
Abstract
Background:
The best storage preservation method for maintaining the quality and safety of human decellularized allograft heart valves is yet to be established.
Objective:
The aim of the present study was to evaluate the stability in terms of extracellular matrix (ECM) integrity of human heart valve allografts decellularized using sodium dodecyl sulfate-ethylenediaminetetraacetic acid (SDS-EDTA) and stored for 6, 12, and 18 months.
Methods:
A total of 70 decellularized aortic and pulmonary valves were analyzed across different storage times (0, 6, 12, and 18 months) for solution pH measurements, histological findings, cytotoxicity assay results, biomechanical test results, and microbiological suitability test results. Continuous data were analyzed using one-way analysis of variance comparing the follow-up times.
Results:
The pH of the stock solution did not change during the different time points, and no microbial growth occurred up to 18 months. Histological analysis showed that the decellularized allografts did not present deleterious outcomes or signs of structural degeneration in the ECM up to 12 months. The biomechanical properties showed changes over time in different aspects. Allografts stored for 18 months presented lower tensile strength and elasticity than those stored for 12 months (p < 0.05). The microbiological suitability test suggested no residual antimicrobial effects.
Conclusion:
Changes in the structure and functionality of SDS-EDTA decellularized heart valve allografts occur after 12 months of storage.
Introduction
Valvular heart disease is an important public-health problem related to high morbidity and mortality rates worldwide,1,2 however, there are no ideal options among the current treatments for heart disease demanding valve replacement. 3 As mechanical valves have poor hemocompatibility, they require a lifetime of anticoagulant therapy. Nevertheless, biological valves, either of allogeneic or xenogeneic origin, have a limited lifespan owing to structural degeneration, calcification, and immunological inflammation.4–6 The use of tissue engineering methods to create heart valve scaffolds has the potential to overcome the fundamental drawbacks of more traditional heart valve replacements.7,8
Tissue-engineered heart valves (TEHVs) have shown considerable advances in the field of valve replacement. 9 Mainly two types of scaffold designs have been developed from biological- and synthetic-based materials. 10 Currently, various techniques are used to generate TEHVs, including decellularization, molding/suturing, electrospinning, and three-dimensional bioprinting. 11 Decellularized TEHVs are prepared by decellularization of native animal 12 and human tissues, 13 and are very attractive scaffolds because of their complex natural anatomical geometry that supports an immediate physiologic and hemodynamic environment. 14 Decellularization has been proposed as a promising method to diminish or even abolish allograft antigenicity and thus avoid the immune response. 15 Clinical experience with decellularized TEHVs has demonstrated a higher freedom from valve dysfunction or replacement than with standard cryopreserved allografts.16,17 Decellularization of TEHVs has been the most successful technique to be translated into the clinic, and is currently an increasingly common strategy in regenerative medicine and tissue engineering. 11 Decellularized TEHVs have some advantages over conventional prostheses and conventional cryopreserved allografts.6–9 Decellularized TEHVs are composed of biological materials that can positively affect cell differentiation and serve as building blocks during the remodeling process. 18 In addition, decellularized TEHVs do not necessitate complete biodegradation and often maintain the mechanical anisotropy of the native valves from which they are derived. 19
Many protocols for decellularization, as well as varying concepts for preservation after processing, have been proposed and applied. Strategies for decellularization include the use of physical methods (e.g., agitation, freeze-thaw, sonication, temperature control), chemical agents (e.g., detergents, hypo-/hypertonic buffers, acids, bases, alcohols), and biological agents (e.g., enzymes, chelating agents). 15 These methods also differ in effectiveness in removing antigens from the extracellular matrix (ECM) scaffold, such as cellular and nuclear materials, as well as lipids and carbohydrates, which can also function as antigens. 20
Human TEHVs ideally need to be processed and to have long-term storability to ensure off-the-shelf availability 21 and enhance safety by allowing for quality testing before use. 22 However, during storage, environmental factors can affect the stability of biological systems by modifying or degrading biomolecules, thus compromising decellularized TEHVs. 23
The best storage preservation method for maintaining the quality and safety of decellularized TEHVs is not well defined. Different protocols for the preservation of unprocessed allografts have been reported, such as the use of glutaraldehyde, 24 glycerol, 25 or ethanol + glycerol + polyethylene glycol 26 ; fresh-wet storage at 4°C27,28; and cryopreservation.29,30 Among these, cryopreservation of homografts has been the gold standard since 1968. 31 Cryopreservation has the advantage of a long storage period; however, deterioration and calcification of cryopreserved valves can occur because of interstitial ice formation.32–34 This condition can affect the long-term graft durability. Nowadays, freeze-drying of biologic heart valves is currently being investigated 6 ; however, freeze-drying leads to the collapse of the ECM structure and disruption of biomolecules. 21 The decellularization process allows valves to be stored in a hypothermic preservation condition by maintaining the storage temperature at around 4°C–10°C. 35 However, no consensus yet exists on how human decellularized TEHVs are best preserved for long-term storage. 21
The aim of the present study was to evaluate the stability in terms of ECM integrity of human decellularized TEHVs stored in isotonic saline solution up to 18 months.
Materials and Methods
Experimental design
We analyzed human decellularized allografts immediately after the decellularization process (0 month) and after storage for 6, 12, and 18 months. All samples were protected from light and stored for 18 months under refrigeration conditions. The volume, turbidity, sterility (microbiological control), and pH of the storage solution; integrity of package; and macroscopic and microscopic findings were analyzed.
Donors and samples
Hearts from human nonheart-beating and heart-beating donors were obtained under aseptic conditions. Seventy aortic and pulmonary valves were dissected using aseptic techniques in a class II-A laminar airflow cabinet. A total of 40 valves (pulmonary = 20, aortic = 20) were used for the biomechanical assay. Ten valves were analyzed immediately after decellularization, 10 valves were stored for 6 months, 10 valves were stored for 12 months, and 10 valves were stored for 18 months. For histological, immunohistochemical (IHC), and morphometric analysis, three pulmonary valves and three aortic valves were included for each time point (immediately after decellularization and at 6, 12, and 18 months of storage). A total of 24 valves (pulmonary = 12 and aortic = 12) were used for cytotoxicity assays. The study was approved by the Ethics Committee of Pontifical Catholic University of Paraná (approval no. 1.455.773).
