
Abstract
Purpose:
The quality of specimens directly affects the experimental results. The stability and structural integrity of nucleic acids in samples have a decisive influence on high-throughput sequencing results. Next-generation sequencing (NGS) provides the most comprehensive criteria for evaluating the specimen quality. To test the quality of cell-free DNA (cfDNA) from lung cancer plasma samples stored in our biobank, we conducted a study to evaluate the quality in terms of the genetic level.
Methods:
A total of 189 peripheral blood samples were collected from patients from patients with EGFR-positive nonsmall cell lung cancer who were seen and treated in Jilin Provincial Cancer Hospital from August 2012 to March 2018. Twelve milliliters of peripheral blood samples were collected and centrifuged at 4°C, 2000 rpm for 15 minutes. Plasma samples were dispensed into cryotubes and stored at −80°C. Plasma cfDNA was extracted by a DNA extraction kit (Qiagen) and the DNA concentration was detected by a Qubit 3.0 fluorometer.
Results:
The total volume of cfDNA extraction at baseline was 50 μL, the median concentration according to Qubit was 0.633 ng/μL, the range was 0.331–6.09 ng/μL, and the median total DNA was 34.25 ng, ranging from 20.35 to 304.5 ng. The median value of the Qubit concentration in advanced plasma samples was 0.838 ng/μL, ranging from 0.24 to 21.9 ng/μL, and median total DNA was 41.9 ng, ranging from 12.0 to 1095.0 ng. Based on the aforementioned quality assessment factors, 4 of 189 frozen lung cancer baseline plasma samples were not included in further analyses, and for the remaining 185 cases of cfDNA >20 ng, the pass rate was 97.9%. In 143 frozen lung cancer advanced stage plasma samples, 133 cases of cfDNA >20 ng, the pass rate was 93%.
Conclusion:
Frozen lung cancer plasma samples stored in the biobank for 1–6 years at −80°C under certain conditions still retain a high level of cfDNA, which is suitable for NGS detection.
Introduction
Lung cancer is the leading cause of cancer-related deaths worldwide. 1 Nonsmall cell lung cancer (NSCLC), which accounts for 85% of lung cancer cases, is the most common cause of cancer deaths. 2 Tumor specimens play an important role in promoting the progress of cancer research and have become the basis of cancer research studies. The quality of the specimens directly affects the experimental results. With the widespread use of next-generation sequencing (NGS), a more precise method of specimen quality control is needed. NGS can simultaneously sequence multiple target genomes from multiple samples. Compared with Sanger sequencing, NGS sequencing requires a small amount of starting DNA/RNA specimens, which provides a strong technical guarantee for multigene detection of circulating cell-free DNA (cfDNA).
cfDNA refers to trace amounts of endogenous and heterologous DNA fragments that are present in the blood circulation and that are free of cellular material. In 1977, Leon et al. found that the free DNA content in peripheral blood of cancer patients was significantly higher than that in healthy people, 3 suggesting that it may be closely related to the occurrence of cancer. The specific mechanism of cfDNA release is not clear; Wyllie proposed that tumor cells release short double-stranded DNA fragments into the blood when undergoing apoptosis or cell necrosis. 4
With the advent of precision medicine and individualized treatment, disease progression, drug efficacy, and clonal evolution can be monitored through detecting cfDNA in peripheral blood, because it includes genomic information on the patient's primary tumor and metastases. Thompson et al. and Schwaederlé et al.'s studies showed the feasibility of using NGS technology to analyze gene mutations in NSCLC patient's plasma cfDNA.5,6 A liquid biopsy with cfDNA in peripheral blood is easier to obtain than tissue specimens and can avoid the limitation of tumor heterogeneity.
Epidermal growth factor receptor (EGFR) mutation is the most commonly detected type of mutation in NSCLC and is present in 10%–40% of cases.7,8 Patients with EGFR-sensitive mutations are generally highly responsive to first-generation tyrosine kinase inhibitors (TKIs), but most patients will develop resistance within 12–24 months of treatment initiation.9–11 Primary and acquired resistance mechanisms for EGFR-TKI treatment, including amplification of MET and ERBB2, deletion or point mutation of EGFR, Kirsten rat sarcoma viral oncogene homolog (KRAS); v-raf murine sarcoma viral oncogene homolog B (BRAF); and PIK3CA, and deletion or inactivation of phosphatase and tensin homolog (PTEN).12,13
Collecting and preserving baseline and advanced peripheral blood samples from patients with EGFR-positive and EGFR-TKI-targeted NSCLC patients is helpful to further explore the molecular resistance mechanism of NSCLC. Biobanking plays an important role in the long-term preservation of biological samples. It is generally accepted that tissue specimens preserve their integrity for long periods of time at low temperature. Kelly et al. 14 showed that frozen tissue samples stored in gas–liquid nitrogen (about −180°C) for 2–11 years had no time-dependent reduction in DNA and RNA integrity coefficients, and the quality of tissue samples was maintained at a high level. Whether plasma samples stored at −80°C for 1–6 years can be used for NGS testing has not been reported.
