
Abstract
Aim:
To ensure that sample quality meets the requirements of experimental research, the gynecology and obstetrics biobank of the Nanjing Drum Tower hospital designed different quality control methods for relevant types of samples. A range of quality control procedures has been formulated.
Methods:
The sample types were frozen tissue, paraffin-embedded tissue, optimal cutting temperature (OCT)-embedded tissue, plasma, buffy coat, serum, blood clots, and urine. Different categories of samples from a random selection of 1% of cases were analyzed for quality control experiments: (i) frozen tissue, buffy coat, and blood clots: RNA and DNA were extracted and the concentration, purity, and integrity were determined; (ii) paraffin-embedded tissue: morphological observations were made after hematoxylin-eosin staining and immunohistochemical detection of β-actin or CD10; (iii) OCT-embedded tissue: hematoxylin-eosin staining and immunofluorescence detection of β-actin; and (iv) frozen tissue samples derived from different organs of 18 fetal autopsy specimens with different cold ischemia times (CITs), 0–12 hours, 12–18 hours, 18–24 hours, and 24–48 hours, were chosen to study RNA quality. There is no universally recognized quality control index for plasma, serum, and urine, so the quality of samples was evaluated from feedback from the research projects in which the samples were used.
Results:
Currently, there are ∼2000 cases and 360,000 sample vials in the biobank. According to the experiments, (i) the concentration and purity of all nucleic acids of selected samples were qualified; (ii) for frozen tissues with a CIT ≤1 hour, using a qualified standard RNA quality number (RQN) ≥7, the qualification rate was 90%; (iii) frozen tissues with CIT between 1 and 18 hours, using a qualified standard RQN ≥5, the qualification rate was 61.1%; (iv) all of the paraffin-embedded tissues qualified for morphological observation; (v) the qualification rate of OCT-embedded tissue was 89%; and (vi) CIT had a great influence on the integrity of frozen tissue RNA. As the tissue CIT lengthened, the integrity of the RNA decreased. The RNA integrity parameters of different tissue types in the same specimen were significantly different.
Conclusions:
A quality control system was constructed in an obstetrics and gynecology disease biobank with various types of diseases and abundant samples. Using specific quality control experiments for different types of samples was a reliable operating strategy that can be beneficial for providing qualified research resources. For birth defect autopsy specimens, the samples used for RNA research should have a CIT of at least <12 hours.
Introduction
T
The Nanjing Drum Tower hospital is located in Nanjing in the Jiangsu province in China, and it is affiliated with the Nanjing University School of Medicine, established by Dr. William Edward McLean, a Canadian missionary, as a “Christian hospital.” The Drum Tower Hospital has 3000 beds and more than 5600 staff. It is a first-class hospital that provides medical treatment, teaching, and scientific research.
The obstetrics and gynecology department at Drum Tower Hospital is China's national clinical key specialty and high-risk pregnancy referral center, with 380,000 annual outpatient visits from more than 20 provinces and 6000 annual deliveries, in which high-risk pregnancy accounts for nearly 70% of pregnancies. In the last 5 years, 25,451 referrals of complex cases were confirmed here. The diagnostic rate for mid-pregnancy fetal complex organ malformation was up to 70%. There was also prenatal ultrasound screening, chromosomal microarray analysis, high-throughput sequencing, cell and molecular diagnostics, and molecular genetics, which were utilized to clarify complex abnormal genotypes, karyotypes, and phenotypes.
As described above, an obstetrics and gynecology biobank was constructed. There were various specimen collection projects with diversified pretreatment methods for different types of obstetric and gynecological diseases. Due to the specifics of obstetric clinical situations, multiple potential problems should be considered before the specimen collection process. To guarantee sample quality, a well-developed quality management system was established. To ensure the sample quality meets the requirements of experimental research, the biobank designed different quality control methods for relevant types of samples, and a range of viable quality control procedures was formulated.
Materials and Methods
Design and implementation of the quality management system
The quality management system involves donor enrollment, signing informed consent, tissue sample collection, liquid sample collection, sample processing, clinical information collection, quality control management, warehouse inventory management, and so on. The implementation process of the biobank is shown as a flowchart in Figure 1. A set of standardized quality management system documents was created, including a quality manual, procedural documents, standard operating procedure files, and records and forms, and were strictly carried out during all processes at the biobank. Quality management system documents were divided into 12 categories, which are shown in Table 1.
