
Abstract
Parathyroidectomy is a standard practice to treat recurrent or persistent hyperparathyroidism. However, this can lead to the onset of hypoparathyroidism, treatable with the autotransplantation of parathyroid tissue (PT). Tissue can be transplanted immediately after parathyroidectomy or cryopreserved and transplanted only in case of necessity. Since 2011, the Cord Blood Bank and Cardiovascular Tissue Bank of Emilia-Romagna has been storing PT for potential autologous transplantation. To date, there are highly variable data about the viability and function of PT after thawing. However, it is not clear if the PT quality is affected by different cryopreservation protocols and/or by the storage time. The aim of this study was to assess the ex vivo function and viability of the PTs of ten patients stored in the Bank. Tissue morphology was evaluated before and after cryopreservation through histological investigations. PT function was analyzed by assessing the ability of cryopreserved PT to synthesize and secrete parathyroid hormone (PTH) in response to different calcium concentrations. Moreover, viability and function were also investigated on tissue-isolated cells in culture. These data show that tested tissues appear to be viable and able to produce PTH even after 5 years of storage, and the histological architecture is well preserved.
Introduction
Hyperparathyroidism (HPT) is a disorder characterized by hyperactivity of the parathyroid glands. It results in the pathological overproduction of parathyroid hormone (PTH) with related systemic effects.1,2 There are different types of HPT, depending on its etiopathogenesis.2,3 Primary hyperparathyroidism (pHPT) is due to an excessive secretion of PTH by the parathyroid glands (tumors or hyperplasia of the cells of these glands).2–6 In secondary and tertiary hyperparathyroidism (sHPT and tHPT), the PTH overproduction is a response to hypocalcemia caused by preexisting conditions such as chronic renal failure.2,6–8
The initial treatment consists of following up patients, preventing complications, or slowing down the development of the disease with appropriate medical therapies. When medical treatments fail, or in the case of symptomatic disease, a surgical approach is recommended.2,3,6,7
At present, total or subtotal parathyroidectomy is considered the standard procedure. Currently, parathyroidectomy is related to remarkable recovery rates and low morbidity, but postsurgical hypoparathyroidism is, however, a possible and feared complication. It can be responsible for serious clinical manifestations due to hypocalcemia, which can be life-threatening if ignored.2,9–11 Although the risk of hypocalcemia is low (1%) after the first operation, in the case of resurgery for recurrent or persistent HPT, this risk can increase up to 30%. 9 The permanent hypoparathyroidism harmful effects have been largely solved, thanks to the cryopreservation of parathyroid glands removed from the patient and subsequently transplanted only if necessary.11,12
Parathyroidectomy, therefore, can be followed by autologous transplantation of parathyroid tissue (PT), which consists in the implantation of small fragments of the patient's tissue, usually in the forearm.8,13 The autotransplantation can be carried out simultaneously, during the parathyroidectomy, or delayed, after a period of cryopreservation.3,8,14
The autotransplantation is the best treatment for pHPT caused by multiglandular diseases (such as sporadic, familial, or MEN 1-related primary hyperplasia) and for secondary or tertiary HPT (after total parathyroidectomy, when it appears as a severe and persistent hypoparathyroidism). 15 Cryopreservation is, therefore, an extremely useful and crucial tool for parathyroid surgery. It allows clinicians to make better decisions, evaluating over time the patient conditions and avoiding unnecessary immediate parathyroid autografts.16–18
However, from the 1970s to now, few studies have been conducted to assess viability and functional preservation of PTs after cryopreservation. Moreover, very often, these studies have yielded variable or even conflicting results due to differences in the freezing methods, in the conservation timing, and in the approaches to evaluate the function and viability of these tissues.9,11,18–26 For instance, some studies concluded that the length of the storage life is a significant factor to predict the failure or success of the autografts since a decreasing PT cell viability and functionality appear associated with cryopreservation and with an increasing storage time.9,18,21,25 Guerrero et al. showed that only 1% of parathyroid specimens stored for more than 24 months still contain viable cells, suggesting that these tissues may not be used for transplantation. 9 Other studies by Cohen et al. confirmed a dramatic reduction in cell viability and function after only 22 months of cryopreservation, demonstrating that these tissues, once transplanted, are no longer functional.18,21,22
Further studies by Alvarez-Hernandez et al. reported that most of the PTs tested after cryopreservation maintain their viability, but lose their negative feedback on calcium metabolism when compared to fresh tissues, indicating a further potential limitation in autografting after cryopreservation. 19
In this study, the viability and function of the PTs of ten patients cryopreserved at the Cord Blood Bank and Cardiovascular Tissue Bank of Emilia-Romagna were evaluated. Since 2011, in fact, the Bank has been authorized for the storage and distribution of PT from patients affected by different types of HPT, with the aim of a potential autologous transplantation in case of persistent hypoparathyroidism after surgery.
