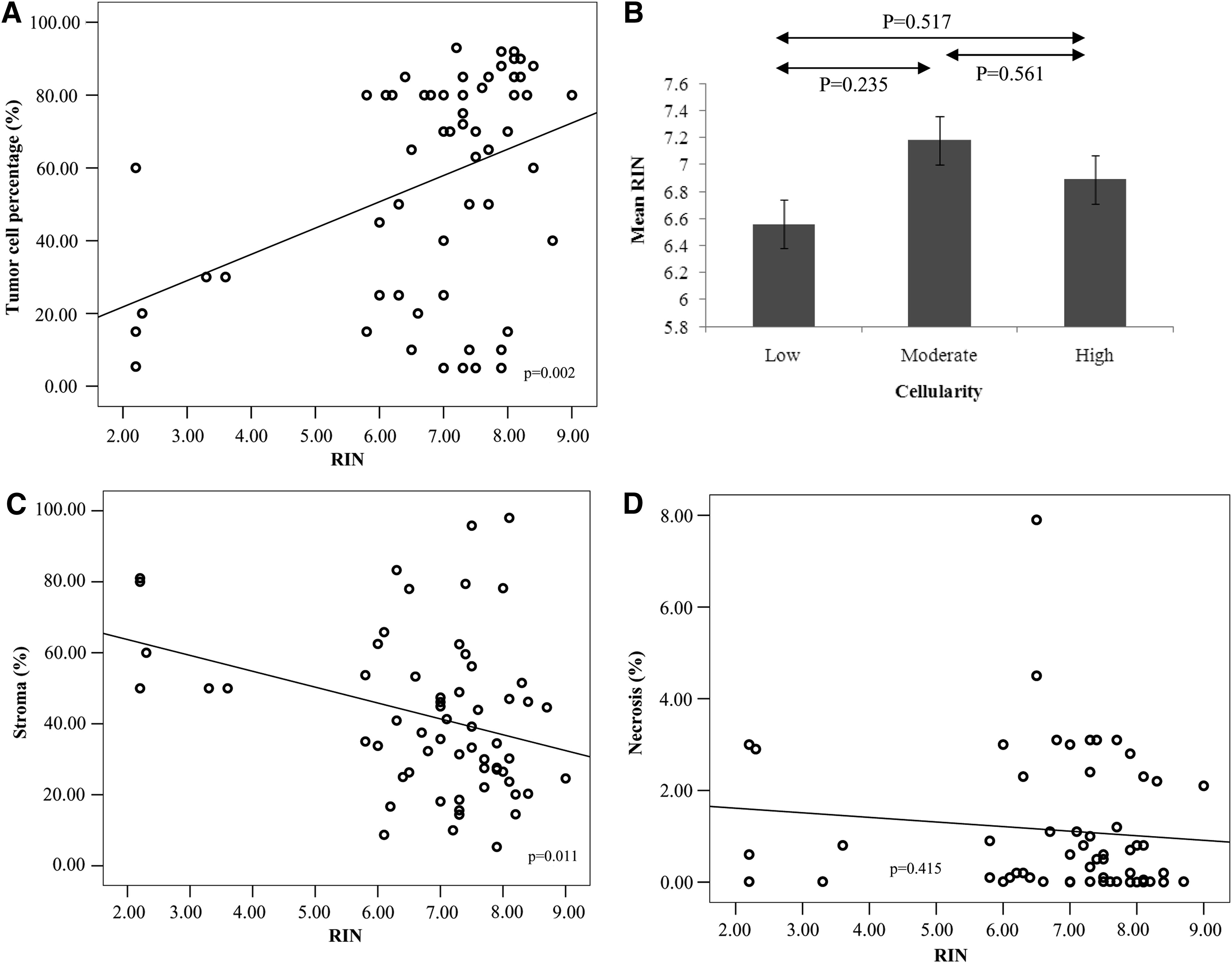
Correlations between histological parameters and RNA integrity in gastric cancer tissues.
The mirror blocks were examined and in 37 (60.7%) of 61 were detected tumor cell percentages higher than 60%. The results showed that significant correlation was found between RIN and tumor cell percentage (r = 0.385, p = 0.002). Gastric cancer tissues with higher tumor cell percentages had higher RIN values. In contrast, gastric cancer tissues with higher stroma extent had lower RIN values (r = −0.324, p = 0.011). Furthermore, the results indicated that RIN values were not influenced by the cellularity (F = 0.743, p = 0.48) and necrosis extent (r = −0.107, p = 0.415).
Discussion
The tissue bank was established in Taizhou Hospital of Zhejiang Province in 2004. 15 In this bank, tissues were collected based on SOPs provided by NCI Best Practices for Biospecimen Resources, and preanalytical variables were recorded during the collection, handling, and storage procedures of biospecimens. To ensure tissue quality before being released for research, quality control measures were implemented every year. In the current study, RNA was extracted and the integrity was evaluated from 90 gastric cancer tissue samples collected and frozen over a 12-year period. The impact of storage duration and clinical and histopathological parameters on RNA quality was analyzed. In previous studies, some parameters were evaluated in cancer biospecimens,16–18 especially colon cancer, but very few studies focused on gastric cancer. This is the first report on the impact of different clinical and pathological parameters on RNA quality of fresh-frozen gastric cancer tissues.
We found that long-term −80°C storage for 12 years did not influence RNA integrity and histomorphology of gastric cancer tissues. Several previous studies had also reported that long-term storage at −80°C did not adversely affect RNA quality in 102 colon samples for 40 months, 82 pancreatic tissues for 7 years, 549 thyroid biospecimens for 11 years, or 153 endocrine tissues for 27 years.19–22 This study suggested that although the preservation temperature is higher than the glass transition (Tg) temperature of water (−135°C), 23 at which detectable enzymatic activity probably ceases, the RNA quality of tissue biospecimens frozen at −80°C freezer is still stable.