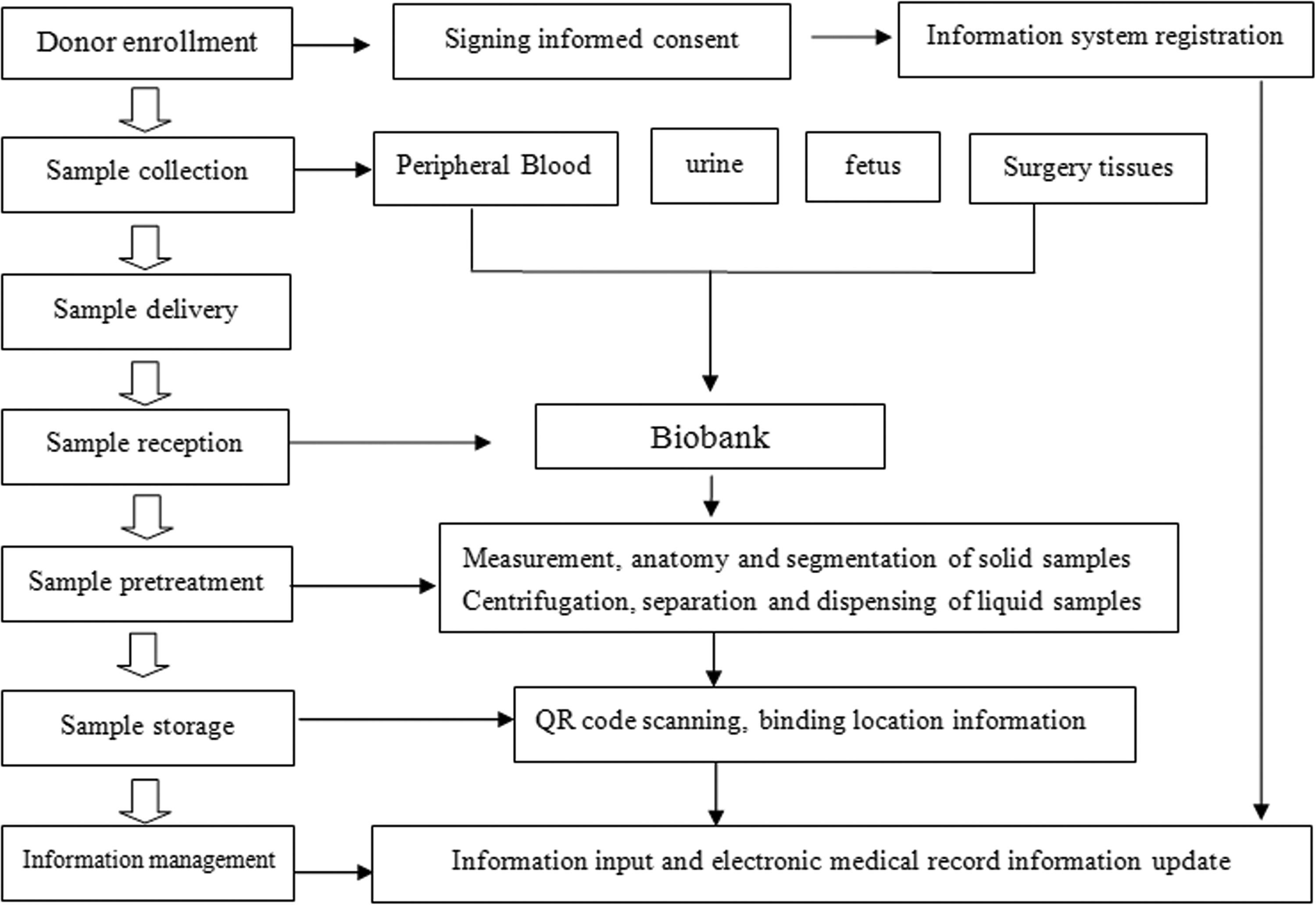
The workflow of biobank obstetrics and gynecology disease biobank.
Categories of Quality Management System Documents
Patients and biospecimens
All of the biospecimens were provided by the Nanjing multicenter biobank, namely the Jiangsu Biobank of Clinical Resources. They were collected with the cooperation of the biobank and the obstetrics and gynecology department of Nanjing Drum Tower Hospital, the Affiliated Hospital of Nanjing University Medical School, with the written consent of every donor.
Biobanking procedures
The clinical biological sample collection activity of the biobank has been approved by the medical ethics committee of Drum Tower Hospital and the human genetic resources office of the ministry of science and technology, the People's Republic of China. All of the research programs using samples were also approved by the medical ethics committee of Drum Tower Hospital. All of the biospecimens were collected with written consent provided by each donor.
The division of labor for biobanking was as follows: the gynecology and obstetrics department was in charge of designing research requirements, patient selection, informed consent, and collecting and transferring samples; the biobank was in charge of reception, disposition, storage, quality control, information management, and intake and distribution of samples. Professional biobank information management software, Infinity (RURO, Inc.), was employed to manage all of the information of the biobank, including the position of vials, information about samples, and the clinical information of donors. When inputting sample information, we also recorded the Sample PREanalytical Code (SPREC), which was suggested by the International Society for Biological and Environmental Repositories Working Group on Biospecimen Science. 1 The variables recorded for solid samples and liquid samples are shown in Table 2.
