
Abstract
Standardization and sustainability are ideals within the biobanking world, and the demand for high-quality well-annotated specimens is growing just as rapidly as the ever-increasing precision and throughput of today's high-tech scientific methods. In the state of New South Wales (NSW) in Australia, the state government has allocated significant funding toward this requirement in recent years, with the launch of the NSW Health Statewide Biobank in central Sydney in 2017, and the introduction of the voluntary NSW Biobank Certification Program, and Consent Toolkit. For new and established biobanks, the influence of these new resources has been twofold: first they have provided valuable guidance for moving toward standardized practices and raising the bar for biobanking quality standards; second, they have brought to the forefront the challenges of sustainability and transitioning to a certification standard of biobanking. In Westmead, ∼20 km from Sydney's central business district, the Westmead Research Hub has responded to these challenges with a collaborative biobanking project initiated in 2015. As the site of almost 30 individual biobanks, and to inform a pilot project of central biobank services, a questionnaire was developed and administered to all of the biobanks. This article reports on the results from the questionnaire and the rationale for subsequent initiation of a core biobanking facility.
Introduction
The Westmead Research Hub (WRH) 1 is located in Westmead, Western Sydney, in a precinct that combines the resources of two world-leading research institutes, two of the largest hospitals in the southern hemisphere plus a major private hospital, the largest pathology laboratory in New South Wales (NSW), and internationally renowned universities, to tackle many of the most common diseases affecting our community. Established in 2001, the WRH partners have been successfully collaborating for 18 years, and WRH is now home to 1400+ researchers and students.
With the colocation of medical research, education, and clinical practice at Westmead there is huge potential for collaboration on translational research projects. This is strengthened by a group of close to 30 biobanks, including biobanks with national and international scale and recognition, which represent an essential part of the research resources on campus. With a major goal to undertake projects that encourage collaboration and sharing both physical and intellectual resources of its members, the WRH has adopted biobanking as a priority area for development.
To initiate this development, a number of WRH biobanks agreed to work together toward a synergistic operating model that would consolidate common biobanking functions. As the first stage of the project, a questionnaire study was designed and conducted to define the current status of WRH biobanks, and to establish the basis for a common operating model. The second stage was to be a pilot project, which is currently underway, to develop and launch central services that will enable and encourage biobanks to move toward a synergistic operating model. Plans for the third stage will be an expansion of access to core facilities developed during the pilot project.
Methods
The WRH appointed a Project Officer 2 days/week from February to December 2017 to develop and conduct a questionnaire of all biobanks operating in the precinct. The project had three objectives:
To obtain current information from all WRH biobanks through the development and administration of a questionnaire. To determine the optimal ways in which WRH biobank operations could be facilitated though synergies, economies-of-scale, and common functions. To disseminate the project findings to both the stakeholders and the WRH as the basis for future planning.
The project first required identification of the complete list of biobanks at WRH; since biobanks had been established individually across multiple different institutes and hospitals, there was previously no such record. With the aim to gather information to inform central support for biobanks on campus, all organized collections of biospecimens and/or data that are routinely collected and stored for the purpose of future research were of interest. Hence all such collections, both human and other organisms, were eligible to participate and no further definition of “biobank” was used for the purpose of this study. Only collections for clinical trials or otherwise primarily for diagnostic purposes were excluded.
The communication designed to elicit a complete list of biobanks was iterative. Initial contact was made with heads of departments and clinical units, directors of the WRH medical research institutes, and senior research leaders in the WRH, requesting information on biobanks of which they had knowledge. Initial contacts were asked to cascade the information to relevant individuals and departments within their organizations. Leads identified subsequent to that initial contact were then pursued, until the full complement of WRH biobanks was identified.
Thirty-three biobanks were identified by this process, which we believe was comprehensive in its reach. Twenty-eight of the biobanks identified participated in the questionnaire, all of which were currently in operation. The small percentage of biobanks that did not participate did not do so for a number of reasons, including that they were new and had not yet started collecting, or were historical collections no longer operating.
A questionnaire was developed addressing all areas of biobanking activity with questions tailored to discover the main activities of WRH biobanks and where they placed in a biobank life-cycle (Supplementary Data). Development of the questionnaire aimed for a broad picture of the biobanking activity on campus within a limited timeframe for the study, and so prioritized inclusion of questions to discover how biobanks would benefit from central facilities rather than gaining depth of detail in any one area. To encourage maximal participation, it was also important to design the questions to enable participation without too much time commitment from the biobanks.