Materials and Methods
Harvesting PT samples
The Cord Blood Bank and Cardiovascular Tissue Bank of Emilia-Romagna is authorized (pursuant to Legislative Decree 191/2007 and after the agreement of the Italian National Transplant Centre, PROT. No 101/11) for the storage and distribution of PT from patients.
The study was performed in respect of the principles of the Declaration of Helsinki. More specifically, in this study, the sample tests of PT from 10 patients have been considered. Patients underwent parathyroidectomy over the last 5 years and agreed, with informed consent, to cryopreservation for an eventual transplant. In general, within 1 hour from specimen harvesting, parathyroid samples were minced, on an ice-cold tissue culture plate to avoid cell damage, in about 10 PT fragments of ∼1 mm3 and then they were distributed in cryovials with a cryopreservation medium composed of RPMI 1640 (Lonza, Walkersville, MD) supplemented with 2% human albumin (Kedrion, Lucca, Italy) and 10% DMSO (Cryo.on; Alchimia, Padova, Italy).
Cryopreservation of PT samples
The samples were cryopreserved with an automatic freezer unit programmed to reduce the temperature at a rate of about 1–2°C/min (IceCube, Sy-Lab Geräte GmbH, Neupurkersdorf, Austria) and finally maintained in the vapor phase of liquid nitrogen tanks (−145°C). In Table 1, it is possible to find all the steps of the cryopreservation protocol before transferring samples in the liquid nitrogen tanks.
Cryopreservation Protocol
For this study, tissue samples from 10 patients have been selected: 3 women and 7 men aged at the time of the surgery between 27 and 68 years old suffering from different forms of HPT (two pHPT, six sHPT, and two tHPT). The samples were thawed after different periods of storage, from a minimum of 10 to a maximum of 66 months (Table 2).
Characteristics of Patients Included in the Study
HPT, hyperparathyroidism; pHPT, primary hyperparathyroidism.
The cryopreservation and the experimental use of PT specimens were carried out in respect of safety and quality standards, according to the National Guidelines, and authorized with the patient's informed consent both for autologous transplantation and for a research investigation aimed to optimization of the current protocols.
Thawing
The tissues were thawed rapidly in a 37°C water bath. Then, at room temperature, the content of each cryovial was transferred to a test tube, and about 1 mL of washing solution (RPMI 1640; Lonza; 1% Penicillin/Streptomycin, Sigma-Aldrich, St. Louis, MO) was added drop-wise to minimize the thermal shocks. The specimens were then centrifuged for 5 minutes at 1500 rpm at room temperature. After removing the supernatant, 1–2 mL of washing solution was added, resuspending and being careful not to damage or remove the tissue fragments. This washing procedure was repeated 3–5 times to be sure to remove the cryoprotectant solution. Finally, the PT samples obtained were placed on a Petri dish for the selection of the fragments for function, viability, histological, and isolation tests.
Functional analysis
For each sample, 4 fragments were distributed in 2 wells of a 24-well plate, 2 pieces for each well, with 500 μL of medium. PT was incubated with two different media. The first medium M1 was composed of RPMI 1640 with
Viability test
For each thawed sample, two fragments of PT were placed in a single well of a 24-well plate with 500 μL of culture medium RPMI added with 10% Fetal Bovine Serum (FBS) (Lonza) and 1% Penicillin/Streptomycin antibiotics (Sigma-Aldrich). The samples were maintained at 37°C for 3 days in sterile conditions. At three different time points, T-0, T-24, and T-48 hours, 10% of alamarBlue reagent (alamarBlue® Cell Viability Assay; Thermo Fisher Scientific, Waltham, MA) was added to the culture medium and incubated for 19 hours. After the incubation, the medium was collected and placed in triplicate in a 96-well plate, 100 μL for each well, for measurements. The fluorescence signals were measured with a spectrofluorometer (Victor Multilabel Plate Reader; Perkin Elmer, Boston, MA) applying a fluorescence excitation wavelength of 530–560 nm and reading the fluorescence emission at 590 nm. Tissue fragments, devitalized, were used as negative controls (NCs). They were obtained by keeping them in deionized H2O for 24 hours to make them no longer viable. Finally, the percentage of alamarBlue reduction was normalized to the basal medium (F590 sample × 100/F590 basal medium).