Variables Contained in Sample PREanalytical Code for Solid Samples and Liquid Samples
Collection projects and sample types
The samples in the biobank include tissues from different organs from neonatal autopsies of patients with birth defects; peripheral blood and urine of pregnant women with preeclampsia (PE); umbilical cord blood, placenta, embryonic membrane, and decidual tissues; and endometrial tissue or diseased regions of patients with intrauterine adhesions, infertility, hysterectomy, teratoma, endometrial polyps, and hydrosalpinx. Sample types were frozen tissue (with or without RNA later), paraffin-embedded tissue, optimal cutting temperature (OCT)-embedded tissue, plasma, buffy coat, serum, blood clots, and urine. The sample collection project details are described in Table 3.
Sample Collection Projects of Different Gynecologic and Obstetric Diseases
OCT, optimal cutting temperature.
Design and implementation of quality control system
There were two major categories of samples in the obstetrics and gynecology disease biobank: solid samples and liquid samples. Solid samples were mainly tissues, which were divided into frozen tissue, paraffin-embedded tissues, and OCT-embedded tissues with different pretreatment methods. Liquid samples were mainly divided into blood (including maternal blood and umbilical cord blood) and urine. With extensive scope and multiple quality control methods, the principle of our quality control experimental design was to confirm that the collection and preservation of samples could meet the corresponding research requirements.
For frozen tissue samples and buffy coats derived from blood, the extraction of DNA and RNA and the detection of abnormal expression and quantification of nucleic acid were necessary, so analyses of nucleic acid concentration, purity, integrity, and internal reference gene expression were performed. For paraffin-embedded and OCT-embedded tissue blocks, the morphological observation and detection of protein immune factors were required, so hematoxylin-eosin staining and immunohistochemical and immunofluorescence detection of internal reference genes were determined.
According to our quality control experiments, buffy coat, blood clots, paraffin-embedded tissue, OCT-embedded tissue, and frozen tissue derived from surgery had ideal qualification rates. Frozen tissue derived from autopsies had a lower qualification rate, owing to the uncontrollable cold ischemia time (CIT). For plasma, serum, and urine, the detection of various specific proteins required different analyses. In addition, since there is no universally recognized quality control index for plasma, serum, and urine, the quality of samples was evaluated using feedback from the managers of research projects in which the samples were used. Until now, all the feedback has been satisfactory.
Quality control projects
Different categories of samples from randomly selected cases were analyzed for quality control experiments and used different experimental methods according to the sample type. The quality control projects for different sample types are as follows:
Frozen tissue, buffy coat, and blood clots: RNA and DNA were extracted, and the concentration, purity, and integrity were detected. Reverse transcription analyses of RNA were then performed and β-actin mRNA expression was detected by quantitative polymerase chain reaction; Paraffin-embedded tissue: morphological observation was done after hematoxylin-eosin staining. In samples derived from surgery, immunohistochemical detection of β-actin (an extensive biomarker in most cell cytoskeleton) or CD10 (a common biomarker for endometrium) was performed; OCT-embedded tissue derived from surgery: morphological observation after hematoxylin-eosin staining, and immunofluorescence detection of β-actin.
The details of quality control experiment projects are described in Table 4.
Quality Control Experiment Projects of Different Sample Types
RT-qPCR, reverse transcription-quantitative polymerase chain reaction.
RNA quality of frozen tissue samples derived from multiple organs of fetal autopsy with different CITs
Frozen tissue samples (72 samples, 100 mg each) from four organ types (18 skin, 18 heart, 18 liver, and 18 placenta) derived from 18 fetal autopsy specimens were chosen for the RNA quality study. According to the CIT of these specimens, the samples were divided into four groups: 0–12 hours (skin, heart, liver, and placenta of four fetuses, 16 samples in this group), 12–18 hours (skin, heart, liver, and placenta of five fetuses, 20 samples in this group), 18–24 hours (skin, heart, liver, and placenta of four fetuses, 16 samples in this group), and 24–48 hours (skin, heart, liver, and placenta of five fetuses, 20 samples in this group).
Frozen tissues were first ground in an electric tissue grinding machine; the total RNA was extracted using TRIzol RNA isolation reagents (Thermo Fisher Scientific) according to the manufacturer's instructions. All of the RNA samples were tested for RNA concentration and purity (A260/280) using the ultrafine nucleic acid protein detector Nanodrop One (Thermo Fisher Scientific). Next, all of the RNA samples were diluted to concentrations of 10 ∼ 30 ng/μL, and the integrity index was detected by Qsep100 (Bioptic, Taiwan, China), which uses capillary gel electrophoresis technology for separation and detection of DNA/RNA fragments. Qsep100 can provide the RNA integrity index and RNA quality number (RQN). The arithmetic of the RQN is similar to the RNA integrity number (RIN) of Agilent2100. Parallel detection of the same samples showed that the numerical value of RQN is almost the same as the RIN. The bias was no more than ±0.1 (Table 5).