The resulting questionnaire had 41 questions, grouped into seven categories:
General details
Consent and donor recruitment
Collection and access
Data and standard operating procedures
Finance
Risk management and sample integrity
Other biobanking-related activities
After administering the questionnaire, the Project Officer corresponded with participants via follow-up phone calls, face-to-face meetings, and e-mails to clarify answers and obtain additional information for analysis. The final information was stored in a purpose-built Access database.
Results
Geographical distribution
The 28 participating biobanks were associated with all five of the WRH partner organizations 2 : Western Sydney Local Health District; Institute for Clinical Pathology and Medical Research (trading as NSW Health Pathology [ICPMR]); The Westmead Institute for Medical Research; The Sydney Children's Hospitals Network (Kids Research); Children's Medical Research Institute; and The University of Sydney.
Illustrative of the translational research projects based at Westmead, WRH biobank operations cross over from hospitals to research institutes, both in terms of sample storage locations and Principal Investigator affiliations. Storage of samples is spread widely across the WRH campus, but with a concentration at research institutes (19 biobanks; 68%). Principal Investigator affiliation is more evenly distributed between clinical and research environments, with 54% of Principal Investigators (15 biobanks) having their main affiliation with public health organizations.
Donor recruitment locations and sample collection points revealed a large geographical distribution, with 10 biobanks recruiting patients from state-wide hospitals, and 4 biobanks nation-wide. Most donors are recruited from the public hospital system, but donors are also recruited at private hospitals and clinics. Similarly, while the majority of sample collection occurs within the Westmead precinct, a significant number of the biobanks also collect samples from further afield.
Type of collections
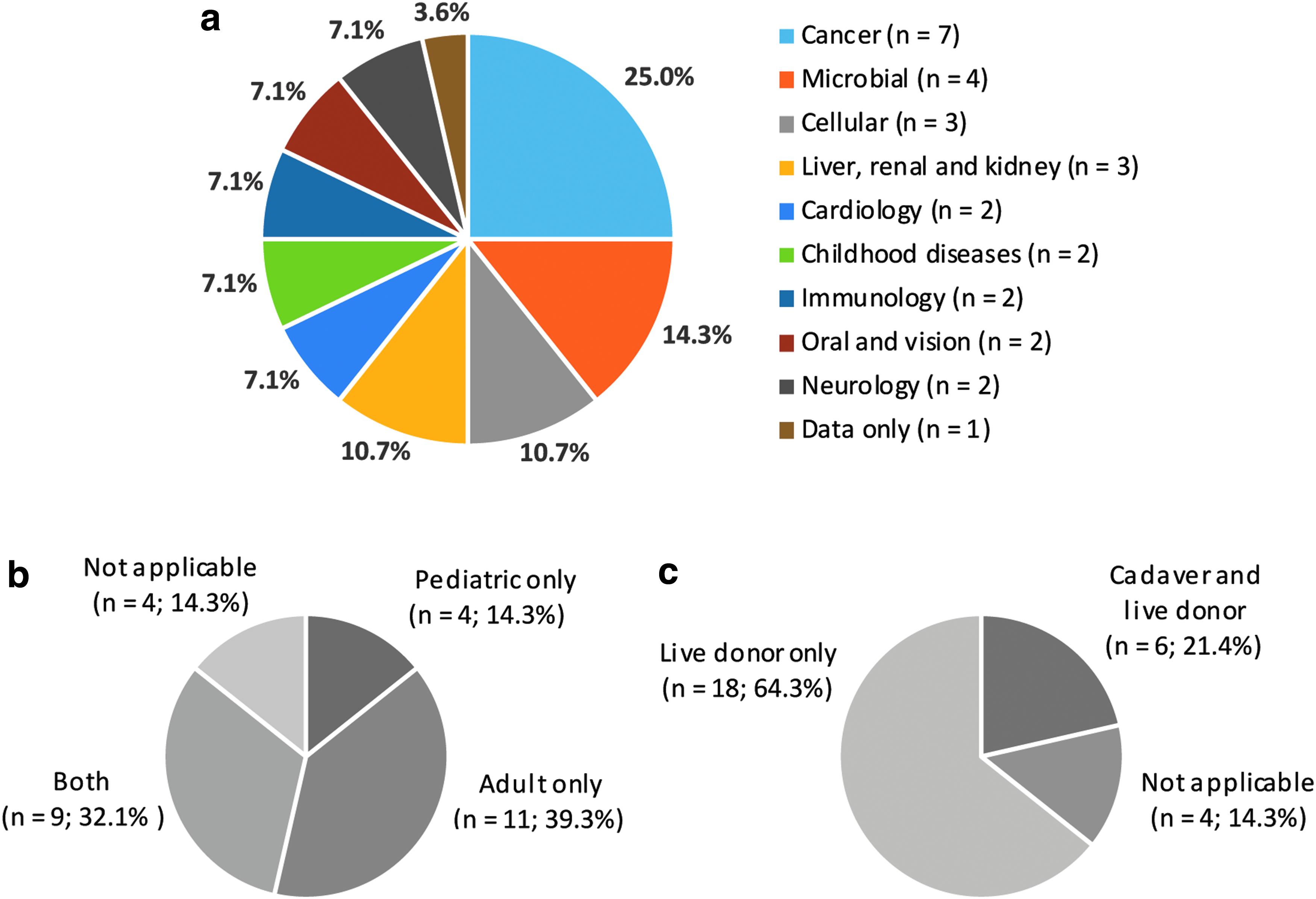
The biospecimens and data held in the 28 biobanks are all disease-based collections including a diversity of human samples, as well as other organisms. The predominant collection types are cancer samples (7 biobanks; 25%) and microbial collections (4 biobanks; 14%). The next most common are cellular (3 biobanks; 11%) and liver, renal, and kidney (3 biobanks; 11%) (Fig. 1a).