Histological analysis
A tissue fragment of each specimen was fixed with 10% buffered formalin solution and embedded in paraffin. The tissue sections (2 μm thick) were stained with hematoxylin and eosin (H&E) for the assessment of the overall tissue architecture and morphological characterization.
If precryopreservation morphological data were available, a comparison analysis between fresh and thawed tissues was performed.
Cell isolation procedure
Two isolation protocols were used to isolate different cell types. For the first protocol, tissue fragments were placed into six-well plates and cultured with growth medium RPMI supplemented with 10% heat-inactivated FBS, 2 mM
For the second protocol, tissue fragments were digested for 40 minutes with collagenase II (1 mg/mL; Sigma-Aldrich) at 37°C. The enzymatic activity was then inhibited with FBS, and the suspension flowed through a 100 μm strainer. The flow-through cell suspension was centrifuged for 5 minutes at 1500 rpm, and the cell pellet resuspended. Cells were finally counted with erythrosine B (Sigma-Aldrich Co., St. Louis, MO) and cultured at a density of 50,000 cells/cm2 in standard growth medium.
Results
Precryopreservation and postcryopreservation histological analysis
H&E staining was performed on formalin-fixed and paraffin-embedded samples to evaluate the tissue morphology after different periods of cryopreservation.
The majority of the thawed PT fragments proved to be free of significant cytological and histological alterations, regardless of the months of cryopreservation. Only one sample (S4) was characterized by alterations related to cryopreservation with nuclear shrinkage and focal disappearance of cytoplasm (data not shown).