In the present study, the histological assessment was completed by the mirror image protocol.11–13 This technique analyzed the tissue next to the frozen tissues and not the frozen tissue itself. Nevertheless, the histology of the mirror tissue significantly correlated with the frozen tissue.24,25 Therefore, the histological results of the mirror image paraffin blocks can be used to assess the other corresponding tissues next to the mirror samples, which were stored in a −80°C freezer. The mirror blocks were examined and the histological parameters were evaluated. We found there were significant correlations between RNA integrity and tumor cell percentage or stroma percentage. Higher RIN values were observed in samples with higher tumor cell percentage or lower stroma percentage. The study on the tumor cell percentage and RIN was consistent with a previous report in biobanked rectal cancer tissues. 16 However, discrepant results were observed in another study on colon cancer. In that study, RNA Quality Index values were higher in samples with lower malignant/stromal cell ratio. This could be because stromal cells maintain a kind of homeostasis to prevent RNA degradation in colon cancer. 14 Furthermore, several studies have reported that mucosa or stroma tissues had lower RIN values. In one study, Bertilsson et al. stated that higher RIN values were found in the tissues with more epithelium than the extracts from tissues with a high proportion of the prostate stroma. 17 Fleige and Pfaffl also observed a lower RIN in extracts from connective tissue-rich organs than that from more cellular organs. 18 The correlation between the tumor cell percentage or stroma extent and RIN values indicated that the collection of representative tissues, avoiding the most stroma- or necrosis-rich samples, is the key for high-quality biobanking. Morente et al. highlighted the importance of histological representativeness. 26 Sandusky et al. proposed that the tissues with a tumor cell percentage higher than 65% were suitable for distribution to researchers for genomic and proteomic analysis. 27 The Cancer Genome Atlas (TCGA) recommends using samples with more than 60% of malignant cells to ensure that the gene expression results reflect the tumor cell results and not the stromal cell results. 28 Furthermore, necrosis extent was usually evaluated to assess biospecimen quality. The maximal necrosis extent threshold is 20% in TCGA studies. 28 In our study, necrosis extent had no significant influence on RNA quality as in another study. 14
In addition to the histological parameters, the difference between clinical variables and RIN was also analyzed in our study. No significant difference was observed between the RIN values and clinical variables, including sex, age, tumor location, surgical approach, or estimated blood loss. In contrast, Bertilsson et al. found that the impact of blood loss on RIN value was statistically significant and lower RINs were observed with higher estimated blood loss in prostate tissue from patients undergoing radical prostatectomy. 17 This might be due to the obviously different blood loss volume in patients with gastric cancer surgery and radical prostatectomy. In our study, the patients lost between 20 and 500 mL, while in that study the majority of patients lost between 500 and 1000 mL and some of patients lost between 1000 and 3000 mL. Massive bleeding during surgery, resulting in increased RNAase activity and RNA degradation could be a plausible explanation.
In our bank, as soon as gastric tissue resection was completed by the tissue bank assistant, the tissue specimens were immediately collected and snap-frozen in liquid nitrogen within 30 minutes to decrease the effect of cold ischemia time on RNA quality and the gene expression profile. In the current study, we found that cold ischemia time had no significant impact on RNA quality. The result was consistent with several prior studies. In one study of colon cancer, RNA integrity was not obviously influenced by cold ischemia for up to four hours in tissues. 19 Recently, Song et al. also reported that RNA is stable independent of fresh-frozen cancer tissue type with less than 1 hour of cold ischemia time. 29 However, on the contrary, several other researchers reported that with the prolongation of cold ischemia time, RNA integrity significantly decreased in colorectal cancer tissues.30,31
In this article, only 86.7% of frozen gastric cancer samples had a RIN of ≥5. The results were similar to one previous article. 14 Zeugner et al. reported that samples from the gastrointestinal tract had lower RIN values than samples from other organs. 9 However, Song et al. found only three samples showed an RIN of <7of a total of 396 various types of cancer tissues, and Bao et al. also reported that 94% had a RIN of ≥7 in colon cancer tissues with tumor cell content higher than 70%.29,19 This difference might partly be explained by some preanalytical factors such as tissue collection, ischemia times, surgical procedure, or RNA extraction procedure.
Moreover, in the present study, RINs were used as the sole measure to determine RNA integrity. As we know, RINs are heavily based on the relative degradative states of the 18S and 28S rRNA peaks and are therefore principally a measure of rRNA integrity. Mathieson et al. had reported the samples with equally low RINs but radically different mRNA integrity, assessed using PCR for different amplicon lengths. 21 Therefore, one limitation to this study is that only RINs were detected for RNA integrity and direct assessment of mRNA integrity by qRT-PCR or other methods has not been carried out.
In summary, we evaluated the RNA quality of gastric cancer tissues fresh-frozen at the biological resource center for 12 years. The impact of the storage duration and clinicopathological parameters on RNA integrity was analyzed. RIN was significantly correlated with the tumor cell percentage or stroma percentage. However, RNA quality was not influenced by long-term storage at −80°C, ischemia time, and other clinicopathological parameters. The research indicated that detailed diagnostic and histopathological information would be useful to screen tissue samples that should be checked for their RNA quality. Standard collection procedure and histological quality control remain essential for tissue biobanking.
Footnotes
Acknowledgments
This work was supported by grants from the National Natural Science Foundation of China (31370920 and 81372247), the Zhejiang Provincial Program for the Cultivation of High-level Innovative Health Talents, and the National Human Genetic Resources Sharing Service Platform (2005DKA21300).
Author Disclosure Statement
No conflicting financial interests exist.