Types of biospecimen and data collections held in WRH biobanks:
Since WRH partners include the Children's Hospital, Kids Research, and the Children's Medical Research Institute, significant recruitment of pediatric patients was to be expected: 10 biobanks (36%) collect from both adult and pediatric donors, 11 biobanks (39%) from adult patients only, and 4 biobanks (14%) from pediatric patients only (Fig. 1b). Most biobanks collect from live donors only (18 biobanks; 64%), and 6 biobanks (22%) collect from both live donors and cadavers (Fig. 1c).
Stratification by primary and secondary sample types revealed a diverse collection across the biobanks. Tissue samples (fresh/frozen or fixed) and blood and derivatives were the most common primary sample types, together making up more than half of the primary samples (65%). Other primary sample types collected include bodily fluids and aspirates, buccal swabs, urine, stool, and microbes (Fig. 2a). Most biobanks (18 biobanks; 64%) also collect and store control samples, which had a similar distribution; most control samples were tissue or blood and derivatives, with the remainder comprised of a variety of other sample types.
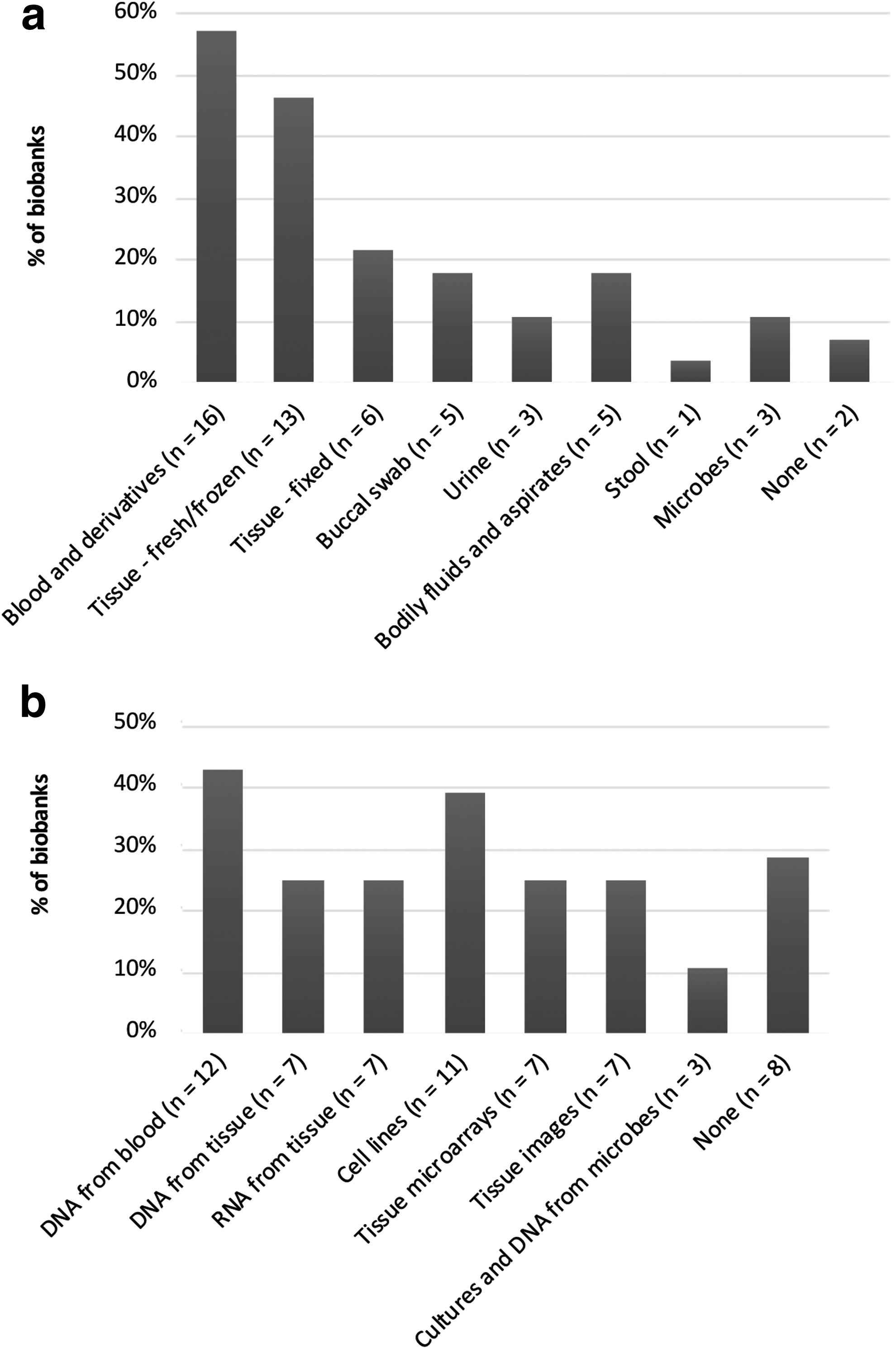
A number of different secondary sample types are stored by the biobanks, with DNA from blood being the most common type (12 biobanks, 43%), followed by cell lines (11 biobanks, 39%). DNA from tissue; RNA from tissue; tissue microarrays; tissue images; and cultures and DNA from microbes are also stored by the biobanks (Fig. 2b).