Decontamination of allograft valves
The heart grafts were decontaminated in RPMI 1640 medium (Sigma-Aldrich, St. Louis, MO) with low concentrations of antibiotics (240 mg/L cefoxitin, 50 mg/L vancomycin, 120 mg/L lincomycin, and 100 mg/L polymyxin B) and kept for 24 hours at 2°C–8°C.
Preparation of decellularized allografts
Allograft heart valves were treated under shaking conditions with a solution of 0.1% sodium dodecyl sulfate (SDS, w/v; Sigma-Aldrich) and 7 mM ethylenediaminetetraacetic acid (EDTA; Sigma-Aldrich) for 1 day, with fresh solution change every 4 hours at room temperature as previously described. 36 Thereafter, the valves were treated with 70% ethanol (v/v) for 24 hours at room temperature to extract residual detergent. The allografts were rinsed with sodium chloride (NaCl) 0.9% solution (Baxter International, Deerfield, IL) to remove residual substances and cellular debris for 10 days, with fresh solution change every 1 day at 2°C–8°C. Then, the allografts were placed in a polycarbonate container with 200 mL sterile NaCl 0.9% solution and stored at 2°C–8°C.
Microbiological control
Samples for bacterial and fungal cultures were collected from all allografts at five different time points: (1) after antibiotic incubation, (2) after decellularization, (3) after 6 months of storage, (4) after 12 months of storage, and (5) after 18 months of storage. The samples were obtained aseptically in a class II-A laminar airflow cabinet and then membrane filtered. In brief, a 100 mL stock solution was filtered through a 0.45-μm sterile membrane filter (Millipore, Cork, Ireland). Membrane filters were aseptically transferred to a container with 90 mL thioglycollate (Laborclin, Pinhais, Brazil), 90 mL tryptic soy broth (Laborclin), and 90 mL Sabouraud medium (Laborclin) for bacteriological and mycological testing. The samples were cultured for 14 days at 35°C (thioglycollate), 35°C (tryptic soy broth), and 22°C (Sabouraud), respectively, and examined daily for visual evidence of turbidity. 37 Suitability tests were performed according to the United States Pharmacopeia criteria. 38 Positive control was performed with spiked samples of stock solution with 100 colony-forming units (Staphylococcus aureus ATCC 6538, Pseudomonas aeruginosa ATCC 9027, Clostridium sporogenes ATCC 19404, Bacillus subtilis ATCC 6633, Candida albicans ATCC 10231, and Aspergillus brasiliensis 16404). Negative control was performed in a container without samples. The medium was considered suitable if a clearly visible growth of microorganisms was seen.
pH analysis
The commercial 0.9% saline solution for infusion had a pH of ∼5.5. 39 The pH of the storage solution was analyzed using a pH meter (Gehaka, São Paulo, Brazil) before storage and at 0, 6, 12, and 18 months after storage to detect any changes caused by the allografts or the storage conditions. The pH meter ranged from 1 to 14. The stock solution was not changed or replenished during the study.
Histological, IHC, and morphometric analyses
Human decellularized allografts were sampled immediately after the decellularization process (0 month) and after storage for 6, 12, and 18 months for histological analysis. Three millimeter sections were fixed with 10% neutral buffered formalin, embedded in paraffin, and sectioned at 4 μm thickness. The morphological integrity of the conduit and leaflet of the allografts was analyzed using hematoxylin and eosin (H&E) and Russell-Movat pentachrome (RMP) staining (American MasterTech Scientific, Inc., Lodi, CA) under a BX51 optical microscope (Olympus, Tokyo, Japan). In brief, nuclei and elastic fibers were stained black, collagen and reticular fibers were stained yellow, mucin was stained blue, fibrin was stained bright red, and muscles were stained red.
IHC analysis was performed to verify the presence of intermediate filaments by using monoclonal mouse antivimentin antibody, clone V9, and IgG1 (M 0725; Dako, Carpinteria, CA) in the allografts after decellularization and different storage times. Paraffin-embedded tissue samples were cut at 4 μm thickness and mounted on silane-coated slides, dried, deparaffinized in xylene, and rehydrated in sequential ethanol baths (100% and 80%). Heat-mediated antigen retrieval was performed before the slides were incubated with primary antibody (dilution, 1:200) overnight. The reaction product was developed with diaminobenzidine and counterstained with hematoxylin. The specificity of IHC staining was confirmed by omitting the primary antibody. The immunostained slides were observed using an optical microscope (Olympus BX51). Slides were scanned using an Axio Scan.Z1 slide scanner (Carl Zeiss Microscopy GmbH, Jena, Germany), and subsequent image preparation was performed using the Zen lite software (Carl Zeiss). Fresh tissue was used as control.
For morphometry, the expression of ECM components (collagen, elastic fiber, and glycosaminoglycan [GAG]) was assessed on RMP-stained tissues. A total of 50 fields per case were analyzed at × 400 magnification by using an optical microscope (Olympus BX51) and scanned using an Axio Scan.Z1 slide scanner (Carl Zeiss Microscopy GmbH). The results were expressed according to the total area analyzed (1.215,625 μm2).