In 7 out of 10 samples, an evaluation was also performed of the freezing process effects, comparing tissue fragments from the same glands before cryopreservation and after thawing. Overall, this comparison showed no significant morphological differences between the specimens (Fig. 1). After thawing, chief cells, those responsible for PTH secretion, did not show nuclear and cytoplasm shrinkage; nuclei were round and homogeneously stained with hematoxylin; depending on the functional activity, the cytoplasm was eosinophilic or clear; after 52 months of cryopreservation, the thawed corresponding sample focally showed cytoplasm fraying.
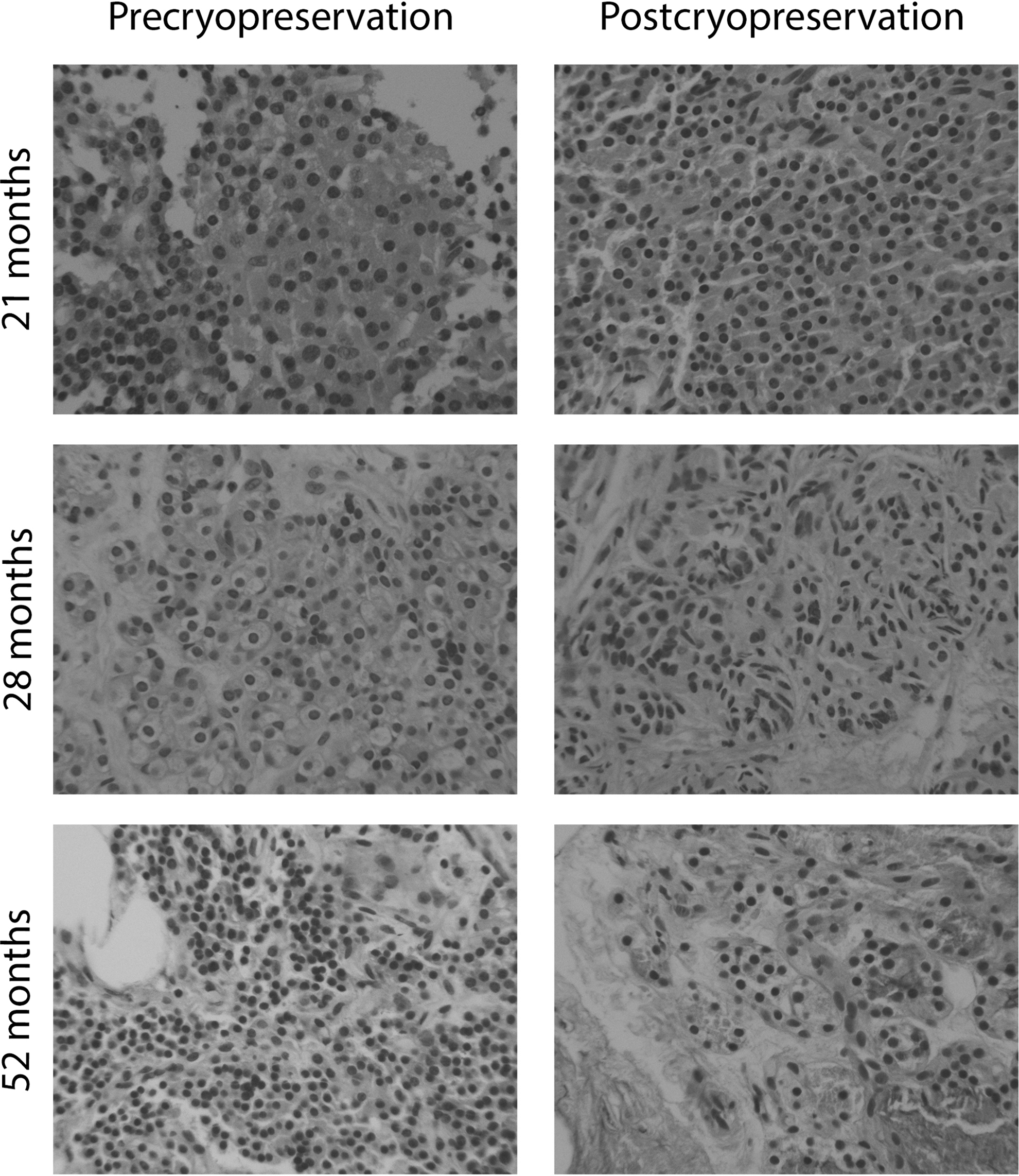
Precryopreservation and postcryopreservation histological analysis. Evaluation of the effects of freezing processes on tissue architecture. The PT of the samples S8 (21 months), S6 (28 months), and S2 (52 months) before freezing and after thawing shows comparable morphological characteristics. H&E staining. 10 × magnification. PT, parathyroid tissue; H&E, hematoxylin and eosin.
Cryopreserved parathyroid fragment viability (alamarBlue assay)
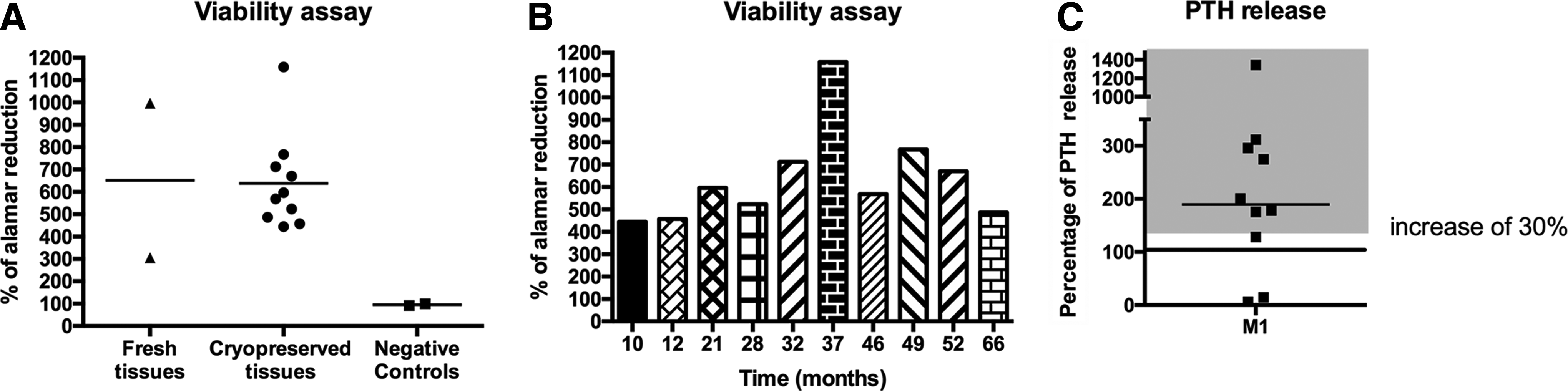
In vitro biological tests were performed to qualitatively and quantitatively determine the viability of parathyroid fragments after cryopreservation. The alamarBlue assay at different time points was analyzed (data not shown) and results at 48 hours in culture were reported in Figure 2A, B. All samples, regardless of period of cryopreservation, showed a percentage increase of the alamarBlue reduction compared to not viable samples (NC with a mean of 95.9%) with a mean of 638.6% ± 217.7% and a range of 444.2%–1158.4%. No correlation was observed between the years of cryopreservation and the percentage of alamarBlue reduction.
