
Abstract
Introduction:
Personalized treatment, supported by biomarkers, would improve survival of ovarian cancer patients. RNA molecules are potentially important biomarkers. The Danish CancerBiobank provides an infrastructure for handling and storage of biological material, including RNA, from Danish cancer patients. The aim of this study was to investigate the effects of handling-time and fresh-freezing versus RNAlater® fixation on RNA degradation in solid tissue from pelvic mass samples.
Materials and Methods:
We evaluated RNA quality in surgical tissue from patients with a pelvic mass. Corresponding samples were either fresh-frozen or fixed in RNAlater, at eight different time points after the surgery. Integrity was measured using a bioanalyzer, and the amount and quality were further investigated by quantitative reverse transcription–polymerase chain reaction measuring the expression of housekeeping genes B2M and HPRT1.
Results:
Our results show that tissue RNA is stable up to at least 180 minutes after the surgery, as the quality was comparable to the quality of RNA handled immediately. Likewise, patient RNA was of acceptable quality after both fresh-frezing and RNAlater fixation, but RNAlater fixation was slightly more effective for RNA preservation.
Discussion and Conclusion:
Our data suggest that RNA in pelvic mass samples is relatively stable. Knowledge about RNA stability is an important prerequisite for research in RNA biomarkers, where the challenge is to balance the need for careful RNA handling and storage with the need for effective large-scale biobanking in a busy clinical setting where patient treatment is the main priority.
Introduction
The incidence of cancer continues to increase for both sexes; female breast cancer, lung cancer, and prostate cancer are among the most frequently diagnosed cancers.1,2 Among women in developed countries, ovarian cancer (OC) is the fifth most frequent cancer and it continues to be the most lethal gynecological cancer. 1 To improve the survival among OC patients, there is an urgent need for new biomarkers to promote diagnosis and personalize the treatment.
Expression profiling studies indicate that changes in expression levels of certain messenger RNAs (mRNAs) may be used to distinguish OC from normal tissue, to determine histological subtype and grade, and to predict survival.3–5 Thus, RNAs seem to have potential as new diagnostic, prognostic, or predictive biomarkers in OC as an alternative to proteins. The mRNA represents the first level of functional expression of the genome. It has traditionally been considered a highly fragile molecule requiring fast sample handling and low temperatures or fixation in commercial RNA-stabilizing buffers to prevent their degradation by cellular RNases. 6 However, fixation increases the costs and introduces additional hands-on steps that may unnecessarily complicate high-throughput large-scale biobanking routines.
The nationwide Danish CancerBiobank, established in 2010 and a part of the Bio- and Genome Bank Denmark, provides an infrastructure for the collection, handling, and storage of biological material from Danish cancer patients across all cancer types. The material can be used for either diagnostic purposes or translational cancer research to improve diagnosis and treatment of malignant diseases. According to nationally approved Standard Operating Procedures (SOPs) in the biobank, tissue is stored both as fresh-frozen and RNAlater®-fixed samples and should according to national guidelines be handled within 1 hour from the surgery. To further optimize the tissue SOPs for large-scale biobanking, additional data are needed on how to achieve optimal RNA stability and quality.
The aim of the present study was to investigate the effects of handling-time and fresh-freezing versus RNAlater fixation on RNA amounts and quality in solid tissue samples. To assess the influence of these conditions on RNA stability, we evaluated RNA integrity and amounts in operational tissue from patients with a pelvic mass.
Materials and Methods
Patients and samples
Women aged 35–70 years and scheduled for operation due to suspected malignant gynecological disease were invited to participate in the study. Samples were taken from the surgical specimens simultaneously with tissue isolation for routine analyses, before any treatment was initiated. Patients were excluded from the study if tissue amounts were too small for sampling. Six patients were included in the study. All participants gave their written and verbal informed consent to the study before their participation. The study protocol was approved by the Danish Ethics Committee (H-B-2008-037) and the Danish Data Protection Agency (2008-41-2353).