Direct contact cytotoxicity assay
The cytotoxicity of decellularized allografts (conduits) after the decellularization process and after different storage times was tested in accordance with ISO 10993/535 and Miranda et al. 40 L-929 fibroblasts (ATCC cell line CCL 1, NCTC clone 929) were seeded in six-well plates at a density of 1 × 105 cells/well. Each well, which had an inner diameter of 35 mm, received 4 mL Dulbecco's modified Eagle medium +2 mM glutamine +10% fetal bovine serum. The plates were incubated for 48 hours at 37°C in an atmosphere of 5 ± 0.5% CO2 in air, until a monolayer with >80% confluence was formed. The medium was removed from the wells and replaced with 1.8% agar added with 0.01% neutral red dye. Samples for the triplicate, positive, negative, and blank controls used six-well agar-overlay plates. After an incubation period of 24 hours at 37°C in a humidified atmosphere of 5 ± 0.5% CO2 in air, the inhibition zone around the samples was measured, as neutral red does not stain dead cells. The biological reactivity of the samples was scored from 0 to 4 in accordance with the following criteria: 0 = absent cytotoxicity (absence of a zone of lysis underneath the sample), 1 = slight (zones of cell lysis underneath the sample only), 2 = mild (zones of cell lysis ≤5 mm from the sample), 3 = moderate (zones of cell lysis >5 mm, and ≤10 mm from the sample), and 4 = severe (zones of cell lysis >10 mm but not involving the entire well). In addition, the wells were examined using an inverted microscope (Nikon Eclipse TS 100; Nikon) to observe cell changes. 36
Biomechanical assay
The biomechanical properties of aortic and pulmonary allografts (leaflet and conduit) were evaluated using a biaxial tensile test to compare the effects of storage time on the properties of tensile strength, elongation, and elastic modulus of tissue as previously described. 36 In brief, an EMIC DL 500 universal testing machine was used to perform the tests (Instron, Curitiba, Brazil). The sample, dumbbell-shaped, was based on the ASTM D1708-13 standard because of small size of the tissue available for the tests. To obtain the samples, it was necessary to manufacture a steel-rule die according standard specifications for use in cutting the allograft. Before each test, the thickness, width, and initial length of the sample were provided to the equipment. Thickness and width values are necessary to calculate the cross sectional area and consequently the stress [Eq (1)]. Initial length is necessary to calculate the strain and consequently the percent elongation [Eq (2)]. Thickness was measured with a thickness gauge at 3 points of the tissue. A preload of 0.1 N and a velocity of 5 mm/min were applied during the test.