Viability and PHT release.
Functional analysis (PTH release in cryopreserved PTs)
PT fragments cryopreserved for different periods of time were tested for the capability to modulate the PTH secretion in response to different calcium concentrations. After thawing, samples were incubated with two different calcium concentrations M1 (0.6 mM Ca2+) and M2 (1.2 mM Ca2+) for 48 hours, and the PTH concentration was determined. As shown in Figure 2C and Table 3, 8 out of 10 cryopreserved parathyroid fragments cultured in 0.6 mM calcium showed a meaningful and relevant higher PTH secretion (30%) compared to the same gland fragments maintained in 1.2 mM calcium (reference: 100%), with a mean of 363.7% ± 401.7% (range 128.1%–1344.8%). Among these, two samples (S3 and S4, 20%) showed a loss of their negative feedback control system with an abundant release of PTH even in the presence of high calcium concentration (1.2 mM, M2 medium).
Parathyroid Hormone Concentration (pg/mL) at Lower and Higher Ca2+ Values and Viability
PTH, parathyroid hormone.
Cell isolation
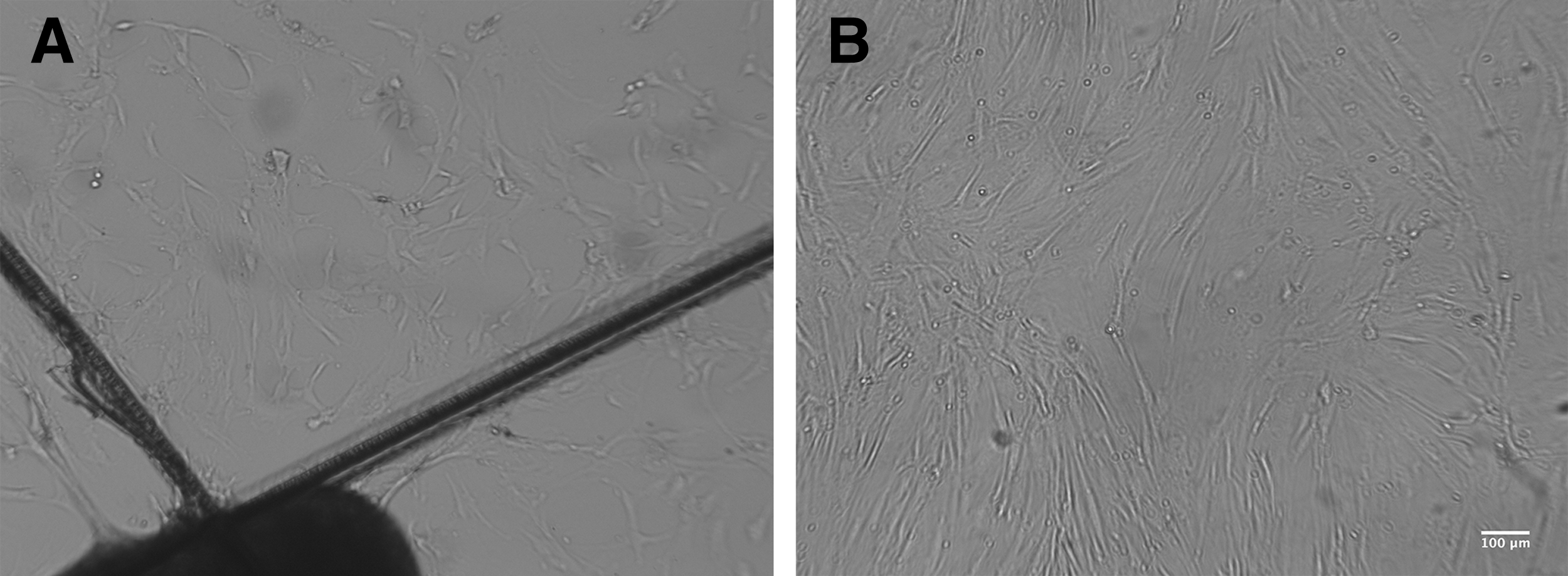
To thoroughly analyze the quality of cryopreserved tissues, two cell isolation techniques were investigated. The first approach focused on the isolation of stromal cells, while the second on the chief cells, the endocrine component. In the first case, a small fragment of cryopreserved PT was plated in culture. After 1 week, cells moved from the tissue and started to grow on the plastic (Fig. 3A). Cells showed the classical fibroblastic morphology and reached confluence in about 2 weeks (Fig. 3B). Moreover, cells were expanded and cryopreserved again.