Each gynecological cancer specimen was covered to avoid drying and kept at room temperature. Eight individual but neighboring samples were isolated from the tumors at 0, 15, 30, 45, 60, 90, 120, and 180 minutes after the surgery. Each sample was divided into three parts: one part was formalin-fixed and paraffin-embedded, one part was snap-frozen in dry-ice cooled isopentane (2-methylbutane) and stored at −80°C for RNA analysis, and one part was fixed in 0.5 mL RNAlater (Invitrogen) at 4°C for ≥24 hours and, after removal of excess RNAlater, stored at −80°C until RNA analysis. The tissue parts were not larger than the tip of an Eppendorf tube (<100 mg) and therefore covered in more than 5 volumes of RNAlater.
The tissue was stored 5–7 years. All tissues were pathologically verified for histological subtype and grade, and tumor stage was evaluated according to the International Federation of Gynecology and Obstetrics (FIGO) standards (Table 1). The degree of tissue necrosis and the tumor percentage were established by a pathologist from blinded hematoxylin and eosin-stained sections (Table 1). All human tissues were handled according to the guidelines of the Danish CancerBiobank.
Pathological Characteristics of Patient Samples
Patients: Women aged 35–70 years and scheduled for operation due to suspected malignant gynecological disease. Six patients were included in the study. All tissues were pathologically verified for histological subtype and grade, and tumor stage was evaluated according to the FIGO standards. The degree of tissue necrosis and the tumor percentage were established by a pathologist from blinded H&E-stained sections. The FFPE tissue for patient 1 was not available at the time of H&E staining.
FFPE, formalin-fixed and paraffin-embedded; FIGO, International Federation of Gynaecology and Obstetrics; H&E, hematoxylin and eosin.
Determination of RNA quality and integrity
Approximately 30 mg of tissue (measured as 3 mm3) was cut from the snap-frozen or RNAlater-fixed tissue parts using a scalpel. The tissue was cut on a metal plate on dry ice in a Styrofoam box, to keep it cold. Each 30 mg tissue block was homogenized immediately in 600 μL cold lysis buffer from the RNeasy Mini Kit (Qiagen, RLT-buffer with 14.3 M β-mercaptoethanol; Sigma), while kept on ice, using a TissueRuptor® Homogenizer (230 V, 50/60 Hz; Qiagen) and stored for up to a year at −80°C until RNA isolation. RNA was isolated using the RNeasy Mini Kit (Qiagen) and 70% and 96%–100% ethanol (Region H pharmacy) including DNA digestion using the RNase-Free DNase Set (Qiagen) according to kit instructions. The RNA was eluted in 2 × 50 μL RNase-free water for all samples. Purified RNA was stored at −80°C for up to 2 years.
Total RNA concentrations were measured using NanoDrop. However, as NanoDrop does not discriminate between intact and degraded RNA molecules, RNA integrity (RNA integrity numbers [RIN]) and quality of each sample (<500 ng/μL, 1 μL) were determined using the Agilent 2100 Bioanalyzer and the Agilent RNA 6000 Nano Kit according to kit instructions.
The presence of high-quality nondegraded RNA in patient samples was confirmed by quantitative reverse transcription–polymerase chain reaction (qRT-PCR) of housekeeping genes B2M and HPRT1. cDNA was synthesized from 100 ng RNA (measured on NanoDrop) using the SuperScript™ VILO™ cDNA Synthesis Kit (Invitrogen). The resulting 20 μL of cDNA was diluted in 50 μL Tris buffer, and transcript levels of B2M and HPRT1 were measured from 5 μL diluted cDNA in duplicates using the Brilliant III Ultra-Fast QPCR Master Mix (Agilent Technologies) and exon spanning probes with FAM™ reporters and matching primers (TaqMan® Gene Expression Assays Hs99999909_m1 and Hs99999907_m1; Applied Biosystems). The program used: 5 minutes of hot start activation at 95°C, followed by 40 cycles of 15 seconds of denaturation at 95°C and 30 seconds of elongation at 60°C.
mRNA levels were calculated as relative to an internal control (mRNA level of control = 1), assuming that the cDNA is doubled in each cycle [mRNA level = 2Ct(Ctrl) − Ct(sample)]. This method is similar to the comparative Ct method and enables comparison of samples from the same patient.
