
Abstract
Background:
The preservation of placental and fetal tissues will contribute to studying the pathogenesis of high-risk pregnancy diseases. However, few studies have focused on the effects of different preservation methods and cold ischemia time (CIT) on the quality of nucleic acids. An available quality control (QC) strategy will be beneficial to evaluate these effects for high-risk pregnancy biobanks.
Methods:
We established an evaluation strategy of nucleic acid QC by analyzing total RNA and genomic DNA (gDNA). Through this strategy, the effects of CIT, cryoprotectants (CPAs), and freeze/thaw cycles on the yield and integrity of placental RNA were analyzed. In addition, the effects of CIT on the yield and integrity of fetal DNA were determined.
Results:
For placental samples, there was no significant difference in RNA integrity (CIT <2 hours). After several freeze/thaw cycles, the RNA quality number values of placental samples in the CPA-free group and in the RNasin (TRIzol) group were decreased. For fetal samples, the DNA integrity of different organs (CIT <24 hours) was completely satisfactory, but it declined with the extension of CIT. Furthermore, different organs had different tolerances to cold ischemia, and the rank was as follows: skin, heart, liver, and placenta. In addition, the content of medium-length (600 bp) and long (1310 bp) fragments of gDNA were mainly reduced with the extension of CIT.
Conclusion:
The RNA integrity of placental tissue was affected by CIT significantly. It is recommended that placenta should be cryopreserved within 2 hours (4°C) from isolation. To ensure DNA quality of fetal tissues, the samples are suggested to be frozen within 24 hours (4°C) from isolation. On the contrary, if samples have a long CIT, skin is superior to other organs in the aspect of biobanking donor's genetic information.
Introduction
H
At present, perinatal biobanks of high-risk pregnancy in China are not common. The Biobank of Nanjing Drum Tower Hospital has cooperated with the Department of Obstetrics and Gynecology to collect maternal and fetal samples of high-risk pregnancies to provide researchers with reliable human tissues for molecular biology research since July 2015. However, due to the limitation of the financing and manpower, it is unrealistic to extract DNA and RNA from fresh tissue. Therefore, it is of great significance to choose appropriate preservation methods to guarantee quality of these samples.
Cryopreservation is the most common method of preservation, and preanalytic variables such as ischemia time and processing methods may affect the quality of frozen tissues. 9 In this article, we analyzed yield, purity, and integrity of nucleic acid samples from high-risk pregnancies to establish a workable quality control (QC) strategy. Because higher quality RNA can be obtained with a lower cold ischemia time (CIT) (when the tissues were separated from donors until samples were retrieved), we chose placental samples that were collected in a timely manner for RNA research. DNA has a tendency to be more stable even with longer CIT, and fetal samples for autopsy were selected for DNA research. Then, the effect of CIT and different storage methods on the quality of RNA and DNA from different samples was explored to optimize collection and preservation programs.
Materials and Methods
Ethics
The samples were delivered from the Biobank of Nanjing Drum Tower Hospital. The acts of collection and research were approved by the Ethics Committee of Nanjing Drum Tower Hospital. The enrolled women (1) were older than 18 years and diagnosed with high-risk pregnancy; (2) were of single gestation; (3) whose gestational age was more than 20 weeks; (4) whose fetuses were alive before induced abortion, delivery, or induced labor; (5) could understand informed consent and were willing to sign the documents.
Processing and preservation of tissues
Placental tissues
All the enrolled women volunteered to sign the informed consent. The fresh placentas were sent to the biopsy room of our biobank in special transfer containers (4°C) as soon as the tissues were isolated and they were kept at 4°C before processing. In accordance with the needs of downstream analyses, placentas were cut into pieces from the decidual membrane surface to embryonic membrane surface and then processed as follows: (1) fresh tissues: pieces within 1 hour from isolation were used for RNA extraction directly and immediately; (2) cryoprotectant (CPA)-free samples: pieces were cut into aliquots of 0.5 × 0.5 × 0.5 cm and stored in empty cryogenic vials without CPAs. Each aliquot was placed in liquid nitrogen immediately and transferred into −80°C after fixation of 12 hours for long-term preservation; (3) RNAlater samples: pieces were cut into aliquots in size of 0.5 × 0.5 × 0.5 cm and minced into cryogenic vials with RNAlater (10 volumes of tissues). Each aliquot was fixed at 4°C for 12 hours and transferred into −80°C for long-term preservation; (4) TRIzol samples: pieces were cut into aliquots in size of 0.5 × 0.5 × 0.5 cm and weighed. The tissue (45 mg) was pulverized with 1 mL of TRIzol reagent in a pestle and mortar containing liquid nitrogen. Each aliquot was stored in empty cryogenic vials and placed into liquid nitrogen immediately. After fixation of 12 hours, they were transferred into −80°C for long-term preservation.
In this article, a total of 108 CPA-free placental samples were analyzed for the effect of CIT on placental samples. According to CIT, samples were divided into six groups, including Group A (0–1 hour), Group B (1–2 hours), Group C (2–4 hours), Group D (4–8 hours), Group E (8–12 hours), and Group F (12–24 hours). On the contrary, 18 placental tissues (from 18 donors) of which the CIT was within 0.5 hour were selected. Each tissue was cut into one T0 sample (fresh sample without frozen and thawed, CIT <0.5 hour) and three frozen samples. T0 samples were processed for RNA extraction immediately without being frozen. Frozen samples were cryopreserved with RNAlater, TRIzol, and without any CPAs as in the corresponding methods above. A freeze/thaw cycle was completed when the frozen samples were melted at room temperature. T1, T2, T3 referred to samples that were frozen and thawed once, twice, and three times, respectively.