Data
Almost all of the biobanks (26 biobanks; 93%) store sample tracking and clinical data in databases, ranging from Microsoft Excel spreadsheets to relational databases in Microsoft Access, open-source software, custom-built project-specific applications, and proprietary Laboratory Information Management Systems. The most common applications used are Excel (11 biobanks; 36%) and Filemaker Pro (6 biobanks; 20%).
The types of clinical data collected are extensive. The most common data item collected is demographics (20 biobanks; 71%), and at least half the biobanks also collect pathology, family history, medications, and comorbidities. Collection of lifestyle factors, treatment, and follow-up data is less common.
Participant consent
A considerable variety of personnel is involved in obtaining informed consent from biobank donors, and some biobanks use more than one type of personnel to obtain consent. Clinicians are involved in obtaining consent for more than half of the biobanks (16 biobanks; 57%), and Clinical Nurses (11 biobanks; 39%), and Biobank Officers (8 biobanks; 29%) are the next most common. Research personnel, other clinical staff, and Genetic Counsellors are also involved in obtaining consent (Fig. 3).
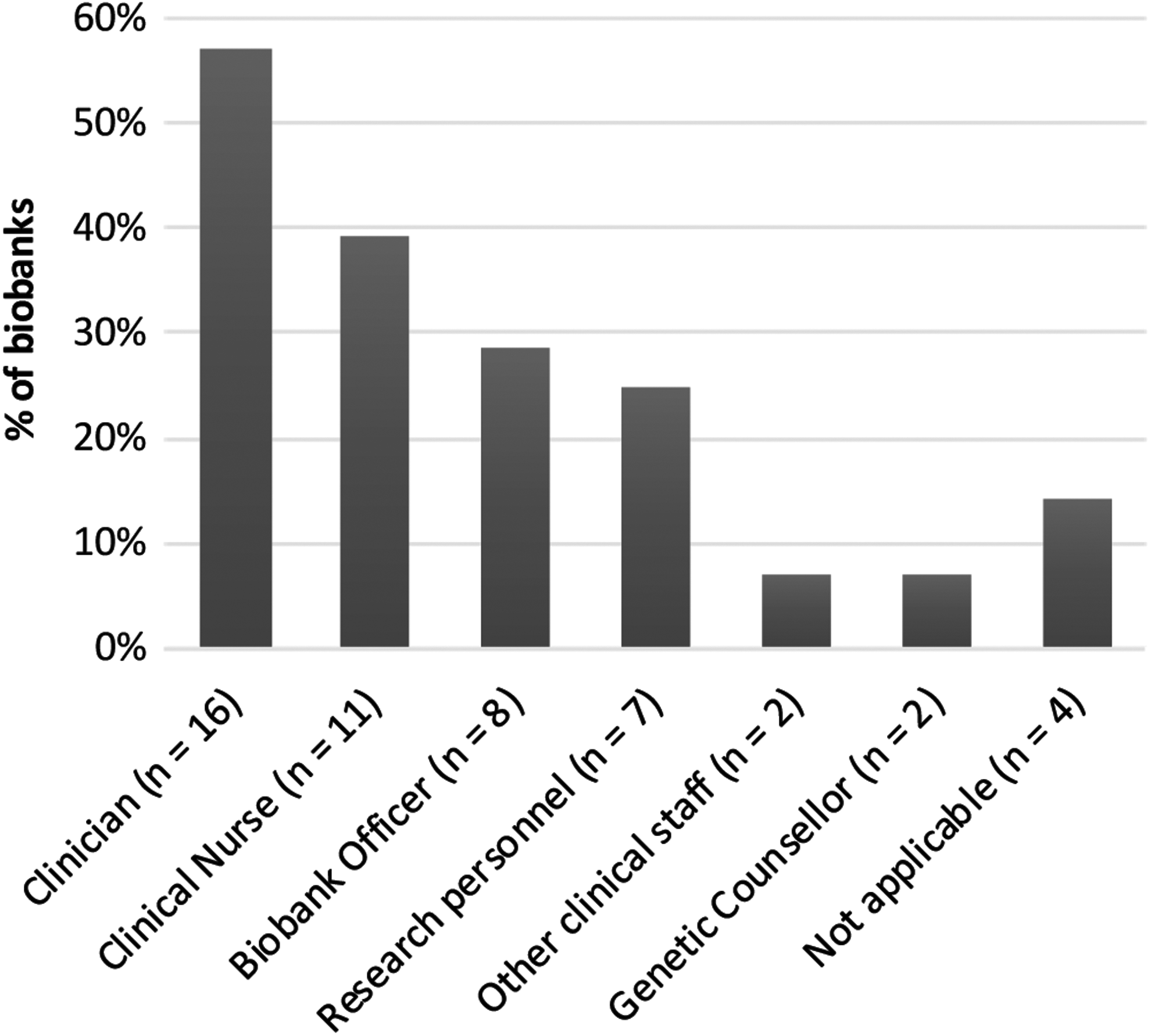