Bias Between Qsep100/RQN and Agilent2100/RIN
Bias = (RQN − RIN)/RIN, which was <±0.1.
RQN, RNA quality number; RIN, RNA integrity number.
Statistical analysis
Differences among multiple groups (comparison of multiple groups of different CIT shown in Figs. 2 and 3 and comparison of multiple groups of different sources of organs shown in Fig. 4) were determined by one-way analysis of variance. Values were considered significant when p < 0.05. Star symbols in the figures represent levels of significance, *p < 0.05 and **p < 0.01. Statistics were analyzed by SPSS 17.0, and the figures were drawn using GraphPad Prism software 5.0.
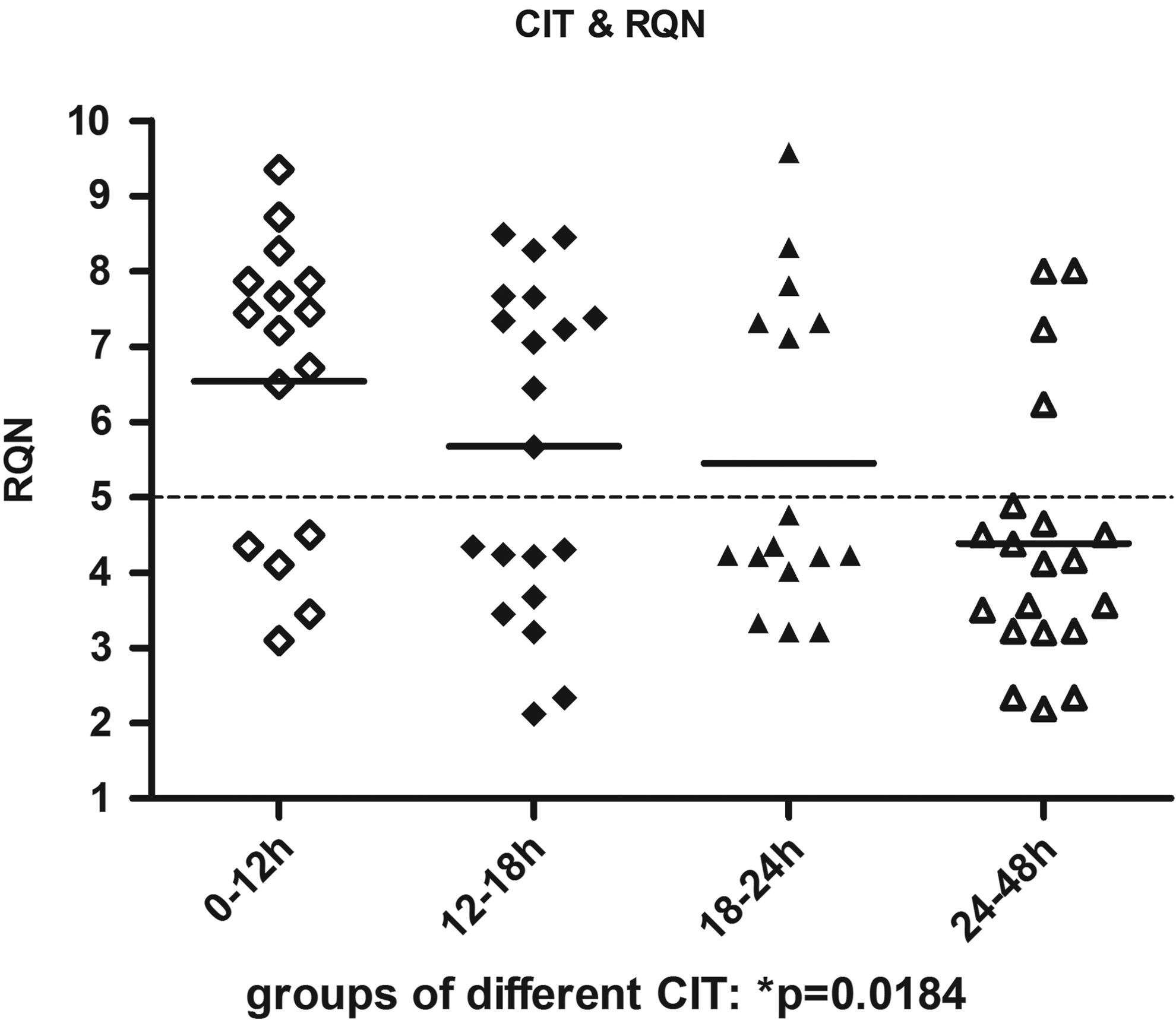
The RQNs among four sample groups (frozen tissue derived from fetal autopsy specimens) with different CITs (0–12 hours, 12–18 hours, 18–24 hours, and 24–48 hours), which were significantly different (*p < 0.05). RQN, RNA quality number; CIT, cold ischemia time.