Stromal cell isolation from cryopreserved parathyroid.
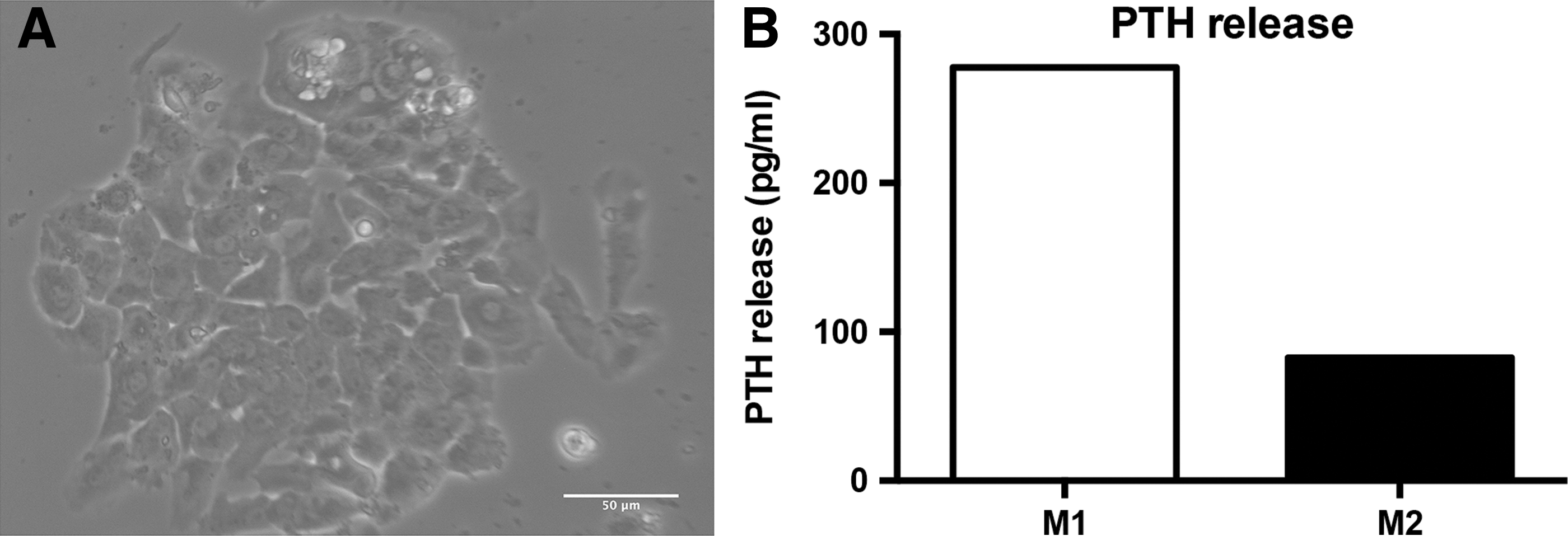
To isolate chief cells, tissue fragments were digested with collagenase II (second technique), and the cell pellet was plated in culture. After a few days, cells with a classical cobblestone morphology were observed (Fig. 4A).
Endocrine cell isolation from cryopreserved parathyroid.
To determine the ability of endocrine cells (chief cells) to release PTH in response to calcium concentration, cells derived from one sample were also incubated for 2 hours with M1 and M2 media. After the incubation period, the medium was collected, and PTH release was determined. As shown in Figure 4B, PTH concentration is increased in M1 condition (277.7 pg/mL) compared to M2 condition (82.7 pg/mL).