Stress calculation:
where σ is the stress in megapascal (MPa), F is the force in newton (N), and A is the cross sectional area in millimeters square (mm2).
Percentage elongation calculation:
where %El is the percentage elongation, ΔL is the variation of sample length in millimeters (mm), Li is the initial length of sample in millimeters (mm), and ɛ is the strain in millimeters per millimeter (mm/mm).
Statistical analyses
Continuous data are expressed as mean ± standard deviation and categorical data as frequency. Continuous data were analyzed using one-way analysis of variance comparing the follow-up time, by using GraphPad Prism software (GraphPad Software, Inc.). A p-value of <0.05 was considered significant.
Results
Visual analysis, pH, and haptic evaluation
No consistent significant alterations possibly related to storage time were observed according to macroscopic structure. The integrity of packaging and labels was maintained. There were no changes in the volume and color (no turbidity) of storage solution stored at 2°C–8°C for up to 18 months. The initial pH of the 0.9% saline solution was 5.8. In the first 24 hours of storage, the pH of the solution was 6.06 ± 0.20 in decellularized aortic allografts and 6.01 ± 0.05 in decellularized pulmonary allografts. After 6 months, the pH of stock solution in decellularized aortic allografts was 6.12 ± 0.06 and that in decellularized pulmonary allografts was 6.14 ± 0.05. After 12 months, the pH of stock solution in decellularized aortic allografts was 6.07 ± 0.22 and that in decellularized pulmonary allografts was 6.21 ± 0.09. After 18 months, the pH of stock solution in decellularized aortic allografts was 6.10 ± 0.12 and that in decellularized pulmonary allografts was 6.15 ± 0.12. The difference between the mean of groups was not significant (p > 0.05) (Fig. 1). The decellularized allografts showed similar characteristics in terms of tactile perception.

Comparative analysis of the pH values of the stock solution at 0, 6, 12, and 18 months of storage.
Microbiological assessment
After antibiotic incubation, no growth was detected using the membrane filter technique until 18 months. The suitability test demonstrated no inhibitory effects on the growth of microorganisms used according to the Food and Drug Administration and United States Pharmacopeia criteria.
Analysis of ECM integrity