Fetal tissues
Fetal tissues were derived from dead fetuses of which legal guardians applied for autopsy and signed the informed consent. Fetuses were transferred to the department of pathology in special transfer containers (4°C) and kept at 4°C before processing. Pathologists separated the myocardium (from left ventricle), liver, placenta, and skin. Biobankers cut organs into pieces in the size of 0.5 × 0.5 × 0.5 cm and kept at −80°C for long-term storage. According to the CIT, 35 donors were selected and divided into 7 groups, including Group G (0–12 hours), Group H (12–18 hours), Group I (18–24 hours), Group J (24–48 hours), Group K (48–72 hours), Group L (72–96 hours). and Group M (96–120 hours), respectively. Each group had five donors and each sample of each organ from each donor was collected. A total of 140 frozen samples were used for DNA QC. The fresh blood samples (CIT <0.5 hour) in the control group were derived from the other healthy pregnant women.
Extraction and analysis of nucleic acid
RNA extraction of placenta
Fresh samples, CPA-free samples, and RNAlater samples were weighed and ground in liquid nitrogen, respectively. Each 45 mg of tissue was immersed into 1 mL TRIzol reagent (Life Technologies) and then RNA was extracted in accordance with references. 10 TRIzol samples were incubated at room temperature for 5 minutes and then RNA was extracted as in the above references.
Extraction of genomic DNA
The fetal samples were weighed and treated with the E.Z.N.A. Tissue DNA Kit (Omega, Shanghai, China) to extract genomic DNA (gDNA). The procedures were carried out with the kit specifications. Fresh blood samples of the control group were treated with the E.Z.N.A. Blood DNA Kit (Omega, Shanghai, China) to extract gDNA by following the manufacturer's instructions.
Detection of concentration and purity
The concentration and purity of nucleic acid were detected by the μdrop plate of Skanit software 4.1 (Thermo Fisher Scientific, MA). The A260/A280 ratios and A260/A230 ratios were used as indicators for purity.
Detection of RNA integrity
The quality of RNA was assessed by using Qsep100 Automatic Nucleic Acid and Protein Analysis System (Bioptic, New Taipei City, Taiwan). The RNA was diluted to 50 ng/μL and analyzed directly with an RNA capillary cartridge in the method of rapid capillary gel electrophoresis. The result images contained three areas: 28S area, 18S area, and pre-18S area (including tRNA, 5 sRNA, and snRNA), respectively. The RNA integrity was calculated and analyzed as an RNA quality value (RNA quality number [RQN]) automatically. The RQN was similar to the RNA integrity number (RIN) and ranged from 1 to 10. The higher the value, the better the RNA integrity would be.
Detection of DNA integrity
The DNA fragments of ACTIN/X7 (1310 bp), AF4/X3 (600 bp), AF4/X11 (400 bp), PLZF/X1 (300 bp), RAG-1/X2 (200 bp), and TBXAS1/X9 (100 bp) 11 were amplified by HotStarTaq Plus DNA Polymerase (Qiagen, Shanghai, China). The reaction system was as follows: 10 × Taq polymerase buffer 2 μL; dNTPs (2.5 mM) 2 μL; MgCl2 (25 mM) 1 μL; mixed primers (0.2 μM of each) 2 μL; DNA template 120 ng; Taq DNA polymerase 0.5 μL; and appropriate RNase-free H2O. Polymerase chain reaction (PCR) was performed using the following conditions: initial denaturation at 95°C for 10 minutes, followed by 37 cycles of denaturing at 94°C for 30 seconds, annealing at 57°C for 30 seconds, extension at 72°C for 30 seconds, and final extension at 72°C for 7 minutes. The PCR products were diluted 20-fold for detection. Rapid capillary gel electrophoresis analysis of the PCR products was accomplished in a single-channel capillary cartridge by the Qsep100 system. 12 The detection conditions were as follows: sample injection: 2 kv/10 s; separation detection: 8 kv/200 s.
Data analysis
The RQN values between two groups were compared using Student's t-test. The DNA yield and purity between different organs and CIT groups were analyzed by using one-way analysis of variance (ANOVA). The RNA yield and purity between CIT groups were also analyzed by using one-way ANOVA. All statistical analyses were done using the Statistical Package for the Social Sciences software version 17.0 (SPSS, Inc.), and statistical significance was set at p < 0.05. The change curve of each group was drawn and analyzed by GraphPad Prism software 5.0.
Results
Analysis of RNA quality of placental tissues
Effect of CIT on quality of placental RNA
The RNA was extracted to detect the yield, purity, and integrity. There was no statistical difference of A260/A280 ratios and A260/A230 ratios (Supplementary Table S1) in each CIT group. The RQN values were calculated by the content of the 18S area and 28S area (Fig. 1). There was no statistical difference in RQN values between Group A and Group B. The RQN values of Group C, D, E, and F were, respectively, compared with the ones of Group A, and the differences were statistically significant (Fig. 2 and Table 1).