Personnel involved in obtaining informed consent from WRH biobank donors. This question was not applicable to biobanks where consent is not required (bacterial and fungal collections) and where consent is not obtained by the biobank directly (cell culture collections previously consented and deposited into the biobank via an agreement).
The majority of the biobanks (26 biobanks; 93%) have donor consent, and of these biobanks, most (19 biobanks; 73%) have consent for unspecified future research. For fungal and bacterial collections (2 biobanks; 7%), consent is not applicable.
Access policies
About half of the biobanks (15 biobanks; 54%) make their samples available for research through open (36%) or collaborative (18%) access, and 43% (12 biobanks) have study-specific access (Fig. 4).

Types of access through which WRH biobanks make their samples and/or data available to researchers: open access (any researcher can apply for samples and/or data); collaborative access (only collaborators of the research group/biobank can apply to access samples and/or data); study-specific access (only researchers linked to a particular study can apply to access samples and/or data); no access (samples and/or data are used exclusively by the group managing the biobank).
Equipment and consumables
The majority of the biobanks hold frozen specimens, and the most common specimen storage requirement is −80°C freezers (24 biobanks; 86%), followed by LN2 cryotanks (14 biobanks; 50%) (Fig. 5). Almost half of the biobanks have two or more storage temperature requirements (13 biobanks; 46%), and almost a third of the biobanks have three or more (9 biobanks; 32%).