The RQNs among four sample groups (frozen tissue derived from fetal autopsy specimens) with different CITs (0–12 hours, 12–18 hours, 18–24 hours, and 24–48 hours) in four different tissue types (skin, heart, liver, and placenta).*p < 0.05.
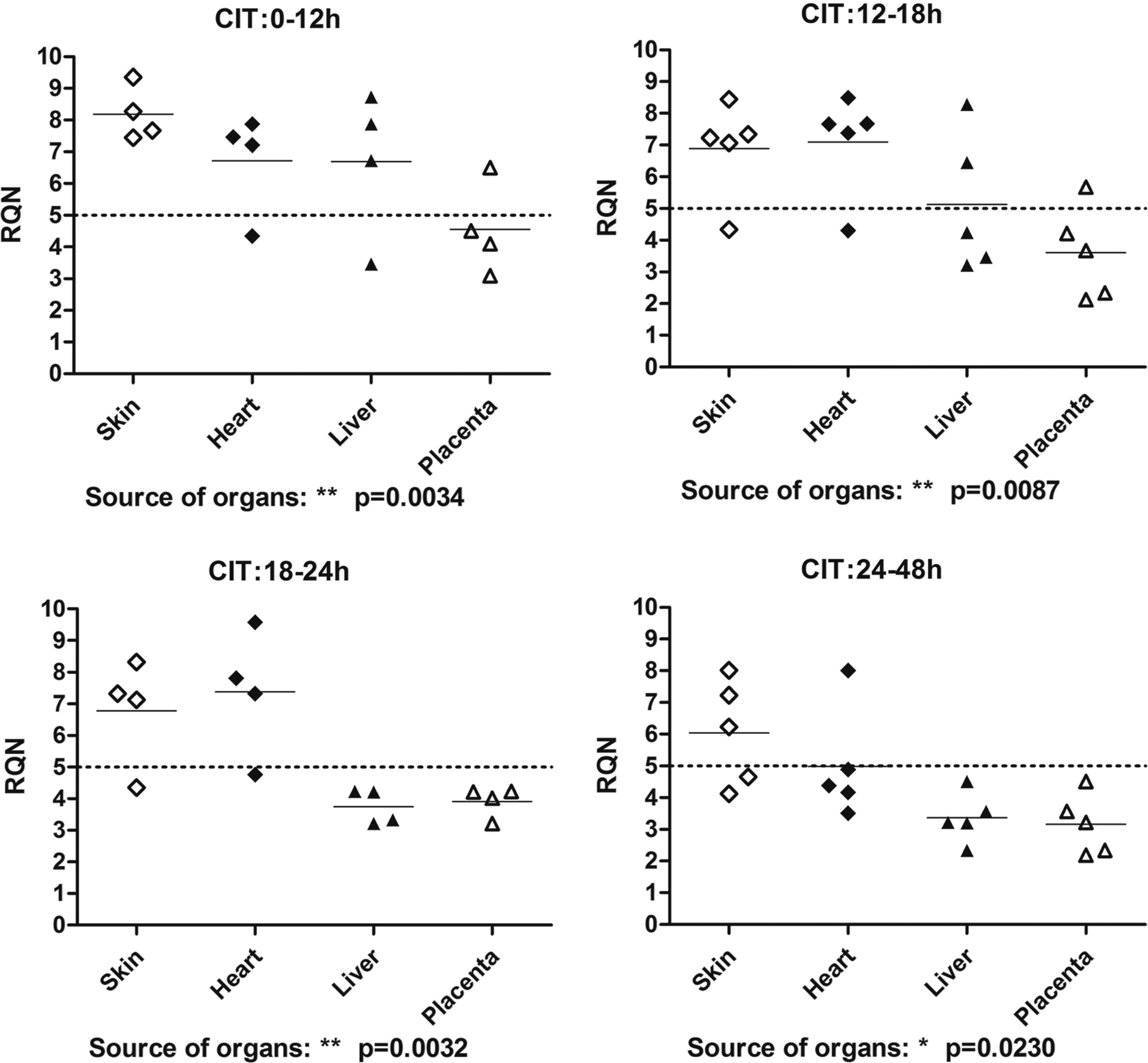
The RQNs among four sample groups (frozen tissue derived from fetal autopsy specimens) with different tissue types (skin, heart, liver, and placenta) in four different CITs (0–12 hours, 12–18 hours, 18–24 hours, and 24–48 hours). *p <0.05, **p < 0.01.