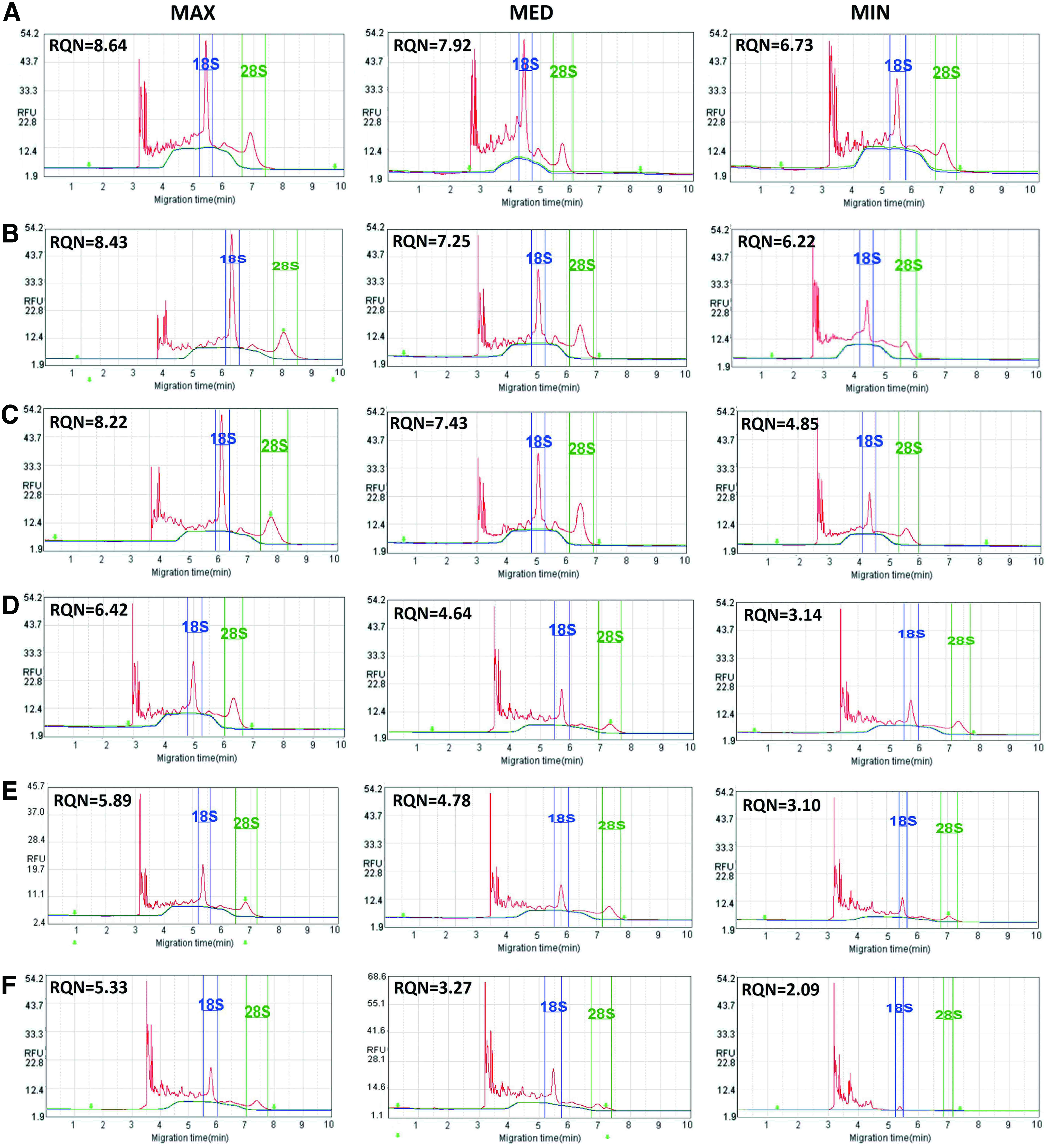
RNA electrophoresis analysis of placental samples in different CIT groups by Qsep100 system.

RQN values of placental samples in different CIT groups.
RNA Unit Yield, RNA Quality Number Values of Placenta in Different Cold Ischemia Time Groups
N is the size of samples, D is the number of donors; RNA unit yield = RNA total yield of each sample (ng)/sample amount (mg); p1 represents the p-value of RNA unit yield between six different CIT groups; p2 represents p-values of RQN between other five different CIT groups compared with Group A.
CIT, cold ischemia time; RQN, RNA quality number.
Effect of freeze/thaw cycles on RNA integrity of placental samples by different preservation methods
The placental samples (CIT <1 hour) were used for freeze/thaw experiments. The results showed that the RQN values of CPA-free samples and TRIzol samples were reduced after freeze/thaw cycles. There were statistical differences between the T2, T3, and T0 samples (p < 0.05). For RNAlater samples, the effect of freeze/thaw cycles on RQN values was not statistically significant (Fig. 3 and Table 2).