Discussion
The damaging effects of permanent hypoparathyroidism have been largely solved, thanks to cryopreservation, and follow-up autotransplantation of parathyroid glands previously removed from the patient.
However, indications and protocols for cryopreservation and grafting developed over the years are quite different among various institutions. This leads to highly variable results with published data that report autograft success rates between 17% and 83%.8,16,23,24 Moreover, few studies have been conducted to assess the viability and function of PT after cryopreservation, and very often these studies report conflicting results.9,11,18–26 Despite this, literature reports highlight that the length of cryopreservation may be a significant factor to predict the failure or success of the transplant because the storage period reduces the viability of PTs and their responsiveness to different calcium concentration.12,19
In this study, all thawed tissues tested have proven to be viable and PTH-secreting, regardless of the length of cryopreservation (from 10 to 66 months), without identifying any trend linked to longer storage times.
Moreover, 80% of the tested tissues, once thawed, have proven not only to be able to produce PTH but also to properly respond to calcium concentration changes. Only in two cases (20% of all the cases), a complete loss of the negative feedback involved in the control of PTH secretion at increasing calcium concentration has been observed. However, it is important not to underestimate the possibility that such an alteration could not be provoked by the cryopreservation process, but it could also be a consequence of the patient disease that affects the glands' physiological functions. 2
It could also be assumed that the glands may show a reduced response capacity to changes in calcium levels due to the stress suffered by the cells during thawing and reimplantation processes. It is very fascinating that results observed in clinical practice after the reimplantation of fragments of PT suggest that the calcium response may improve after a period of temporary adaptation. 19
Moreover, the histological analysis before and after freezing did not show any relevant cytological difference or significant morphological alterations in the tissue architecture, confirming the results obtained with the viability and functional analysis.
Another aspect observed in this study is a significant variability among samples. Such differences are most likely due to an intrinsic biological variability, but may also be caused by the difficulty of the preparation of standard samples with equal dimensions, weight, and cellularity. It underlines, therefore, the need for improvement in the standardization of experimental processes.
Most of viability studies in the literature are focused on cultured cells in monolayer, and there are very few studies on biopsy specimens or tissue fragments. Another interesting point is that the protocol performed in this study showed the effectiveness of alamarBlue in the viability assessment of the cells contained in the tissue fragments examined.
With respect to the extreme variability of freezing protocols described in literature by various institutions, considering the results obtained in our processing laboratory in more than 10-year experience, we can conclude that the choice to carry out a programmed cryopreservation and the freezing solution certainly influences tissue viability. To preserve specimen integrity and functionality, we have determined that in the cryopreservation process, it is important to combine in the freezing solution a part of human proteins as additional cryoprotective agents (albumin or autologous serum in our experience). Moreover, for preserving PT, RPMI is certainly the optimal medium as it contains low levels of calcium. Finally, the rapid time of thawing and the immediate DMSO removal are also very critical.
The isolation of viable cells from fresh and cryopreserved PT has been described in several studies20,27,28; however, data from cryopreservation periods longer than 24–25 months are not available.9,26
To thoroughly analyze the effect of cryopreservation on the different types of cells present in the PT, both the stromal component and the endocrine component have been successfully isolated. We have also tested the capability of endocrine cells isolated after cryopreservation to secrete PHT in response to different calcium concentration. These results showed that cell functionality is maintained also after cryopreservation.
In conclusion, PT cryopreservation after parathyroidectomy is currently a very common practice, although the actual use of cryopreserved tissues is low, and autografts are few.
Considering that it can take years to distinguish a transient hypoparathyroidism condition from a permanent one, an optimal and efficient cryopreservation, able to ensure quality products with proper viability and function even after long periods of storage, would be a significant therapeutic advantage for these patients.
The findings of this study then support the possibility to store the PT for a more extended period than suggested by the literature to date, assuming a period of 5 years as maximum storage time, as defined for the cardiovascular tissues cryopreserved at the bank according to national and international guidelines. Finally, these data provide an interesting starting point for further investigation, but still need a higher level of statistical validity (i.e., by increasing the sample number) and a better sample standardization to confirm and deepen what has been observed so far. All of this may, indeed, provide new insights for more efficient validation tests, enhancing the sample preparation phases and obtaining the best quality products.
Footnotes
Author Disclosure Statement
No conflicting financial interests exist.