Results
Sample capacity and qualification rate of multiple sample types
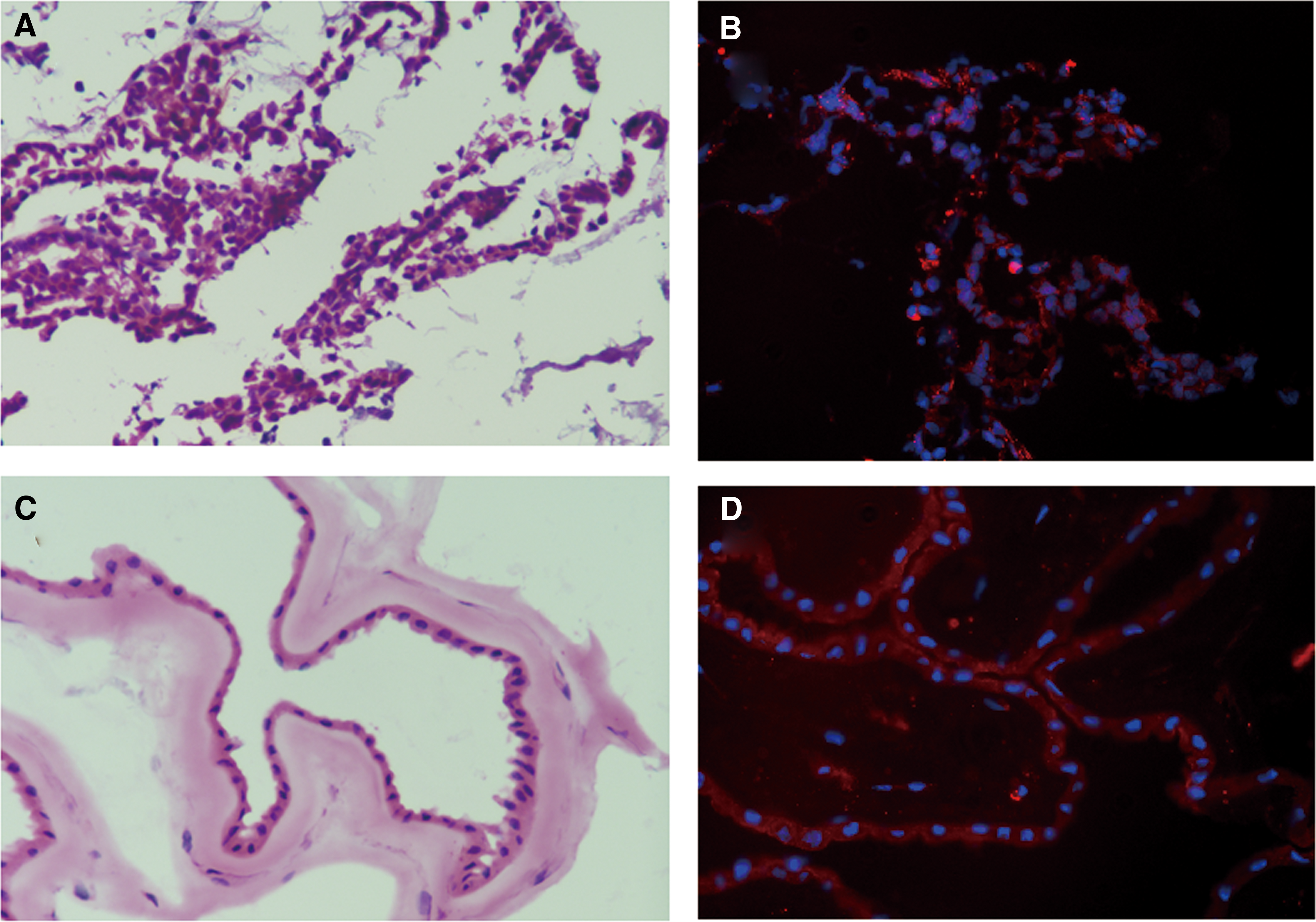
At present, in the biobank, there are samples from more than 2000 cases with obstetric and gynecological disease (1000 birth defects, 600 PE, 200 endometriosis, and 200 gynecological oncology) and up to 36,000 vials of samples, including 28,000 tissue samples and 8000 liquid samples. According to the results of the quality control experiments, (i) the concentration and purity of nucleic acids of selected samples were qualified. The purity qualification indicator for DNA was 1.8 < A260/A280 < 2.0, and the purity qualification indicator for RNA was1.8 < A260/A280 < 2.2.2–5 The concentration qualification indicator was the nucleic acid yield for each milligram of tissue ≥100 ng. The expression of β-actin detected by reverse transcription-quantitative polymerase chain reaction in the total RNA sample derived from 36 selected ovarian cancer tissues is shown in Table 6. (ii) Frozen tissues derived from surgical specimens with CIT shorter than 1 hour, using the qualification standard RQN ≥7, showed a qualification rate of 90%. An RIN of 7 is regarded as the threshold above which samples are suitable for most applications.6–8 (iii) Frozen tissues derived from autopsy with a CIT shorter than 18 h, using the qualification standard RQN ≥5, showed a qualification rate of 61.1%. Some studies report that degraded RNA from tissue samples (RIN >5) can still be used to perform gene expression analysis. 9 The CIT of samples derived from autopsy was always much longer than surgical specimens, so a concession standard (RQN ≥5) was performed. (iv) All of the paraffin-embedded tissues were qualified for morphological observation after hematoxylin-eosin staining. The staining images, whether qualified or not, were evaluated according to a tissue section evaluation standard provided by the Department of Pathology, which includes several indices such as integrity, thickness, tool marks, flat, contaminated, bubble, diaphaneity, and contrast. Figure 5 shows the hematoxylin-eosin staining images of multiple tissues and different organs derived from autopsy. Figure 6 shows the images of hematoxylin-eosin staining and immunohistochemical detection of β-actin expression in paraffin-embedded tissues derived from the maternal surface of the placenta, fetal membrane, and decidual tissue. Figure 7 shows the images of hematoxylin-eosin staining and immunohistochemical detection of CD10 expression in paraffin-embedded tissues derived from untreated endometrium, electrocuting endometrium, and the uterus mediastinum. (v) The qualification rate of OCT-embedded tissue was 67%. If tissue dehydration and bubble removal procedures were added to the sample pretreatment process, the qualification rate increased to 89%. Figure 8 shows images of hematoxylin-eosin staining and immunofluorescence detection of β-actin expression in OCT-embedded pregnant decidual tissue and amniotic membrane. For dehydration, the tissues were fixed in neutral formaldehyde for 2–4 hours, followed by two washes in phosphate-buffered saline. After washing, the samples were dehydrated in 5%, 10%, and 15% sucrose solutions for 30 minutes each. After the dehydration procedures, tissues were embedded in OCT and stored at −80°C.