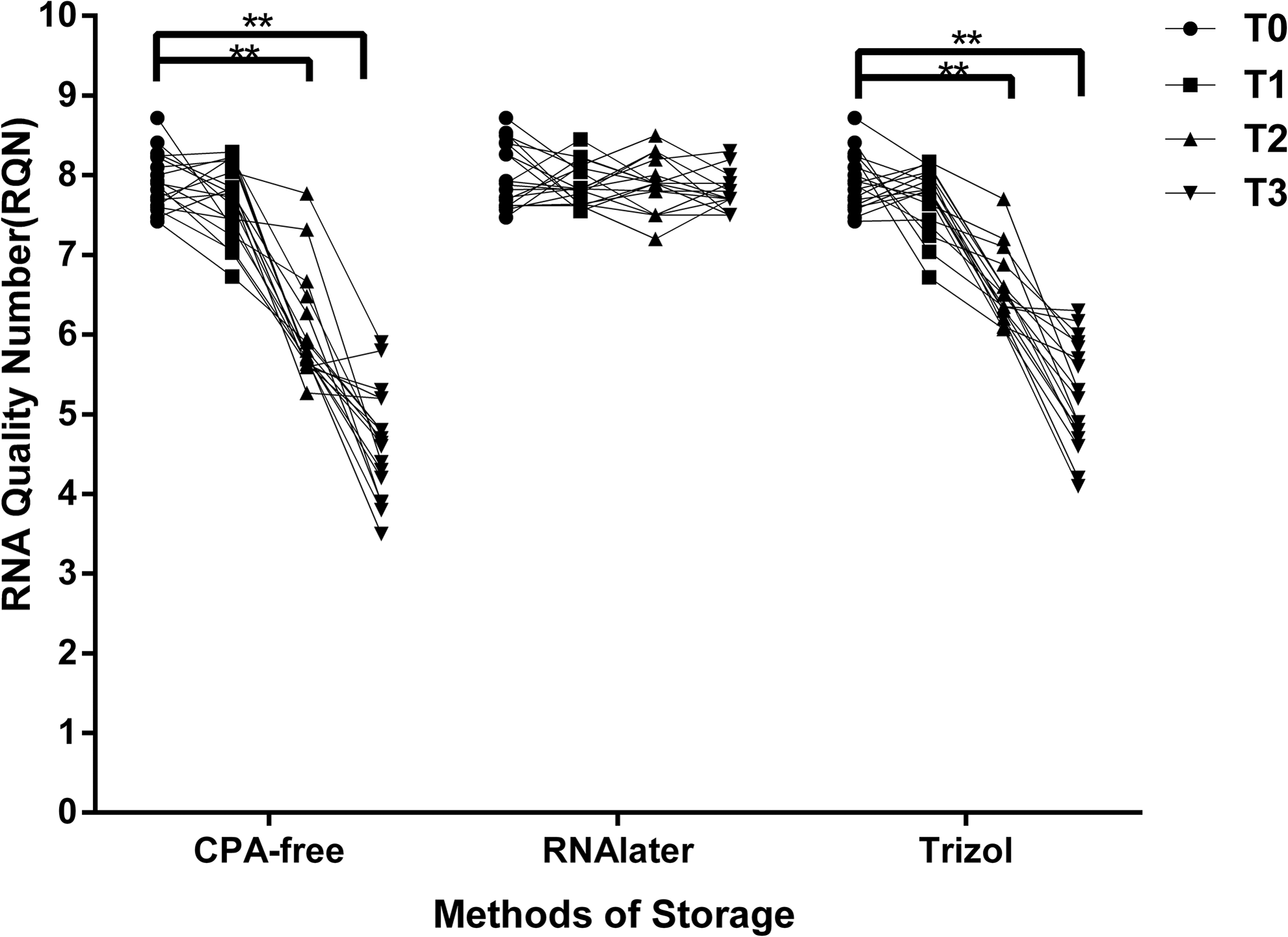
RQN values of placental samples in different storage methods after different freezing/thawing cycles. T1, T2, and T3 denote the samples were frozen and thawn out once, twice, and three times, respectively. T0 denotes fresh samples of which CIT was 0.5 hour. **p < 0.01. The sample size of each group was 18.
Effect of Freezing and Thawing Cycles on RNA Quality Number Values of Placenta Samples Frozen in Different Methods
N is the number of samples; T0 represents fresh samples without freezing and thawing; T1, T2, T3 represent samples that were frozen and thawn out once, twice, or three times, respectively. p1, p2, p3 represent p-values of RQN between T0 and T1, T0 and T2, T0 and T3, respectively.
CPA, cryoprotectant.
Analysis of DNA quality of fetal tissues
Detection of gDNA purity and yield
Fetal DNA QC was performed on the myocardium (from left ventricle), liver, skin, and placental tissue samples. The gDNA of samples in Group G, H, I, J, K, L, and M were analyzed for purity and yield. The results showed that the purity and yield of the same organ in different CIT groups were not statistically significant, while there were statistical differences of organs in the same CIT group (p < 0.05). The order of the yield went as follows: liver, placenta, heart, and skin (Fig. 4 and Table 3).