Statistical analyses
Statistical analyses of the difference in stability between fresh-frozen and RNAlater-treated samples were carried out using mixed modeling with RIN as the dependent variable for bioanalyzer data and the mRNA levels of housekeeping genes B2M and HPRT1 as dependent variables for qRT-PCR data. Mixed modeling was used because it allows inclusion of more than one explanatory variable. Both analyses were performed with time of treatment and RNAlater treatment/fresh-freezing as explanatory variables and with individual as a repeated measure.
To fulfill the assumption of normally distributed dependent variables, B2M and HPRT1 mRNA levels were log-transformed where applicable, resulting in estimated ratios between RNAlater and fresh-frozen samples after back transformation. Results are presented with 95% confidence intervals, and p-values <5% are considered significant. Model assessment was carried out using martingale residuals. All statistical calculations were performed using SAS (v9.4; SAS Institute, Cary, NC).
Results
Tissue RNA is stable up to at least 180 minutes after the surgery
The integrity of patient RNA was measured using an Agilent 2100 Bioanalyzer. Although there was low variation between samples from the same patient, there was no significant RNA degradation over time (p = 0.91) (Figs. 1A, 1B, 2A, 2B, 3A, 3B, and 4). RNA purified after 3 hours of cold ischemic time was not more degraded than RNA from tissue that had been frozen or fixed immediately after the surgery. The RIN ranged from 3.2 to 9.2. However, the majority were above 6. There was no significant difference in RIN from RNAlater-treated samples or fresh-frozen samples (estimated difference: 0.45 [CI: −0.199 to 1.093], p = 0.17).