Hematoxylin-eosin staining images of multiple tissues and different organs derived from autopsy. Images were photographed by microscope Nikon DS-Ri2 with magnification times 200 ×. Scalebar = 100px.

Images of hematoxylin-eosin staining

Images of hematoxylin-eosin staining
Hematoxylin-eosin staining
β-Actin Copy Number Detected by RT-qPCR of Total RNA Sample Derived from Thirty-Six Selected Ovarian Cancer and Adjacent Tissues
Different CITs influence the RNA quality of frozen tissue samples derived from multiple organs
All of the concentration and purity parameters of selected samples were qualified. The evaluation index for RNA purity and concentration was 1.8 < A260/A280 < 2.2, and the content of nucleic acid molecules extracted from each milligram of tissue was greater than 100 ng. The evaluation index for RNA integrity was RQN ≥5. The integrity results for all detected samples are shown in Figure 2. The RQNs among the four sample groups with different CITs were significantly different (p < 0.05). The longer the CIT, the lower the RQNs of the samples (Fig. 2). There were significant differences among liver tissues (p < 0.05) with different CIT, but there were no significant differences among skin, heart, and placenta (p > 0.05) (Fig. 3).
We also observed that the CIT had a great influence on the quality of frozen tissue RNA. When the CIT was >12 hours, RNA from tissues derived from the heart, liver, and placenta began to degrade. When the CIT was >18 hours, most of the RNA samples derived from the four tested organs were substandard. When the CIT was >24 hours, nearly all RNA from the heart, liver, and placenta was degraded (Fig. 4). We found that the tissue quality parameters of different tissue types in the same specimen were significantly different (p < 0.05) (Fig. 4) when the evaluation index for RNA integrity was RQN ≥5. The qualification rate of multiple tissues with different CITs is shown in Table 7. It is noteworthy that the tissue quality parameters of different tissue types in the same CIT group were significantly different and were best in skin, followed by heart, liver, and placenta.
Qualification Rate of Multiple Organ Derived Tissues with Different Cold Ischemia Time
Evaluation index for RNA integrity: RQN ≥5.
CIT, cold ischemia time.
Discussion
To maximize the utilization of resources, the construction of a biobank should be oriented to certain research projects, and the quality control system should be designed to meet research needs. The main research interests in obstetrics and gynecology at Drum Tower Hospital include birth defects, PE, and endometrial diseases. A series of articles have been published on the construction of the biobank and the associated scientific research and clinical practices.10,11 The outcomes of the research programs are dependent on high-quality clinical biospecimens. There are more uncertain and emergency situations in obstetrics and gynecology than in other disciplines, and this could disrupt biobanking procedures and affect sample quality. Reasonable planning and clinical coordination during the biobanking process are very important.