H&E-stained sections did not present obvious deleterious effects or signs of autolysis in the structure of the ECM due to the preservation method in decellularized aortic and pulmonary valves stored for 6, 12, and 18 months (Figs. 2–4 and 5A–D). The major ECM components were examined using RMP staining (collagen: yellow, elastin: black, and GAGs: blue) (Figs. 2–4 and 5E–H). The decellularized ECM showed elastic fiber fragmentation caused by the process of decellularization. However, the orientation in layers was maintained. ECM fiber rearrangement was observed in aortic and pulmonary decellularized allografts without structure degeneration related to storage time. After the storage period, the morphology of the aortic and pulmonary decellularized allografts was comparable to the newly decellularized ones. No difference in vimentin tissue expression related to storage time was identified (Figs. 2 and 4I–L).
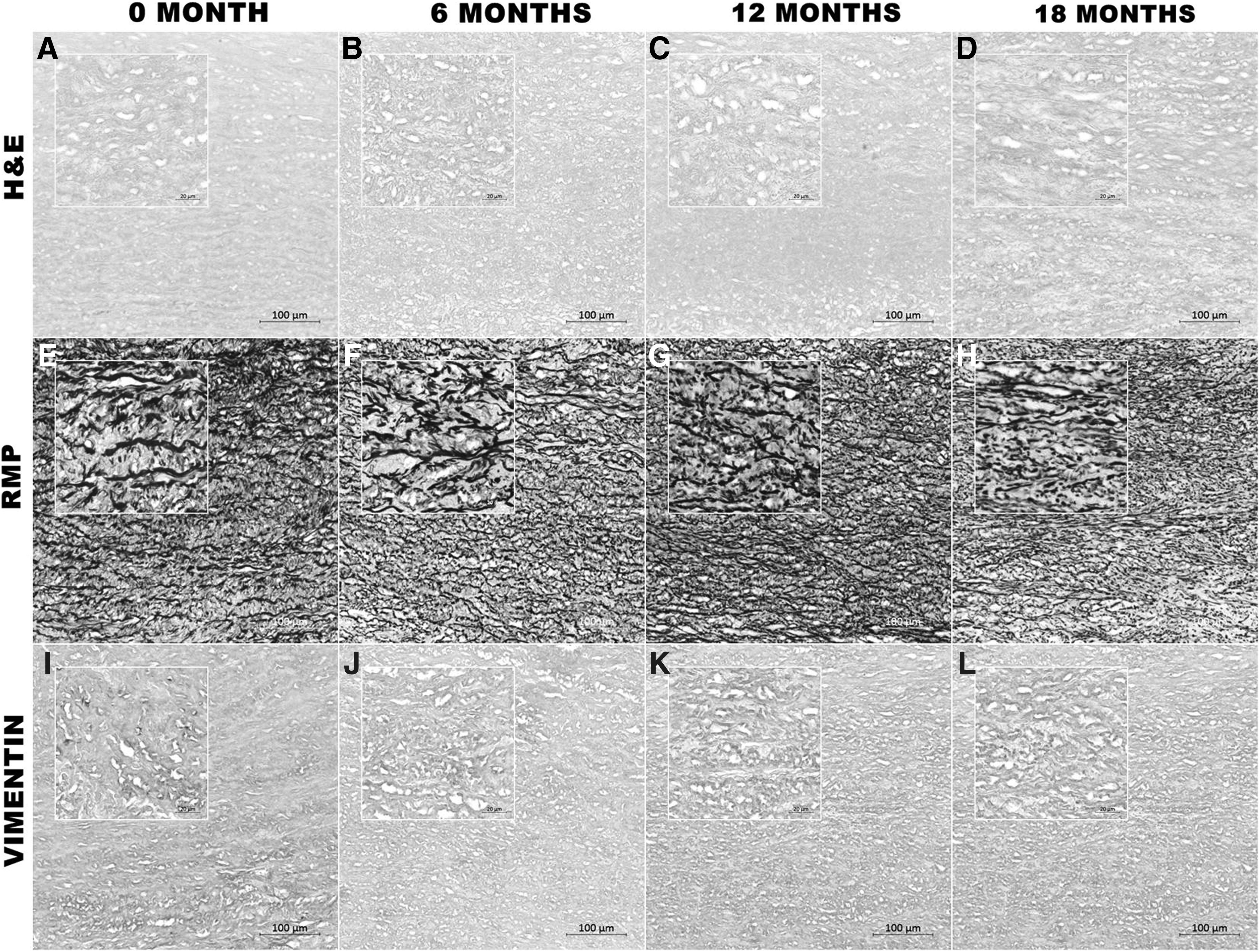
Histological and IHC analyses of decellularized aortic conduits. Representative hematoxylin and eosin and Russell-Movat pentachrome-stained sections did not present obvious deleterious effects or signs of autolysis in the structure of the extracellular matrix due to the preservation method for decellularized aortic valves stored for 6 months

Histological and IHC analyses of decellularized aortic leaflets. Representative hematoxylin and eosin- and Russell-Movat pentachrome-stained sections did not present obvious deleterious effects or signs of autolysis in the structure of the extracellular matrix due to the preservation method for decellularized aortic valves stored for 6 months
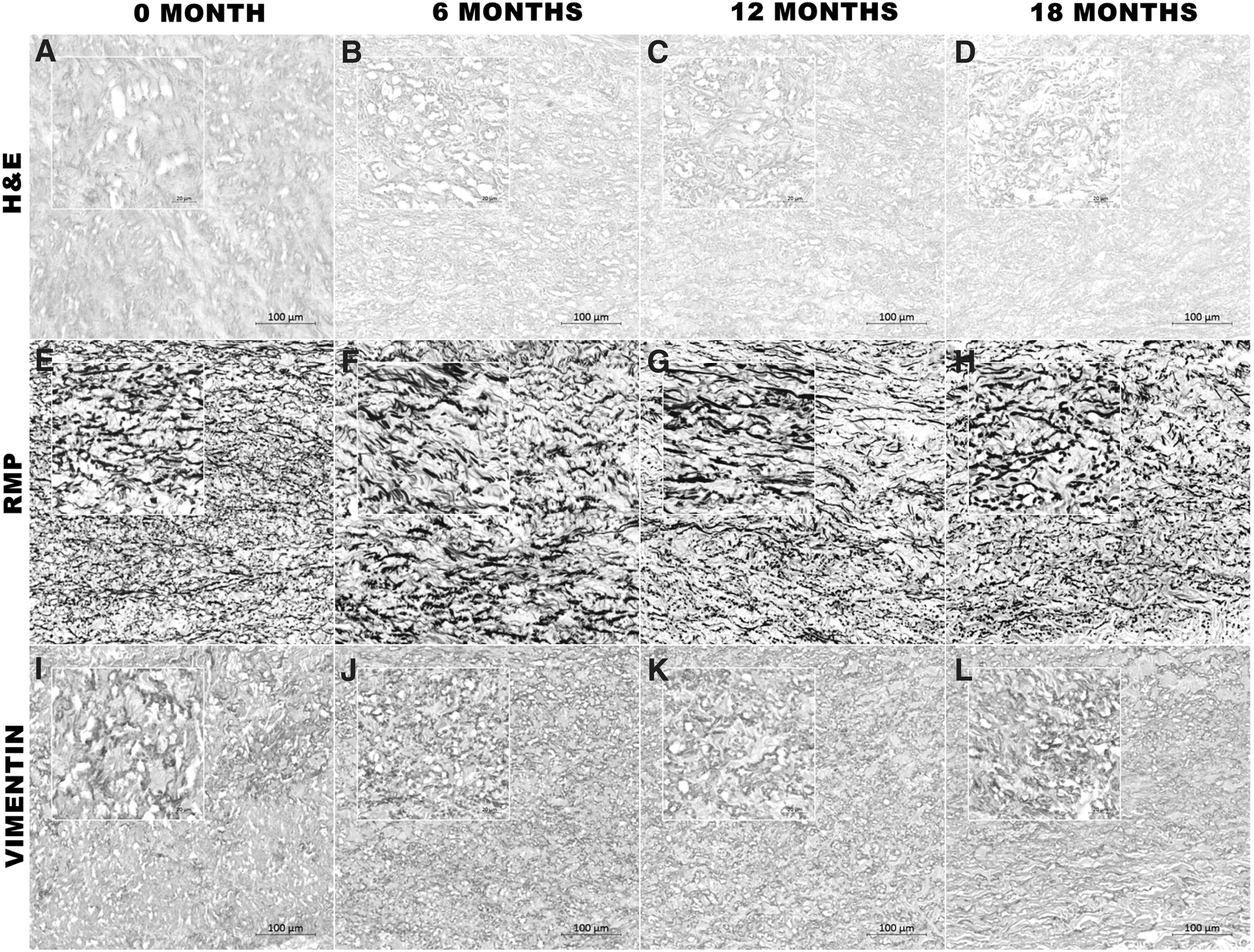
Histological and IHC analyses of decellularized pulmonary conduits. Representative hematoxylin and eosin- and Russell-Movat pentachrome-stained sections did not present obvious deleterious effects or signs of autolysis in the structure of the extracellular matrix due to the preservation method for decellularized pulmonary valves stored for 6 months
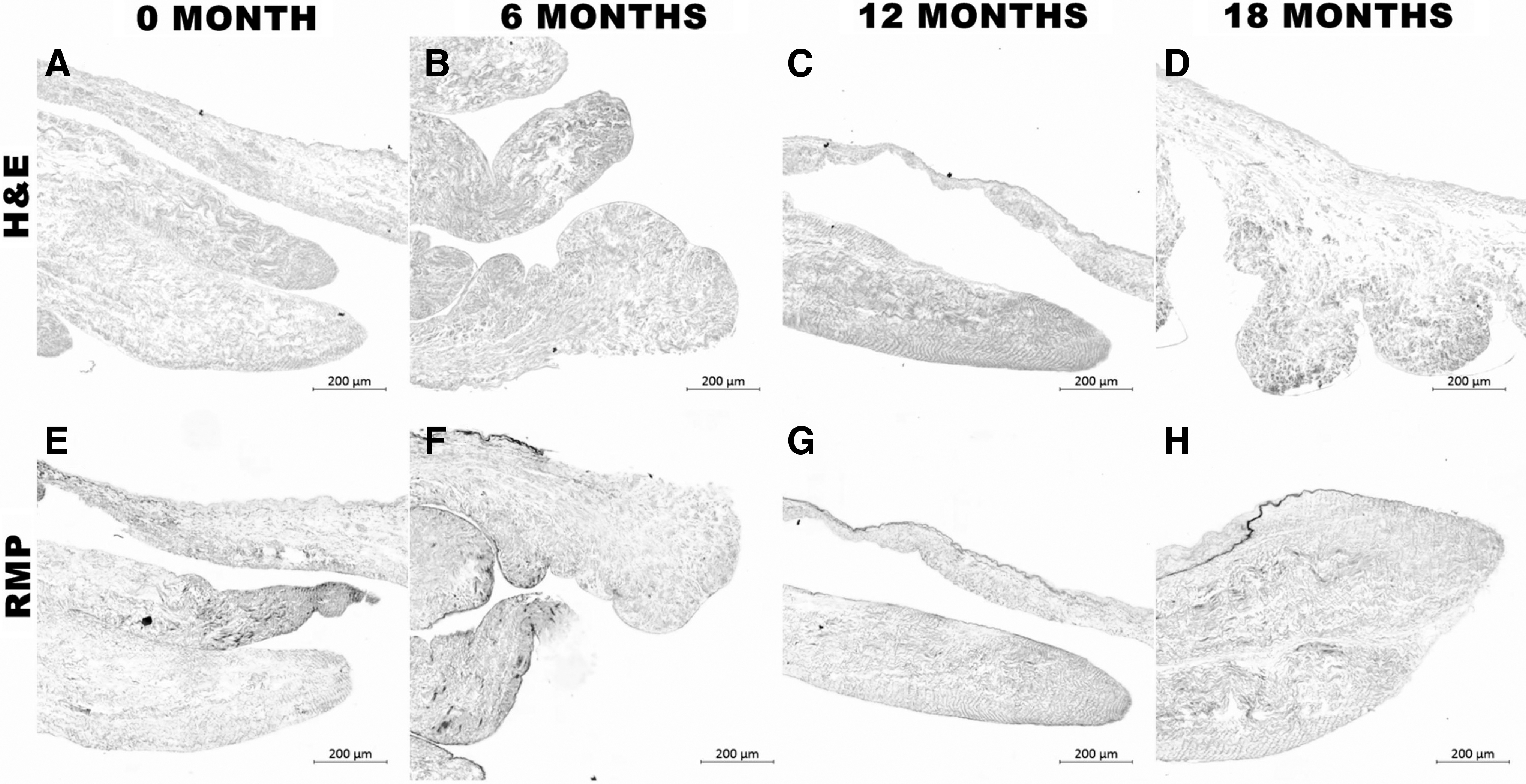
Histological and IHC analyses of decellularized pulmonary leaflets. Representative hematoxylin and eosin- and Russell-Movat pentachrome-stained sections did not present obvious deleterious effects or signs of autolysis in the structure of the extracellular matrix due to the preservation method for decellularized pulmonary valves stored for 6 months
The results of quantitative morphometric analysis of ECM components in RMP-stained tissues are detailed in Figure 6. Each time point was analyzed in three separate samples, and the area occupied by the particular stained component was quantified. The elastic fibers, collagen, and GAG of decellularized aortic/pulmonary conduits were evaluated, and no difference was detected among different times of storage (0, 6, 12, and 18 months) (Fig. 6).