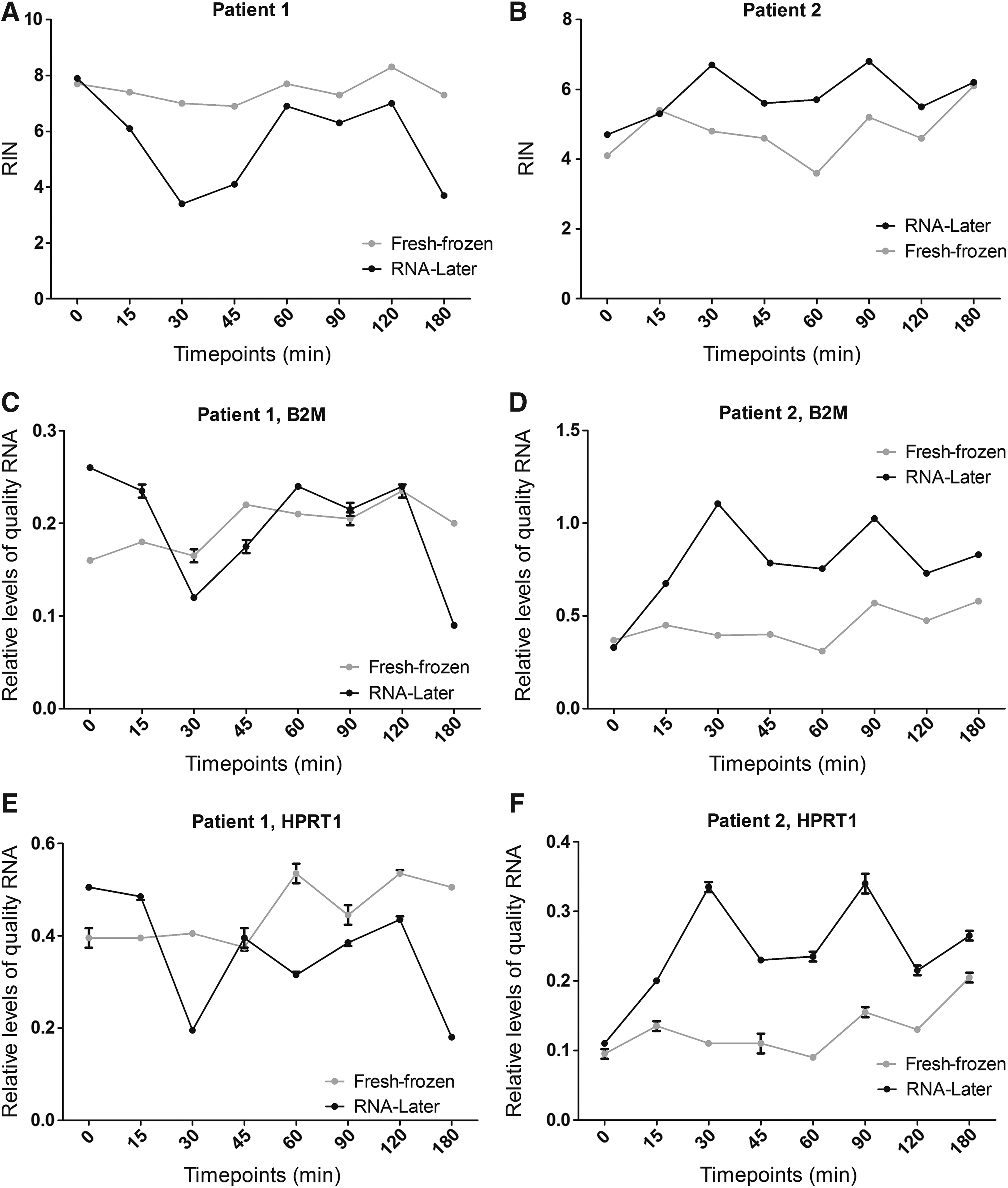
RNA quality of patients 1 and 2.

RNA quality of patients 3 and 4.

RNA quality of patients 5 and 6.
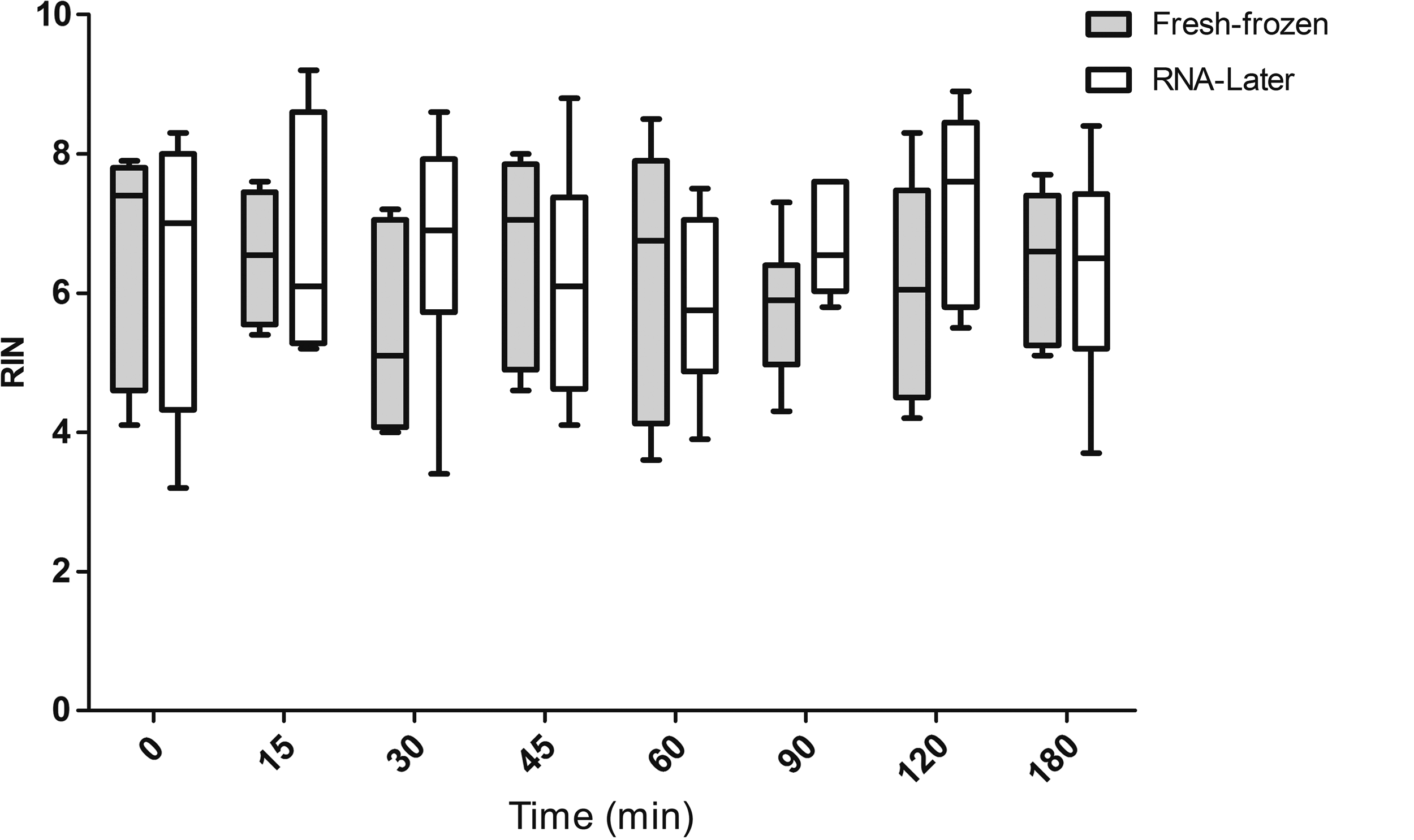
RNA integrity of all patients. RNA integrity measured on Agilent 2100 Bioanalyzer. RIN values of fresh-frozen (gray boxes) and RNAlater-fixed (white boxes) are pooled for all patients and compared for each time point. RNA degradation is not influenced by time. RNAlater is slightly more effective for RNA preservation than fresh-freezing. Whiskers: minimum to maximum.
Tissue RNA can still be detected in qRT-PCR after 180 minutes
As some of the RIN values were below 6 and NanoDrop detects both degraded and intact RNA, we wished to confirm that the samples contained enough high-quality functional mRNA to obtain qRT-PCR data. We did that by measuring the amount of intact mRNA from housekeeping genes B2M and HPRT1 by qRT-PCR. The results were in good accordance with the bioanalyzer data (Figs. 1C–F, 2C–F, and 3C–F).
All samples were amplified, and the Ct values ranged from 18.53 to 30.26. High-quality samples with a high RIN came up early and had low Ct values in both qRT-PCRs, whereas samples with a lower RIN came up later in the qRT-PCRs, as expected. This was especially clear for the correlation between HPRT1 mRNA levels and RIN values (R = 0.92 for fresh-frozen samples and R = 0.62 for RNAlater-treated samples), whereas the correlation was less evident for B2M mRNA levels (R = 0.26 for fresh-frozen samples and R = 0.64 for RNAlater-treated samples). There was no reduction in RNA levels over time (p = 0.99 for both B2M and HPRT1).