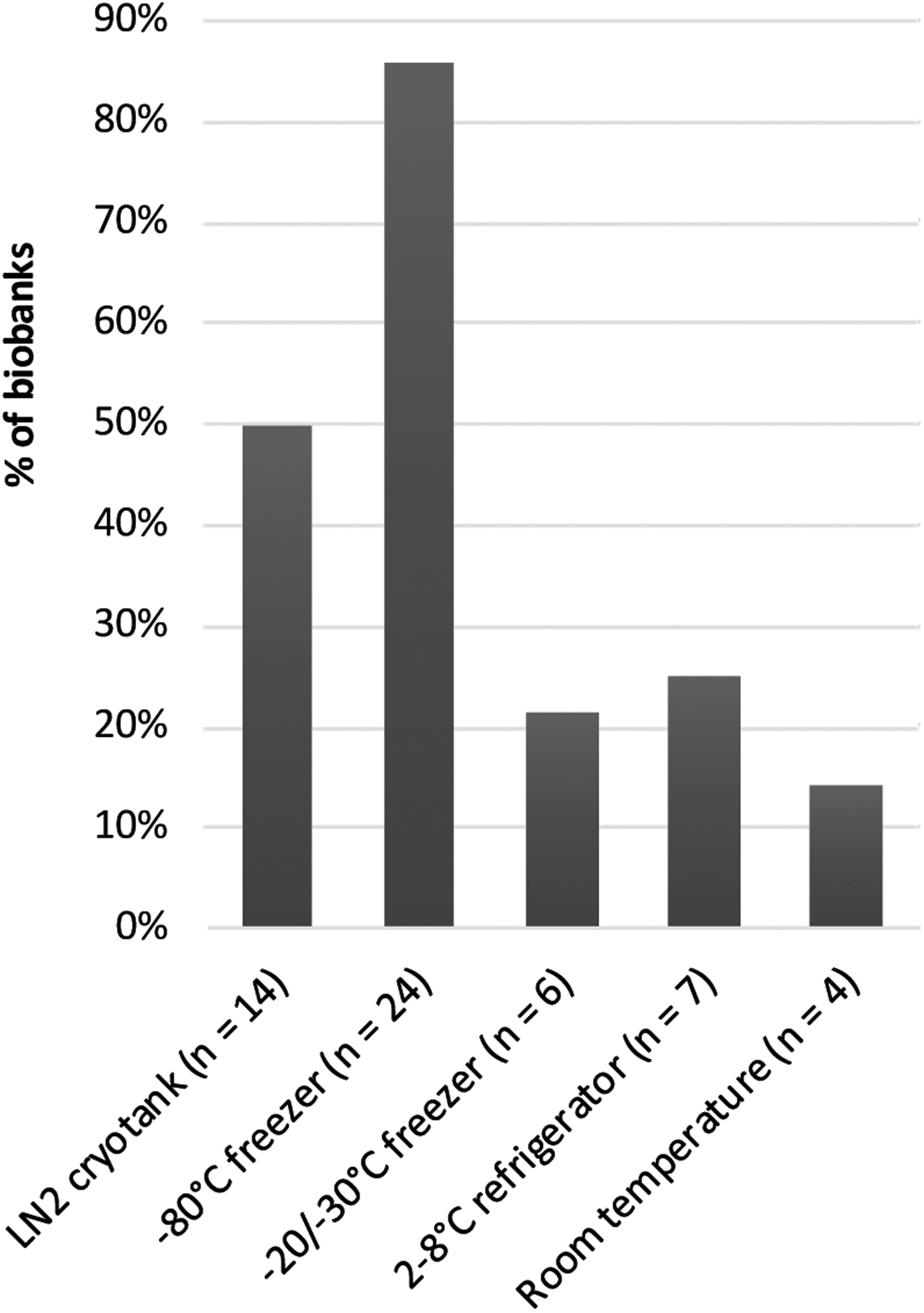
Storage temperature requirements of WRH biobanks. Thirteen biobanks (46%) require ≥2 storage temperatures, and 9 biobanks (32%) have ≥3 storage temperatures.
With the majority of biobanks storing frozen specimens, it follows that tubes are the most used specimen container (25 biobanks; 89%). There was a large variety of tubes used, ranging from 0.7 to 10 mL, and of 30 different tubes listed (manufacturer and volume), 20 were used by only one biobank. The tube volume most commonly used is 2 mL. Other storage containers listed were Petri dishes/agar plates, containers for O.C.T. (optimal cutting temperature) compound, cassettes, and Guthrie cards.
Quality management
A wide range was observed in the level of formalized quality management in place at the biobanks, in regards to both risk management and quality assurance (QA) for sample integrity. A little over half of the biobanks (16 biobanks; 57%) have a formal disaster plan that includes backup storage facilities. Of those biobanks that do have a formal disaster plan, some have backup storage in the same building (e.g., allocated space in another freezer), and others have off-site backup, either at a different organization on the WRH campus, and/or at distant geographical locations.
A significant portion of the biobanks (20 biobanks; 71%) do not have a QA or quality control (QC) program in place. This response is not necessarily indicative of the level of QA/QC in practice however, as the question asked was about a formal program that is currently in place with clearly defined criteria and regular compliance audits. Of the 8 biobanks (29%) that do have a program in place, there was a range of QA and QC measures described in the free text responses, from simple measures to full programs based on international best practices or standards.
Funding
Most of the biobanks (18 biobanks; 64%) rely on peer-reviewed external grant funding for support. A number of biobanks also hold other forms of funding including internal funding, infrastructure funding, and donations (Fig. 6). Only a quarter of the biobanks (7 biobanks; 25%) have a cost-recovery schedule in place for researchers accessing biospecimens and/or data.

Types of funding obtained by WRH biobanks. “Internal” funding includes institutes, hospitals, or local health district funding for biobank staff. “Other” includes various other funding sources, both private and public.