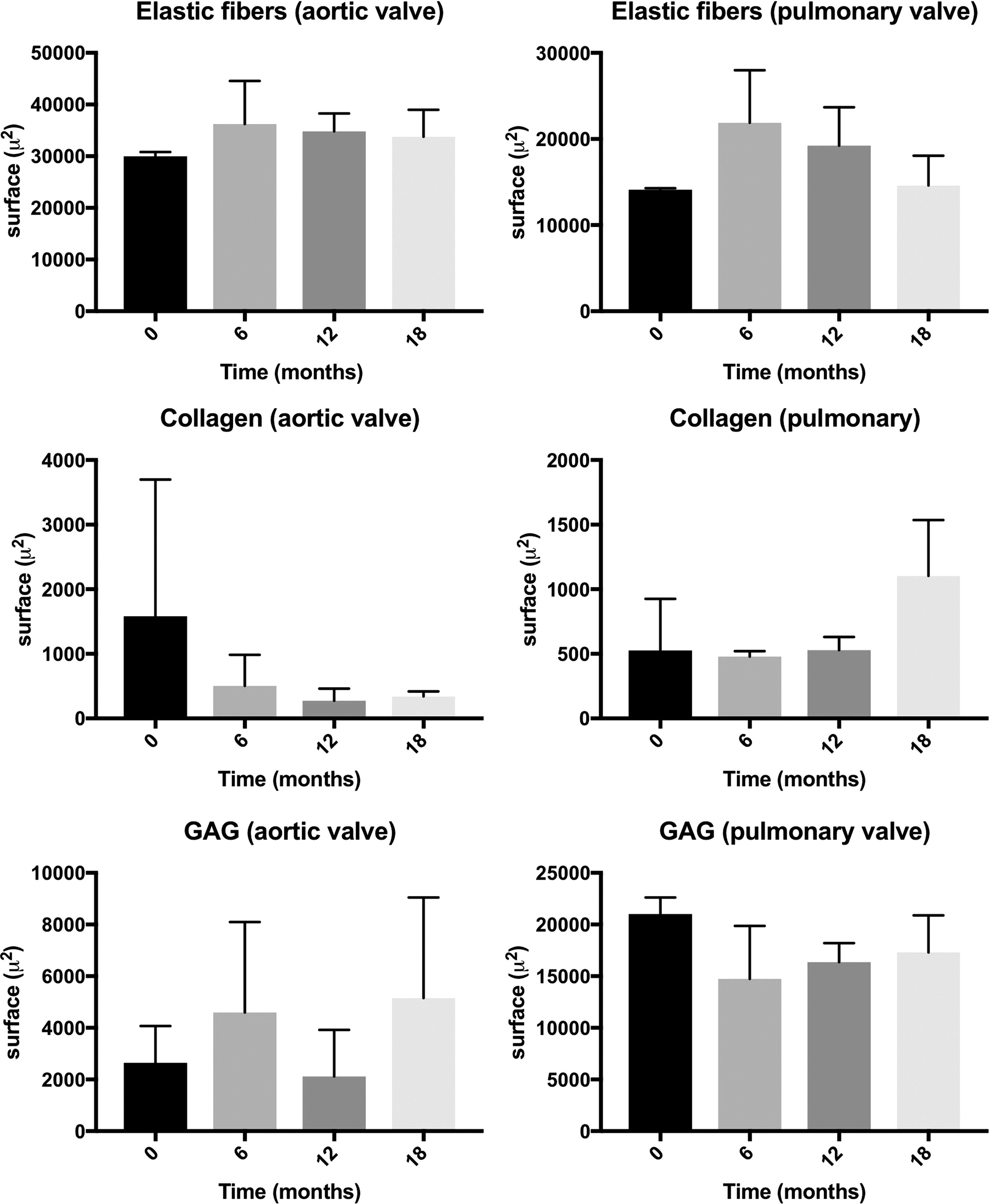
Quantitative morphometric analysis of extracellular matrix components in Russell-Movat pentachrome-stained tissues. The area occupied by the particular stained component was quantified (μm2) according to the entire analyzed field. No difference was detected between tissues analyzed immediately after the decellularization process (0 month) and those stored for 6, 12, and 18 months. GAG, glycosaminoglycan.
Contact cytotoxicity assay
The results of the cytotoxicity tests showed that the fibroblast cells did not present a halo of debris and dead cells around the fragments of human decellularized allografts immediately after the decellularization process (Fig. 7A) and after 6 months (Fig. 7B), 12 months (Fig. 7C), and 18 months (Fig. 7D) of storage, similarly to the negative control (Fig. 7F), suggesting that the material is not cytotoxic to fibroblast cells. In contrast, latex (positive control) caused the formation of a halo due to debris and dead cells (Fig. 7E).
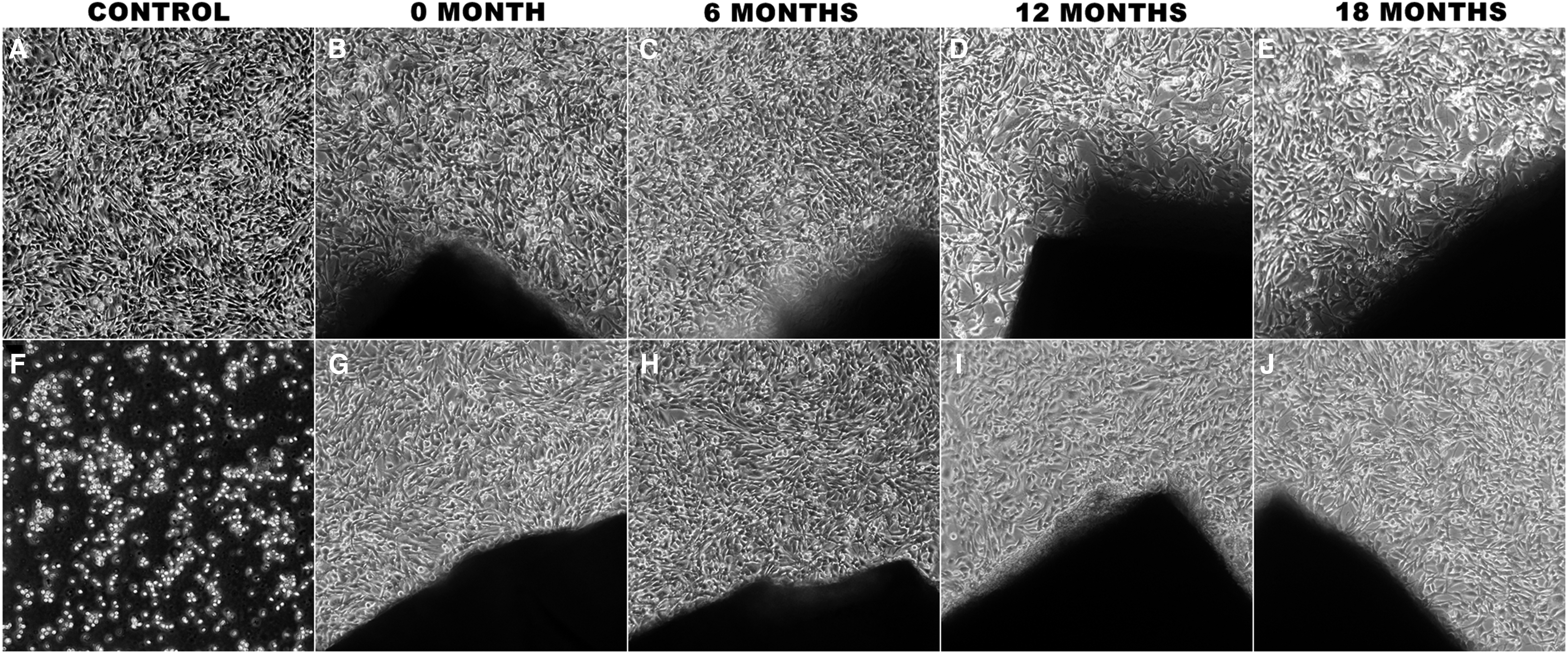
Contact cytotoxicity assay of decellularized aortic and pulmonary allografts. Phase contrast microscopy images showing the morphological appearance of L-929 fibroblasts cells after 48 hours in culture growing in contact with decellularized aortic and pulmonary allografts. Negative control - no tissue in culture (
Biomechanical assay
The properties of tensile strength, elongation, and elastic modulus of the decellularized aortic (Fig. 8) and pulmonary (Fig. 9) valves are presented as column scatter plot graphs showing the mean and standard deviation. The difference between the mean of groups is detailed in each graph for all properties.