Although a trend toward better RNA quality was seen in RNAlater-treated tissue when qRT-PCR data for the two genes were analyzed separately (B2M: estimated ratio 39% [CI: 0% to 93%], p = 0.051, HPRT1: estimated ratio 28% [CI: −8% to 78%)], p = 0.147), no significant difference was observed between RNAlater-treated samples and fresh-frozen samples. However, pooling data from the two genes suggested that RNAlater was better at preserving the RNA compared with fresh-freezing (estimated ratio 33% [CI: 3% to 72%], p = 0.03).
Discussion
Personalized treatment is an important step toward improving or prolonging the lives of OC patients. Biomarkers are the foundation of personalized treatment and RNA molecules are promising biomarker candidates in OC, as already illustrated by several studies, which have identified mRNA profiles that can distinguish between long- and short-time survivors.7–13 However, it is a requirement that we can handle and store RNA effectively, but at the same time carefully, to prevent RNA from degradation by RNases during handling in the busy environment of a hospital or clinic where the patient is in focus. Strict guidelines from the CancerBiobank about tissue handling time can be a challenge in a clinical setting.
Our data suggest that RNA in pelvic mass samples is stable for up to 3 hours after the surgery. This creates more possibilities when it comes to research in RNA cancer markers. It may seem surprising that RNA, normally considered fragile, can avoid degradation for such a long period after tissue has been removed from the body, but similar results have been observed for the lung, liver, breast, colon, and tonsil tissue, whereas RNA in pancreatic tissue have been shown to be stable in RNAlater for at least 30 minutes.14–18 RNA is supposedly protected from RNases as long as the cells are alive and intact.