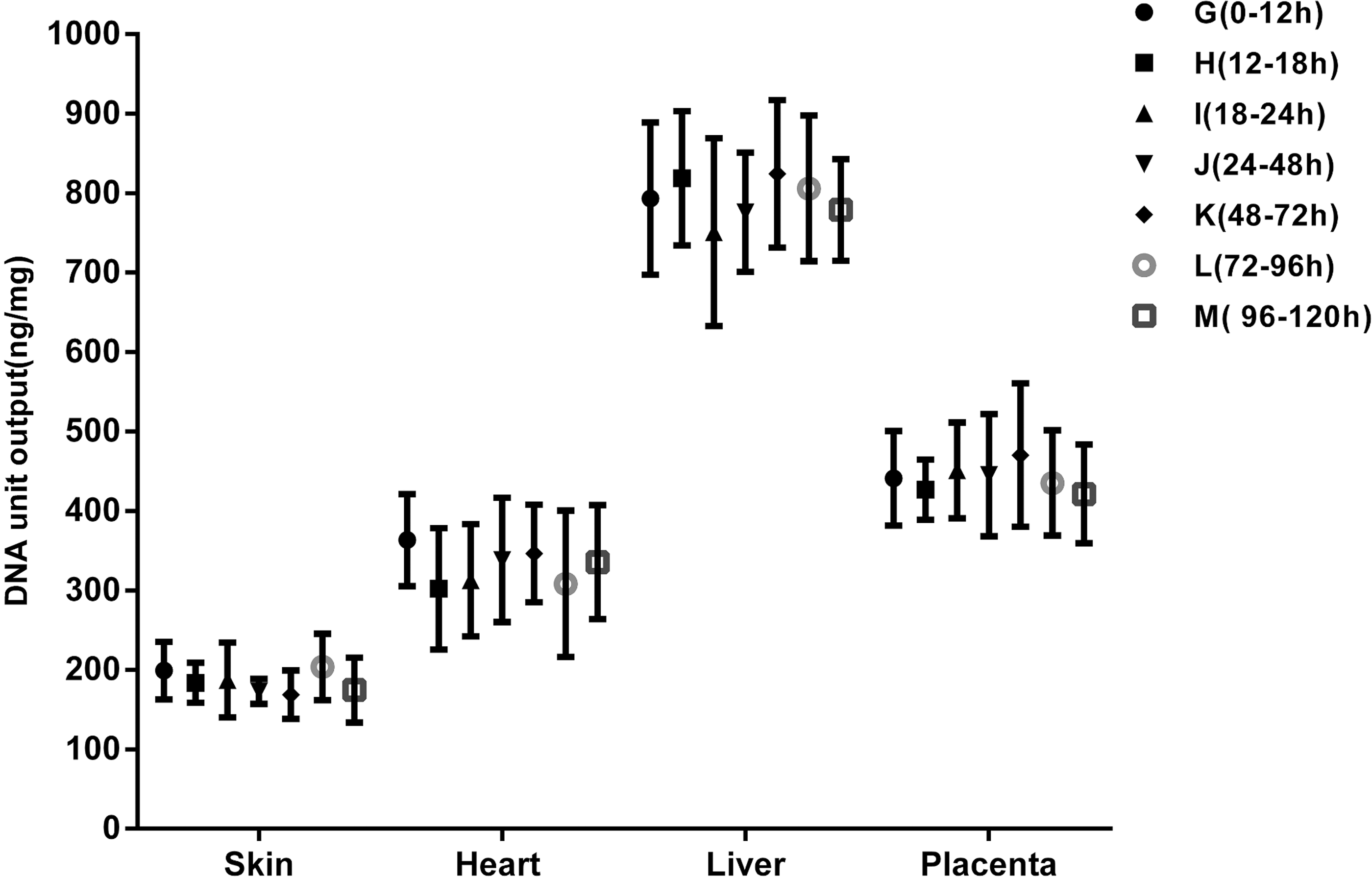
DNA unit yield of liver, skin, placenta, and heart in each CIT group. DNA unit output (ng/mg) = DNA total output of each sample (ng)/sample amount (mg). The sample size of each organ in each CIT group was 5.
DNA Unit Yield (Mean ± SD) (ng/mg) of Different Organs in Different Cold Ischemia Time Groups
DNA unit yield = DNA total yield of each sample (ng)/sample amount (mg); p1 represents p-values of DNA unit yield between different organs in the same CIT group, respectively. p2 represents p-values of DNA unit yield of one same organ between different CIT groups.
Evaluation of DNA integrity
The fragments of 1310, 600, 400, 300, 200, and 100 bp were amplified from gDNA of different CIT groups and the control group. In this article, the content (peak area) of each fragment in PCR products was detected by the Qsep100 system. The samples were classified into three ranks as follows: Qualified, Unqualified, and Poor according to the peak area ratio of each PCR fragment between sample groups and the control group (Fig. 5 and Table 4). The results showed the following. (1) The quality of the sample DNA decreased with the extension of CIT, and the skin had the best tolerance to cold ischemia, followed by the heart, liver, and placenta (Table 5). (2) The PCR products of unqualified samples showed decreases in contents of DNA fragments in all six different sizes (100, 200, 300, 400, 600, and 1310 bp). The PCR products of the poor samples showed the absence of long fragments (1310 bp) and medium-length fragments (600 bp) (Fig. 6).