Graphical representation of the mechanical parameters obtained for decellularized aortic valves immediately after the decellularization process (0 month) and after storage for 6, 12, and 18 months: tensile strength (MPa) of the aortic conduit
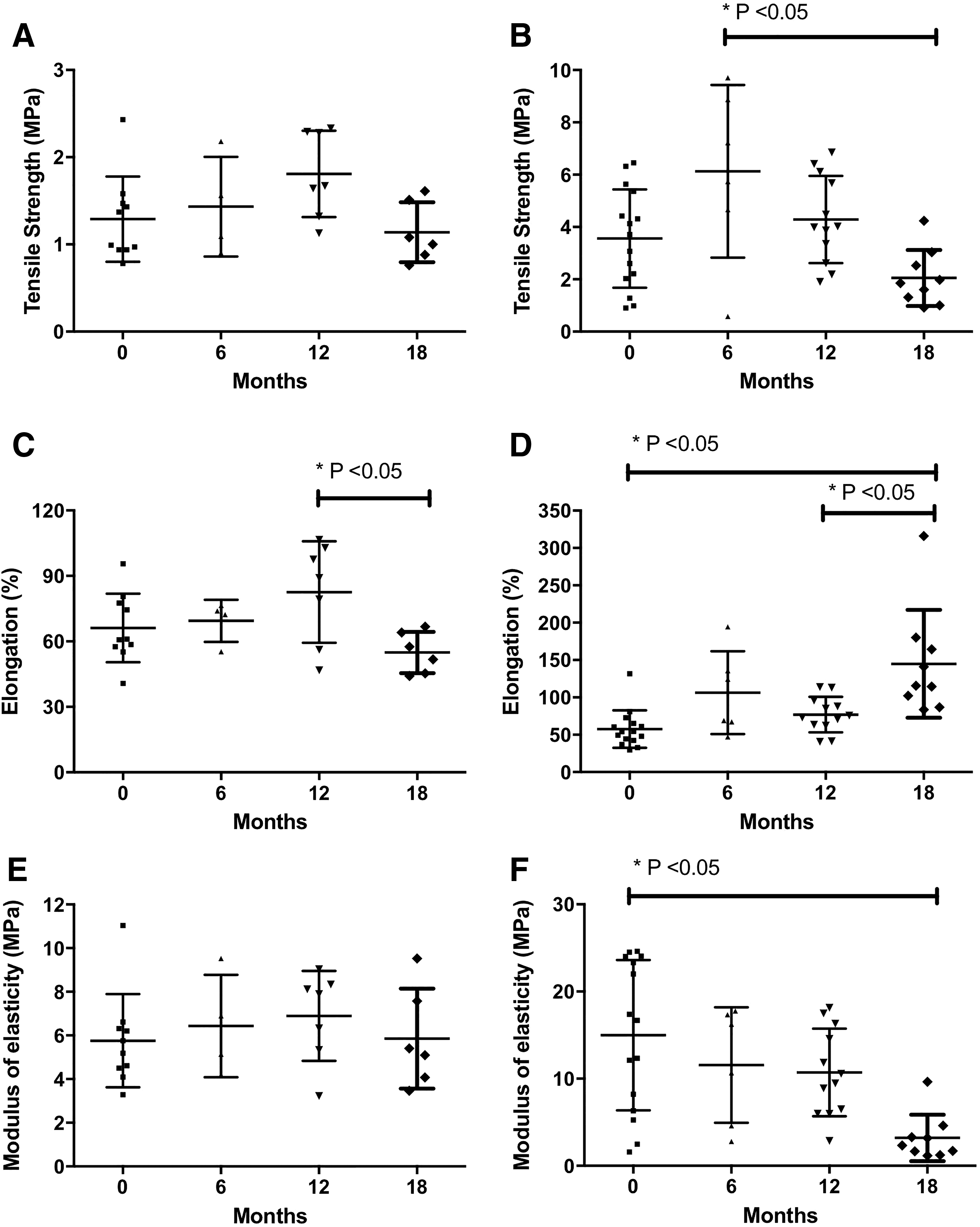
Graphical representation of the mechanical parameters obtained for decellularized pulmonary valves immediately after the decellularization process (0 month) and after storage for 6, 12, and 18 months: tensile strength (MPa) of the pulmonary conduit
Discussion
In this study, we present data demonstrating that hypothermic preservation of decellularized allografts in 0.9% NaCl up to 12 months did not damage the allograft structure and functionality. Preservation of decellularized allografts after 12 months showed significant alterations in biomechanical assays, suggesting that function of the valve can be prejudiced.
The current knowledge on the storage of decellularized allografts and the evaluation of their quality during storage is limited. 21 Preservation of allograft valves is the most important determinant of their durability. 41 Several preservation methods have been developed, including hypothermic preservation, cryopreservation, and vitrification. According to Han and Bischof, cryopreservation and vitrification use cooling to very low temperatures in the presence of high concentrations of cryoprotective chemical agents for preserving tissues. 42 Although these cryogenic techniques provide longer preservation time than hypothermic preservation, they can induce freezing injuries in tissue because of ice formation within cellular or extracellular spaces, and/or by the addition and removal of high concentrations of cryoprotective chemical agents. 42
Proper storage of processed tissue is the key to a successful tissue transplant. 43 In the present study, we demonstrated that the time and temperature of storage did not have a significant effect on the pH of the stock solution maintained up to 18 months. The pH of the storage solution is a critical parameter; furthermore, the stability of most proteins is pH dependent. 44 The pH of the stock solution did not change significantly during 0, 6, 12, and 18 months of storage when compared with the initial pH value of 5.8. There are three basic factors that affect the pH of a commercial saline solution: atmosphere, ions in solution, and container. 39 During storage, many environmental factors influence the stability of bioproducts41,45; therefore, care should be taken to prevent mix-ups, contamination, and cross-contamination of tissues, supplies, and reagents. Moreover, our method of processing and storage had a low risk of microbial infection and a low cost. After the disinfection process, the cultures were negative until 18 months. Microbiological suitability tests confirmed the absence of residual antibiotics even at 18 months of storage.