The aim of this study was to determine the concentration and content of cfDNA in plasma samples from NSCLC stored in our biobank and to evaluate whether it is suitable for NGS detection.
Materials and Methods
Blood collection and plasma separation
Peripheral blood samples (with EDTA-K2 anticoagulant) were collected from patients with EGFR-positive NSCLC who were admitted to the Jilin Provincial Cancer Hospital from August 2012 to March 2018. Blood was centrifuged at 2000 rpm for 15 minutes at 4°C. The plasma and leukocyte layers were separated into 1.5 mL cryotubes, respectively, and then stored at −80°C, until analysis. The study was approved by the Ethics Committee of our hospital and all patients received informed consent.
cfDNA extraction
The cfDNA in plasma samples was extracted using the QIAamp Circulating Nucleic Acid Kit (Qiagen). The extracted cfDNA was quantified with Qubit 3.0 (Invitrogen) and stored in −20°C for the next library construction.
Statistical analysis
Data distribution was determined by the Kolmogorov–Smirnov (K–S) test, which was used to determine whether the data had a normal or non-normal distribution. Normal and non-normal distributed data were expressed as the mean ± standard deviation and (P25, P75), respectively. The Kruskal–Wallis test was used for significance of differences among data with non-normal distributions.
Results
The amount of cfDNA was extracted from the plasma of baseline patients. The volume of cfDNA extracted from plasma in 189 patients with baseline NSCLC was 50 μL, the median concentration using Qubit was 0.633 ng/μL, the range was 0.331–6.09 ng/μL, and the median total cfDNA extraction was 34.25 ng, range 20.35–304.5 ng. The amount of cfDNA extracted from patients at baseline was as shown in Figure 1. In 189 frozen baseline plasma samples, 4 samples had a cfDNA content of 10–20 ng, and these samples were not included in further analyses. The remaining 185 plasma samples with cfDNA extraction amount >20 ng were used for the next library construction, and the pass rate was 97.9%.