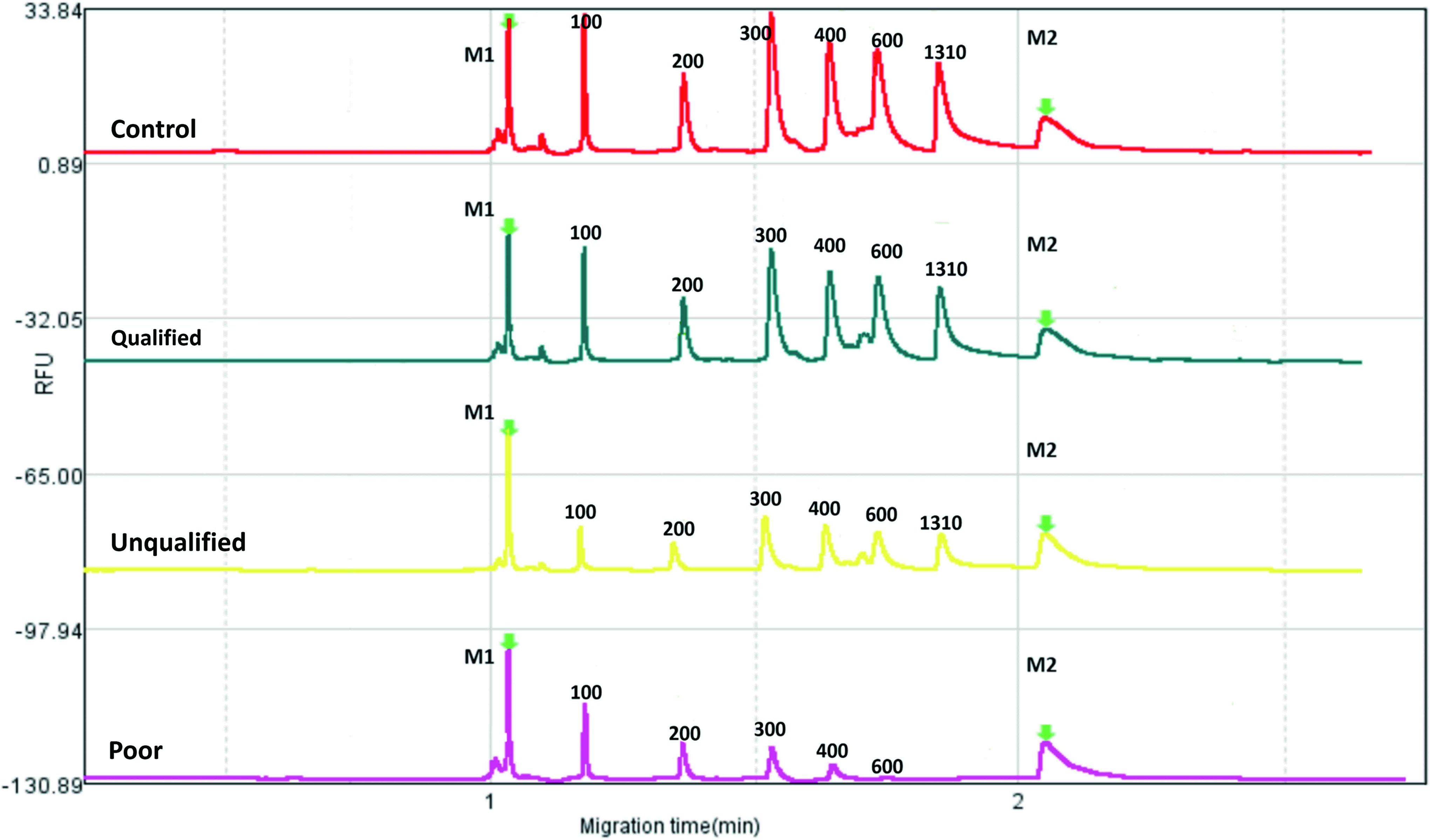
Capillary gel electrophoresis-based fragment analysis of PCR products of qualified, unqualified, and poor samples by Qsep100 system. M1 and M2 represent the lower Marker (M1 = 20 bp) and upper Marker (M2 = 5000 bp) in DNA Alignment Marker, respectively. The numbers 100, 200, 300, 400, 600, and 1310, respectively, represent the fragments of 100 bp, 200 bp, 300 bp, 400 bp, 600 bp, and 1310 bp, respectively. PCR, polymerase chain reaction. Color images are available online.