Areas of support requested
At the end of the questionnaire, biobanks were asked how central support could facilitate their biobanking activities. The free text responses identified three main areas where support is needed:
IT support
T support was the most frequently (14 biobanks; 50%) mentioned area of support. Specific requests included custom-built databases; databases to link donors to many sample collections; linking of pathology data with hospital medical records; and IT support for maintenance and routine upgrading of databases.
Staff support
Many of the biobanks (11 biobanks; 39%) requested additional personnel to help with their activities, including sample collection and/or processing support; data collection and data entry support; coordination of sample transport from collection sites; centralized specimen reception and handling; distribution of samples to researchers; general laboratory support (research assistants and laboratory technicians); and pathologist input.
Infrastructure support
The biobanks requested a range of infrastructure support, including more freezer space; backup storage; QA for stored samples; and automated blood processing.
Several other responses within the questionnaire were consistent with the extent and areas of responses around central support. When biobanks were asked whether they have the capacity to synergize with other biobanks for collection and/or storage, 20 biobanks (71%) responded “yes.” Most biobanks are also interested in linking their data through data linkage projects (18 biobanks; 64%); obtaining templates for standard operating procedures and minimum data sets (17 biobanks; 61%); and a coordinated effort to obtain discounts on lab consumables (24 biobanks; 86%).
Discussion
Before embarking on a project to develop a synergistic operating model for the large group of biobanks based at Westmead, it was necessary to first gather current information to understand their existing operations and requirements. The questionnaire developed for this study took an exploratory approach that successfully illustrated the previously unknown landscape of biobanking at WRH, and provided valuable information to inform the next step of the project. A report was prepared to disseminate the findings of the questionnaire to all of the participating biobanks and to the WRH executive.
Three main findings of the information gathered were as follows: (i) the substantial resource that WRH biobank collections collectively represent; (ii) the main challenges that are likely to be faced in working toward harmonization; and (iii) the significant duplication of efforts between the biobanks, representing opportunities for benefits through collaboration.
A powerful resource for translational research
The questionnaire substantiated prior knowledge that Westmead is a center of excellence in biobanking. The biobanks are led by investigators affiliated with all of the WRH partner organizations, highlighting the commitment to and credentials in biobanking on the precinct. Characterization of the collective resource highlighted the significant depth and breadth of clinically important samples collected and stored by the biobanks. A particular strength was shown in cancer and microbial collections that make up 39% of all WRH biobanks (11 biobanks).
The collated findings of the questionnaire bring to light the major research resource that biobank collections at Westmead represent. Not only do these collections facilitate many of the translational research projects on site, but half (15 biobanks; 54%) of the WRH biobanks have open or collaborative access policies. Of these biobanks, 12 (46% of biobanks that obtain consent) also obtain consent for unspecified future research. Taken together this represents a powerful resource for translational research, both on campus and to the research community nationally and internationally.
In comparison to other research enabling core facilities on campus, the significance of this resource has been relatively hidden, with separate standalone biobanks running independently (though individual biobanks network to various extents within their specialist areas). Core services for biobanks could bring greater visibility and connectivity for those biobanks by facilitating researchers' access through a central contact point. For those biobanks who were happy to be listed, their details are now included on the WRH website. 3
Challenges for harmonization
With 28 biobanks that have been established independently in response to requirements in different fields of research, it is unsurprising that a significant diversity of operations has evolved. The diversity highlighted by the questionnaire in certain areas represents some of the challenges that will be faced moving toward a standardized model.
One of the most evident diversities was the many different types, brands, and volumes of sample tubes and other sample containers used by the biobanks. The most common volume was 2 mL, which often holds a much smaller working volume of liquid samples. Robotic storage is the best-practice solution for the future, 4 and this will require compatible tubes with two-dimensional barcodes, which were not in use by any of the biobanks. Additionally, the most compact storage systems require the smallest storage tubes for any given working volume. Hence, it is likely that most biobanks would need to change their sample processing to comply with this transition.
The diversity of databases used by the biobanks likely presents the most significant challenge for standardization. A common IT platform is seen as a desirable goal of the initiative, contributing to efficiency and reduced costs, and for participating biobanks this will involve the challenge of preparing datasets for migration.
A third challenge highlighted by the questionnaire is the gap to bridge to reach best-practice guidelines for quality management. A lot of biobanks do not currently have a formal QA/QC program in place, or an adequate risk management plan. In combination with the large number of requests for staff and infrastructure support, this result suggests that the underlying issue is resource constraints; significant staff time and equipment is required to implement and maintain a full quality management program. 5
The introduction of central biobanking support, including managed storage facilities and specimen processing services, will provide new options and flexibility to help biobanks to address these gaps. Central services will relieve biobanks of parts of their operations, allowing time for transitioning to standardized and best practices. For biobanks that have been established as part of a research project or department, central services will enable biobank management to be outsourced, freeing up time to focus on research, and consequently adopting best-practice biobanking through the services.