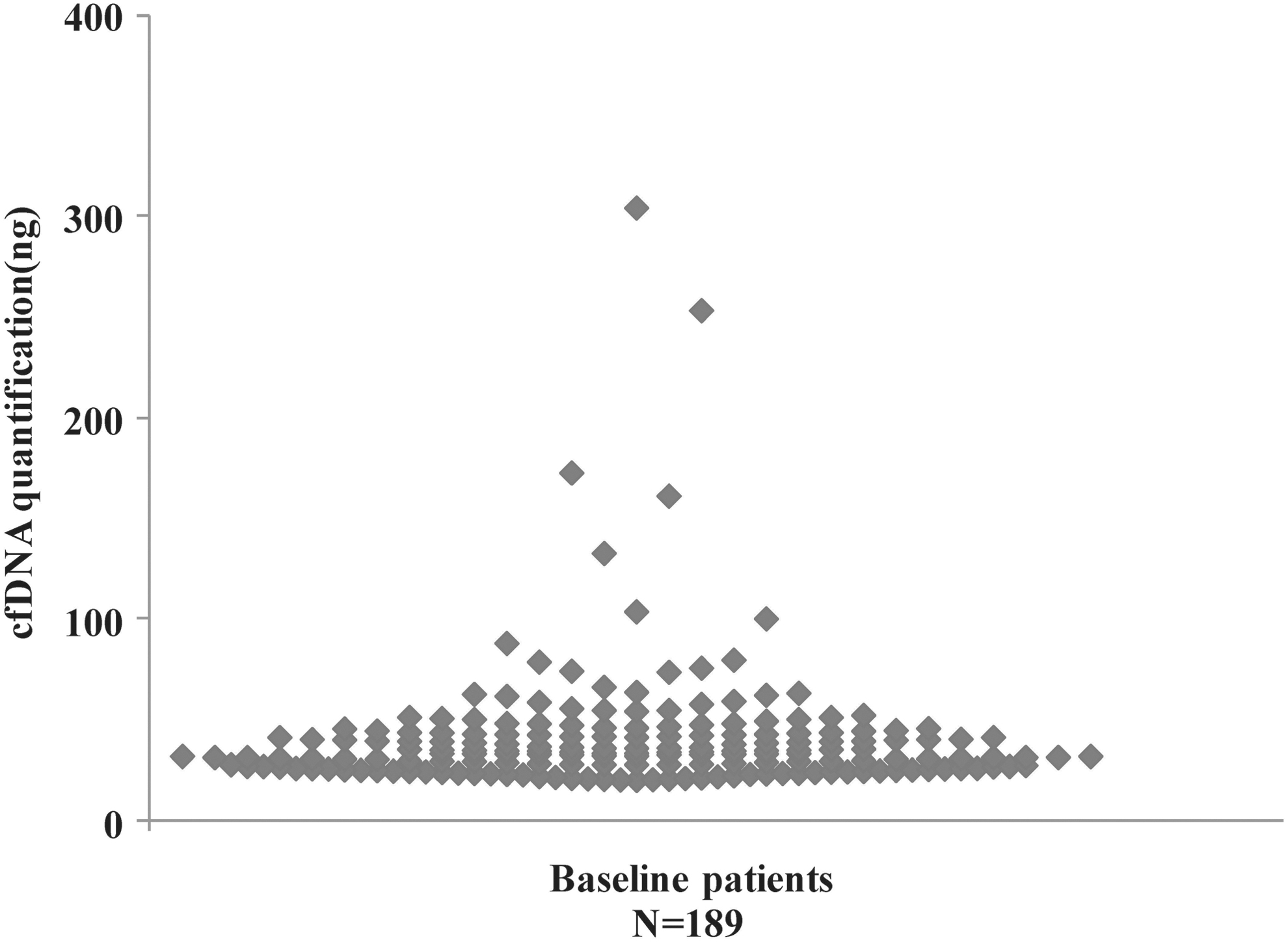
The amount of cfDNA extracted from patients with baseline NSCLC (N = 189). cfDNA, cell-free DNA; NSCLC, nonsmall cell lung cancer.
Amount of cfDNA extracted from plasma in patients with advanced NSCLC
The volume of cfDNA extracted from plasma in 143 patients with baseline NSCLC was 50 μL, the median concentration using Qubit was 0.838 ng/μL, the range was 0.24–21.9 ng/μL, and the median total DNA was 41.9 ng, ranging from 12.0 to 1095.0 ng. The amount of cfDNA extracted from patients with advanced disease is shown in Figure 2. The cfDNA extraction of 10 samples was 10–20 ng and these samples were not included in further analyses. The cfDNA extraction of 133 plasma samples was >20 ng, which could be used for the next step of library construction, with the pass rate of 93%.

The amount of cfDNA extracted from patients with advanced NSCLC (N = 143).
Annual distribution of cfDNA extraction and concentration mean value in NSCLC patient's plasma
The cfDNA extraction concentration in 2012, 2013, 2014, and 2018 were 1.079 ± 0.867, 1.131 ± 1.250, 0.749 ± 0.378, and 1.246 ± 0.648 ng/μL, respectively, and the data were normally distributed. The cfDNA extraction concentrations in 2015, 2016, and 2017 were (0.515, 1.100), (0.541, 0.974), and (0.514, 1.133) ng/μL, respectively. Data were non-normally distributed. There was no significant difference between the plasma cfDNA extraction concentration with respect to the storage year, p = 0.375.
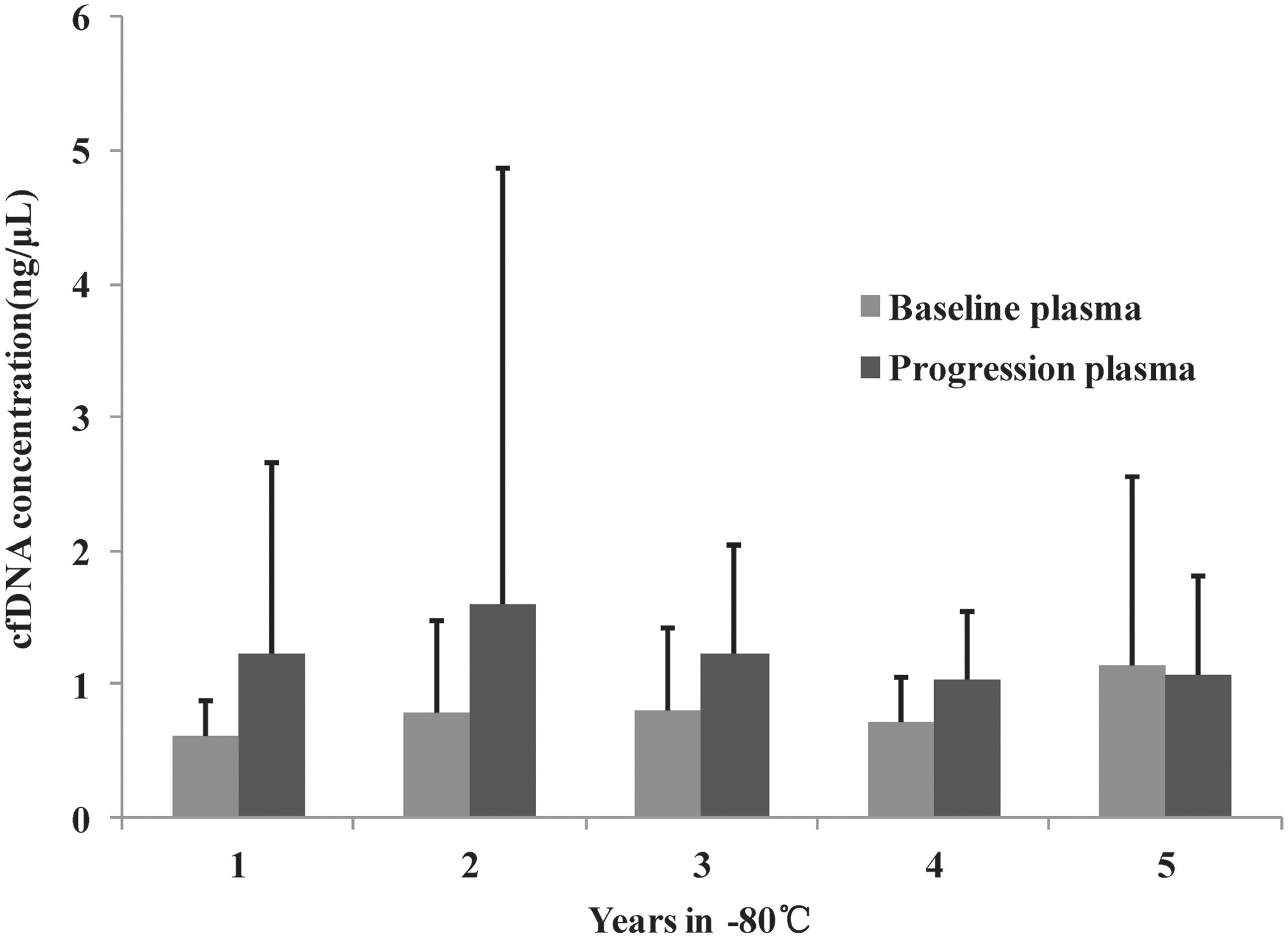
A small number of total samples and uneven distribution of sample numbers in each storage period existed in the retrospective study. After excluding 5 and 6 years of sample data with a small sample size, we used the Kruskal–Wallis test to analyze the effect of storage time (1–4 years) on cfDNA extraction concentration of the samples. We observed that the cfDNA extraction concentration showed a downward trend with the increase of storage time, p = 0.676. The graph of cfDNA concentration over storage time is shown in Figure 3.