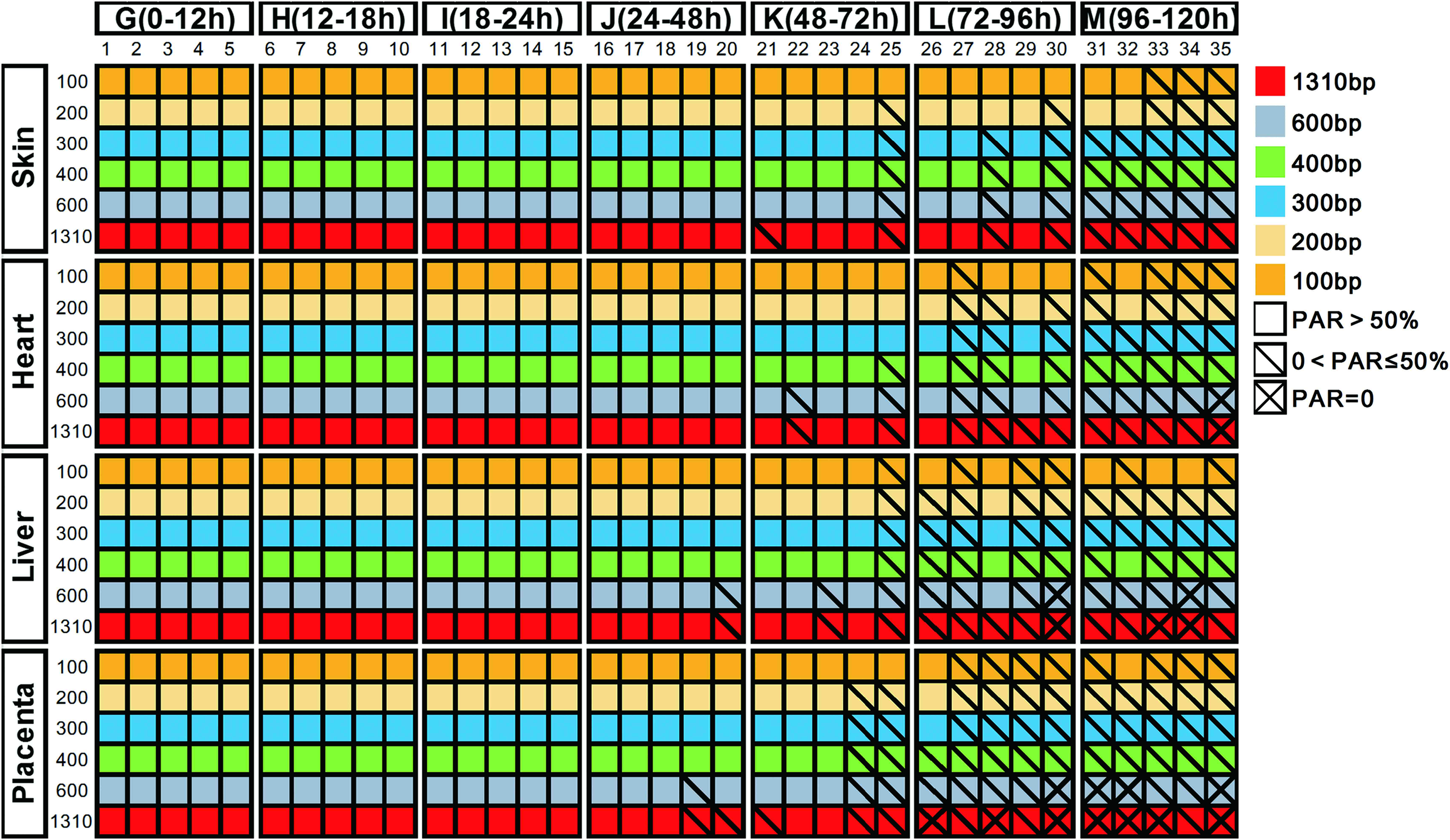
The peak area ratios of fragments in PCR products of liver, skin, placental, and heart samples. The numbers 1–35 represent 35 donors. Color images are available online.
Assessment Standards of DNA Integrity
PAR, peak area ratio.
The Qualified Ratios (Qualified Samples/Total Samples) of Different Organs in Different Cold Ischemia Time Groups
Discussion
High-risk pregnancy is considered to be a serious threat to the health and life of pregnant women and infants, which can increase the risks of complications during pregnancy, in childbirth, and in puerperium. High-risk pregnant women may have complications such as gestational hypertension, preeclampsia, and gestational diabetes, while the infants may have outcomes of premature birth, birth defects, and even stillbirth. It is of great importance to explore the pathogenesis of high-risk pregnancy as well as the prevention and treatment solutions by conducting research on high-risk pregnancy samples. However, the preanalytical variables of CIT, preservation methods, and freeze/thaw cycles may cause structural changes in nucleic acids13–16 and other bioactive substances. Therefore, we studied the placental and fetal samples, which are the common tissue samples of high-risk pregnancy, and tried to establish an effective QC strategy for nucleic acids to select suitable samples for different research purposes.
Integrity is an important index to evaluate the quality of nucleic acids, but the evaluation method needs to be improved. In this study, we used an automatic nucleic acid and protein analysis system to detect the RQN value, which is similar to the RIN value and can reflect the RNA integrity.17,18 When evaluating the DNA integrity, many studies have used agarose electrophoresis to analyze the gDNA quality.19–21 To some extent, although the quality can be observed by analyzing the smear on the electrophoresis gel, the results cannot be completely quantified and graded. In our study, the gDNA observation of qualified, unqualified, and poor samples on agarose electrophoresis showed that compared with the control sample, there was an obvious diffuse band under gDNA in poor samples, but there was no apparent diffusion difference between the qualified and some of the unqualified samples (Supplementary Fig. S1). Therefore, the qualified and unqualified samples cannot be accurately differentiated by agarose gel electrophoresis. To carry out an accurate QC, we designed six DNA primers of different sizes for gDNA amplification. The contents of DNA fragments were detected and graded for quality assessment, compared with the control group.
Several studies have focused on the impact of cold ischemia on RNA quality and the results have shown that different organs have different tolerance to cold ischemia. When the researchers investigated breast cancer tissues where the CIT was within 40 minutes (at room temperature), there was no statistical difference between the RIN values of frozen and fresh samples. 22 When stored at the temperature of 4°C, the RIN values of colon tumor samples where the CIT was within 1.5 hours decreased 44%, compared with those of which the CIT was within 10 minutes. 23 Some researchers also considered that the effect of CIT on RIN values or 28S/18S values varied from organ to organ.22,24–26 In this article, there was no statistical difference of RNA integrity between fresh placenta and CPA-free samples when the CIT was within 2 hours. If the CIT was greater than 2 hours, the RQN values of frozen samples decreased. The difference between the frozen samples and fresh tissue became more and more obvious with the extension of time. When the CIT was greater than 12 hours, the mean RQN values of CPA-free samples were less than 50% of fresh tissues. Therefore, to reduce the effect of CIT on RNA quality, it is recommended that the placenta samples should be cryopreserved within 2 hours after separation.