Opportunities for synergy
The number of biobanks that have become established across the Westmead campus demonstrates the necessity of biobanks in a translational research hub, and also the significant opportunity for biobanks to benefit from a synergistic model. Twenty-eight biobanks operating independently represents significant duplication, both of efforts and infrastructure; hence a lot of potential for cost savings through collaboration and centralization. Going forward, the project aims to address these opportunity costs and gain from economies-of-scale and enhanced operational efficiencies.
This questionnaire study has indicated a significant capacity of WRH biobanks to synergize their activities with other biobanks in the precinct. Three main areas where biobanks would benefit from central services were indicated: IT support, staff support, and infrastructure support. Further advantages of moving toward a synergistic model will be improvements in standardization of methods, quality management, and access.
Significant gains that could result from collaboration were evident in responses about storage facilities, with many biobanks having two or more different temperature requirements for their samples. Reliable and well-maintained infrastructure is crucial for contemporary biobanking, but it is expensive. Especially for −80°C freezers and LN2 storage, central services could mean that biobanks only pay for the space they need, and do not have to manage the facility themselves. 6 In addition, central management of a QA/QC program including backup storage will ease the burden on each biobank.
The questionnaire responses around data also showed a major area for potential cost-savings. Many of the biobanks collect a breadth of data-fields that is very costly of staff time. In future, if biobanks can transition to a common IT platform, they stand to benefit greatly from data-linkage projects that will avoid the need to duplicate data from health databases to research datasets.
Despite the likely challenges for harmonization discussed, the advantages that biobanks and researchers could gain through collaboration make it worthwhile to initiate efforts to work toward a synergistic operating model. Moreover, the questionnaire has brought to light the inherently unstable funding base for the majority of independent biobanks relying on peer-reviewed grants. This aspect alone makes transition to a more sustainable model imperative.
Limitations and next steps
While the questionnaire developed for this study served local priorities at WRH, a notable limitation is that it did not provide quantitative data. Ideally, more detailed information would have been obtained for planning central support, in particular around rates of recruitment, sample numbers collected and released, and cost of operations. However, this was not attempted in this initial information gathering phase for several reasons:
The depth of information gathered was limited by available resources, as described above. Additionally, since the extent of biobanking operations in the precinct was an intended finding of this study, it could not be predicted in advance what level of undertaking a more thorough approach would be.
Willingness to adopt a new model was previously unknown, so it was possible that resources could be misspent on information gathering that would not translate for the intended purpose of the larger project.
Information will be gathered in a number of ways as the project develops, and the subsequent stage of the project was to launch core biobanking facilities developed with the input of user consultation.
Further quantitation of the size of an individual biobank's collections would not inform a prediction of the level of adoption of core services. It is planned that newly introduced facilities and services will be scaled gradually in response to demand.
The level of duplication between biobank operations on the WRH campus identified by this study points to significant cost and other benefits that could be achieved through a more synergistic model. Though it was not feasible to collect the metrics required to measure the benefits of centralization from the full cohort of WRH biobanks, going forward the subset of biobanks that utilize core facilities will be of interest and benchmarks developed for before/after comparisons.
As highlighted by Vaught et al., 7 “Success” is dependent on many different factors—technical, ethical, legal, and financial. As this fledgling service has comparable ethical and legal factors across the parties, then technical and financial imperatives become the main measures on which to base benchmark parameters. Financially, the success of centralization can be measured in each of the three areas where a need for support was indicated: IT support, staff support, and infrastructure support. For example, a measure of financial gains in IT and staff support would be the number of full-time equivalents of IT professionals or Biobank officers dedicated to the collective biobanks versus the number proposed in the integrated model. For infrastructure, financial gains are expected through sharing of equipment, which can be measured by equipment numbers and value (e.g., number and cost of freezers and LN2 cryotanks between the collective biobanks before and after adopting central facilities).
The major technical imperative for a synergistic operating model of biobanking at WRH is to support the best quality research though the provision of high-quality well-annotated specimens. This study indicated a need for support to raise the level of formalized quality management across WRH biobanks. This will be addressed in the new model by centrally maintaining currency with both methodologies and contemporary changes in research practices. Central biobank staff will be specialists in the biobanking field and apace of any changes and recommendations in evidence-based practice, QA methodologies and ethical and legal practices. Two technical benchmarks for success will be an increase in the number of certified biobanks and an increase in the number of research projects collectively supported by WRH biobanks.
Footnotes
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.