The study must be considered preliminary due to the small patient cohort. However, the consistency of the results suggests that RNA from gynecological tumor tissue is quite stable. As most of our patients suffered from different ovarian conditions, from benign tumors to serous adenocarcinoma, the stability of RNA may be a general phenomenon among ovarian tumors.
As one of the samples was an appendix tumor, it is likely that the RNA stability observed in this study is a general trait in several tumor types, but it is always necessary to examine the RNA stability before making biomarker studies in new tissue types. There are several tissues where RNA can be expected to be less stable, for example, in tissue with high enzymatic activity such as pancreatic tumors. It is also important to assess the stability for each new biomarker identified to understand the exact patterns of expression and degradation for a given tumor type. In this study, we only looked at general RNA integrity and levels of a few housekeeping genes.
Even though we did not see a significant decline in RNA stability over time, we did observe some variation in RNA quality among samples from the same patient, despite that they were neighboring fractions of the same tumor. The patterns of variation in RNA quality for each patient were similar in all molecular analyses and therefore most likely reflect tissue heterogeneity rather than artifacts introduced during analysis. Overall, samples with low RNA quality came from tissue that was difficult to homogenize. An example of this was the fibroma of patient 4. However, the observed variation in RNA quality does not reflect variation in tumor percent or tissue necrosis as scored by the pathologists. Instead, we suggest that it reflects heterogenic gene expression, which has been described for OC previously. 19
To the best of our knowledge, stability of ovarian tumor tissue has not been examined before, but RNA stability has been tested for other tissues. Most studies which have compared RNAlater with freezing conclude that RNAlater is as good as, or slightly better than fresh-freezing, when it comes to preservation of RNA in mammalian tissue.20–25 One study found that RNAlater was much more effective in preserving RNA from breast cancers compared with fresh-freezing, but in that study, the tissue was minced, reducing the protection of the RNA from RNases. 26
In our study, tissue kept in RNAlater generally had a firmer consistency and was slightly more difficult to homogenize. Others report that RNAlater fixation introduces tissue condensation, cell shrinkage, and hyperchromatic nuclei. 17 Macroscopic effects of RNAlater fixation were not evaluated in the present study. Despite the firm consistency of the tissue, our data indicate that RNAlater fixation may be slightly better at preserving RNA from pelvic tumors compared with fresh-freezing. However, this was not consistent for all patients and only significant when measured by qRT-PCR and when data from both genes measurements were pooled. The low number of participants in the study may explain why this difference was not observed when the genes were analyzed individually.
The difference in RNA quality between RNAlater-fixed tissue and fresh-frozen tissue is very small, from which we can conclude that it is possible to obtain a high RNA stability from fresh-frozen tissue, comparable to that from RNAlater-fixed tissue, if samples are kept cold and clean before and under homogenization and until RNA purification. This is highly interesting, as RNAlater complicates tissue-handling in the clinic and is a disadvantage when it comes to large-scale and high-throughput biobanking. Moreover, RNAlater is an extra cost and commits the tissue for RNA purification so it is not accessible for other analyses.
It can be debated whether it is necessary to continue to prioritize RNAlater-fixed sampling of pelvic masses in a biobank setting. However, RNAlater protects the RNA against accidents like freezer breakdowns or faulty transportation, whereas fresh-frozen tissue is only usable if everyone who is in contact with the sample, after it leaves the biobank, are skilled enough to keep the sample clean and cold.
Our data suggest that RNA in pelvic mass samples is not degraded in the first 3 hours after the surgery. This knowledge will be a great help during future research in biomarkers and personalized treatment of OC and, hopefully, bring us one step closer to faster diagnosis and better treatment of the disease.
Footnotes
Acknowledgments
This work is supported by Mermaid III. The Danish CancerBiobank is acknowledged for biological material and data regarding handling and storage.
Author Disclosure Statement
No conflicting financial interests exist.