Moreover, we explored the protective effects of CPAs after freeze/thaw cycles of placental samples. Many researchers have considered RNAlater as a good CPA.17–19,22,23 A study on placenta and decidua showed that compared with CPA-free samples, RNAlater can stabilize RNA integrity longer and more effectively. 27 Our results showed that RQN values of RNAlater samples, which were frozen and thawed three times, were not statistically changed compared with fresh tissues. So we recommend RNAlater to be a CPA for samples that need to be frozen and thawed repeatedly. However, even with RNAlater, the samples should not be frozen and thawed more than three times. In addition, some studies have suggested that TRIzol can be used as a CPA to improve the quality and yield of RNA.28–31 However, our study found that TRIzol did not significantly weaken the effect of freeze/thaw cycles on RNA integrity. We also found that if CPA-free samples were aliquoted enough for short-term preservation without being frozen and thawed repeatedly, they can meet the requirements of most RNA research.
When comparing DNA production of different organs, it was found that, for each aliquot, if a certain DNA yield is required, the needed weight varies from organ to organ. The unit DNA yield of liver samples was significantly higher than that of placental and heart samples, and almost four times as much as skin samples. However, the current internationally recognized guidelines 13 do not provide an appropriate weight or volume of each aliquot for different organs. Our research suggested that if researchers would like to obtain adequate DNA from a single aliquot for each single trial of different kits to avoid freeze/thaw cycles or waste, preliminary experiments are recommended to determine the weight and the related volume of each aliquot before large-scale collections. A series of formal standard operating procedures (SOPs) will also be recommended. When the large-scale collection is conducted, the research should be on the basis of the SOPs.
CIT has an influence on DNA integrity of fetal samples, but the effect was different among organs. Skin had the best tolerance to cold ischemia and the following rank in turn was the heart, liver, and placenta. Consequently, if tissues had a long CIT, skin is superior to the other three organs in preservation of genetic information. In addition, we chose fresh blood (CIT <0.5 hours) as the control group for its warmth, and CIT can be controlled and minimized. The fetal samples of four different organs in various CIT groups were compared and graded based on gDNA quality. The detailed data of control and samples are shown in Supplementary Table S2. As a result, with the extension of time, the gDNA demonstrated a disappearance of the long fragment (1300 bp) first and the medium-length fragment (600 bp) second. However, the short fragments (100 and 200 bp) tended to exist in most cases. These results indicated that we could select suitable samples for experiments of different needs according to the CIT. For fetal tissues, the samples for which the CIT was within 24 hours had good gDNA integrity for most experiments. When the CIT was 24–72 hours, the content of the long fragment decreases but some of the medium-length fragments did not change greatly. These samples still can be used for routine DNA research, such as next-generation sequencing and polymerase chain reaction-short tandem repeat (PCR-STR) analysis. If the CIT was longer than 96 hours (4°C), the medium-length and long fragments were degraded and these samples can only be used for research with short DNA fragments.
Except for DNA integrity, the purity has been considered another index for quality evaluation. The A260/A280 ratios of RNA should be between 1.8 and 2.2.32–34 The A260/A280 ratios of DNA should be maintained between 1.8 and 2.0. 35 In this study, the mean values of purity in each group were not significantly different, and the purity of 98% samples was in the qualified range. The results proved our extraction process to be compliant with the standards. On the contrary, nucleic acid purity is greatly influenced by extraction methods and kits, and it is less affected by preanalytical variables. Therefore, we did not regard it as a main index for QC.
In conclusion, it is of great importance to establish an integrated and effective QC system to assure high-quality samples for a biobank of high-risk pregnancy. We developed a QC strategy for frozen tissues by analyzing the integrity and yield of nucleic acids. The strategy can instruct the collection and processing procedures and determine the most suitable cryopreservation types and conditions for different studies. However, we only focused on total RNA and gDNA of frozen tissues and did not study other bioactive substances. The samples and organs in our study were also limited. It is worth considering more extensive and in-depth studies on the influence of preanalytical variables on the nucleic acid quality of other organs. It is our plan as a next step to select more types of organs for QC studies of different nucleic acids.
Footnotes
Acknowledgments
Our research was supported by the Innovation Capability Development Project of Jiangsu Province (No.BM2015004), Nanjing Health and Family Planning Commission medical science technology innovation platform project (ZDX16006), National Natural Science Foundation Grants (81502244), social development projects supported by the Department of Science and Technology of Jiangsu province (BE2016604), Six Talents Peak projects supported by the Department of Human Resources and Social Security of Jiangsu province (WSN-080) and Fund of National Human Genetic Resources Sharing Service Platform (2005DKA21300). We thank the Department of Obstetrics and Gynecology, Nanjing Drum Tower Hospital, for collecting the high-risk pregnancy samples.
Author Disclosure Statement
No conflicting financial interests exist.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.