Many factors, such as the harvesting method, preservation protocol, implantation technique, or patient selection process, are controversially discussed in terms of their influence on allograft durability after implantation.42,46 The fresh-wet method of storage of unprocessed allograft valves has some disadvantages such as increasing calcium content, and decreasing the phosphate content, thus accelerating the calcification process. These effects limit the age of donors to 40 years, and medium 199, which is commonly used in fresh-wet storage procedures, needs to be modified. 34 Moreover, refrigerated storage of heart valve leaflets causes rapid deterioration of the synthetic capabilities of fibroblast protein in 2 weeks. 32 Chow and Zhang reported a decrease of insoluble and total collagen in bovine thoracic aortas that had been stored at common storage temperatures (4°C, −20°C, or −80°C) at three different time points (48 hours, 1 week, or 3 weeks). 47 After 48 hours of storage, salt-soluble collagen decreased in all storage methods. This was expected as salt-soluble collagen is the most easily degraded of the three types of soluble collagen. The reason why the salt-soluble collagen levels returned to values similar to those of fresh samples after 1 and 3 weeks of storage was not clear. 47 On the contrary, Waterman and Adami 45 demonstrated that fresh allograft valves stored in medium 199 containing extremely small doses of penicillin at 4°C up to 60 days showed good long-term results, with 97% of patients aged 30 years or older remaining free from valve degeneration after 10 years. 48 The temperature of preservation can also influence the final pH of the solution, decreasing pH in room temperature when compared with refrigerated allographs. 49
The aortic and pulmonary decellularized allografts showed a very similar histologic structure across different times of storage. It is known that any decellularization process causes a certain degree of ECM denaturation. 15 The observed ECM changes in our study were related to the decellularization process rather than to storage.
Histological analysis showed that decellularized allografts stained with H&E and RMP did not present obvious deleterious effects or signs of autolysis in the structure of the ECM due to the preservation method. Histological and IHC analyses revealed few differences in the structure of the conduits that could be related to the time of storage. There were no significant differences in morphological aspects, antigenic viewpoint, and dye affinity among the different storage times analyzed. Overall, nuclear material and cytoplasmic elements were absent, although cytoskeletal remains were maintained after decellularization.
In the current study, no difference in vimentin expression related to storage time was identified. The presence of intermediate filaments (vimentin) after the decellularization process may mean that there were cytoskeletal remains in these decellularized allografts. The fact that we did not find differences in vimentin expression over time means that there was no degeneration of cytoskeletal remains during the preservation process of these allografts. This could, perhaps, be another criterion for preservation. It should be stressed that decellularization methods do not allow for the removal of the total content of the cellular material. The use of immunohistochemistry may not be a good measure of protein integrity. This method evaluates specifics epitopes, but does not evaluate the integrity of the entirety of the protein. 50
As the decellularized heart valves are to be used for surgical purposes, in addition to histological and microbiological analysis, a haptic evaluation was performed. In this study, no change occurred in the tactile perception of decellularized allografts after hypothermic preservation in 0.9% NaCl.
Because tissues are preserved for an in vivo application, their functional properties must also be preserved. These functional properties are tissue dependent and often related to the macroscopic mechanical properties of tissue. 42 Biomechanical characterizations of human native and decellularized heart valves are rare in the literature.51,52 In this study, the tissue biomechanical properties changed over time in different aspects. Allografts stored for 18 months presented lower tensile strength and elasticity. Wang et al. evaluated structure and biomechanical properties of freeze-dried decellularized porcine pulmonary heart valves. 53 These authors demonstrated that the elastic modulus values of freeze-dried tissue stabilized by lyoprotectants were greater than those of decellularized tissue, but similar to those of native tissue. 53 A progressive increase in the percentile elongation of the pulmonary leaflet was observed over time, but without statistical significance (Fig. 7D). In heart valves, like in many tissues, collagens are the main structural proteins responsible for structural integrity and biomechanical strength, predominantly tensile strength. 54 It has been proved that the frequently used decellularization agents may disrupt the collagen structure in decellularized tissues, thus decreasing the mechanical strength of the obtained ECM scaffold. It has also been shown that most detergents cause at least some removal of GAGs from the scaffold, an effect that has varying degrees of negative impact on the viscoelastic characteristics of the scaffold. 55 Collagen and elastin play important roles in maintaining the mechanical properties of the ECM. 56
This study has several limitations. The tissues stored for 6, 12, and 18 months were obtained from the same donor; however, the tissues analyzed immediately after decellularization were obtained from a different donor. The biomechanical assay and histological analysis were performed in valves from different donors. Although the microbiological suitability tests were performed according to the United States Pharmacopeia criteria, we believe that a high-performance method for detecting residual antibiotics, such as high-performance liquid chromatography or mass spectroscopy, would offer more safety data. Furthermore, these tests could detect residues from decellularization, such as SDS and EDTA, which could be associated with degeneration of ECM with longer storage. The morphometric analysis was performed in only three donors for each time and valve. This number limits the statistical analyses. The decellularization protocol itself is a limitation. It is possible that other decellularization protocol could give different results, and the variability also occurred in our decellularization protocol.
The decellularized allografts produced in our tissue bank were hypothermically preserved in 0.9% NaCl up to 6 months. Taken together, the results obtained in this study suggest that decellularized allografts can be successfully preserved for up to 12 months without loss of structure and functionality. Further studies should be conducted to understand the full potential of decellularized allografts to improve their stability and clinical applications.
Footnotes
Acknowledgment
We are grateful to Cesar Augusto Oleinik Luzia for biomechanical tests.
Author Disclosure Statement
No conflicting financial interests exist.
Funding Information
This work was supported by the Brazilian Ministry of Health (FNS 814611/2014).