The biobank system should be able to set scoring formulas in advance on the basis of the SPREC (including the type of sample, sampling method, warm ischemia time, CIT, temporary storage temperature, centrifugal force, and storage conditions), quality comprehensive score (storage path, freezing, and thawing times, etc.) cold chain monitoring system data (the detected temperature curve and accidents), and reagent quality control data.
Quality control schemes of different categories of samples were selected based on the preassessment reference data of corresponding samples. The quality control task was generated according to multiple parameters such as sample type, range of applications, quality control cycle, and coverage. The quality control tasks included time, sample ID, quality control methods, and executive staff.
For unqualified samples in preassessment, the corresponding operations should be carried out to determine the end result assessments of the samples: (i) the samples enter directly into the destruction process and (ii) the samples derived from abundant sources can be used in a reduced scope, such as reduction to the DNA level from the RNA level. Also, reconsider the suggestion of application of unqualified samples from rare sources, otherwise the subsequent research results of these unqualified samples could not be guaranteed.
According to our biobank construction and sample quality control experiments, most of the results are satisfactory. Frozen tissues from surgery and liquid samples derived from blood and body fluids had an approved qualification rate for nucleic acid quality evaluation. The paraffin-embedded tissues were preferred for morphological observation in the biobank, which were better than frozen section staining images of fresh tissues. Without tissue dehydration, the staining images of frozen sections were not so clear compared to paraffin sections. According to the results of immunohistochemical analyses of a universal biomarker and specific biomarkers in certain paraffin tissue samples, the paraffin-embedded tissues and OCT-embedded tissues were reliable for morphological evaluation and protein expression detection.
For tissue samples, studies have reported that CIT is a critical factor for RNA integrity. It has been reported that liver samples show significant RNA degradation after 1 hour of cold ischemia, which is more pronounced in smaller samples. 12 Another study suggested that a CIT of up to 30 minutes was effective for maintaining the integrity of RNA in most samples and RNA degradation varied according to different topographies. 13 There is also evidence that sample preservation in RNA later improves RNA yield and quality, while some samples, such as breast cancer tissue, were largely unaffected by sample preservation method or cold ischemia. 14 A comprehensive study revealed that tissue quality was not adversely affected by long-term storage or limited variations of the CIT, and RNA was stable independent of tissue type with <1 hour of cold ischemia. 15
According to our results of quality control experiments, for frozen tissue samples derived from surgery, the qualification rate of RNA integrity was 90%. Meanwhile, autopsies require special attention to CIT. The delivery room is busy, and many cases with birth defects are seen each night. For most birth defect autopsy specimens, the CITs were several hours to dozens of hours. According to the results of our experiments, the CIT influences RNA integrity, and in the group of 0 hour < CIT ≤ 12 hours, the RNA of four selected patterns of organization was degraded at different levels. Most of the RNA of samples whose CIT was >24 hours was unqualified, which proved the importance of timely handling and cryopreservation of specimens. The samples used for RNA research should have a CIT <12 hours. Having extra personnel available for timely sample delivery may be helpful for shortening the CIT.
On the other hand, tissues derived from different organs have different RNA quality results. With the extension of CIT, the stability of tissue RNA was greatest in skin, followed by heart, liver and placenta. It has been reported that placenta samples collected in RNA later have higher and more consistent RINs compared to snap-frozen tissue, 16 and some studies propose a cutoff time of 90 minutes from delivery, after which samples cannot be used for gene expression analysis. 17 Results have also indicated that small differences in RNA integrity affect gene expression quantification by introducing a moderate and pervasive bias in expression level estimates that significantly affected 8.1% of studied genes. 18 We are using RNA later for the preservation of unstable tissues such as the placenta, and more specific research will be carried out in the future.
In addition to the regular quality control projects in existing facilities of the biobank, we can also randomly select various samples for qualified third-party quality control testing at regular intervals. In this way, we can obtain professional and industry-recognized quality reports for samples and have the opportunity to use more advanced methods (such as ultrathin sectioning, 19 digital pathology virtual microscopy technology, 20 and noncontact frozen sample detection,21,22) for sample quality control experiments.
Footnotes
Acknowledgments
This work was supported by the Innovation Capability Development Project of Jiangsu Province (BM2015004), Nanjing Health and Family Planning Commission medical science technology innovation platform project (ZDX16006), National Human Genetic Resources Sharing Service Platform (2005DKA21300), National Natural Science Foundation Grants (81502244), Social development projects supported by department of Science and Technology of Jiangsu province (BE2016604), and Six talents peak projects supported by department of human resources and social security of Jiangsu province, (WSN-080), China.
Author Disclosure Statement
No conflicting financial interests exist.