cfDNA concentration of each storage period.
Mean value of plasma cfDNA concentration in baseline and advanced phase of NSCLC patients
As shown in Figure 4, at the baseline phase in 2013, 10 patients had a mean cfDNA concentration of 1.148 ng/μL. In the baseline phase of 2014, 31 patients had a mean cfDNA concentration of 0.71 ng/μL. In the baseline phase of 2015, 46 patients had a mean cfDNA concentration of 0.807 ng/μL. In the baseline phase of 2016, 75 patients had a mean cfDNA concentration of 0.796 ng/μL. In 2017, 21 patients had a mean cfDNA concentration of 0.619 ng/μL. In 2013, the advanced stage, there were three cases with a mean cfDNA concentration of 1.075 ng/μL; in 2014, four cases had a cfDNA concentration of 1.044 ng/μL. In 2015, 29 cases had a cfDNA concentration of 1.232 ng/μL. In 2016, in the advanced stage, 43 patients had a mean cfDNA concentration of 1.605 ng/μL, and in 2017, 57 patients had a mean cfDNA concentration of 1.224 ng/μL.
Mean value of plasma cfDNA concentration in baseline and advanced phase of each year.
Discussion
This study retrospectively analyzed the feasibility of plasma cfDNA for NGS stored at −80°C, and detected the concentration of cfDNA and the total amount of cfDNA before NGS sequencing. In the EGFR-positive patients with advanced NSCLC, for 12 mL of peripheral blood samples, the median total cfDNA at baseline was 34.25 ng, ranging from 20.35 to 304.5 ng. The median total cfDNA was 41.9 ng, ranging from 12.0 to 1095.0 ng, which was higher than the baseline. It has not been found that long-term storage at −80°C affects plasma cfDNA.
With the gradual improvement of biospecimen science and biobanks, there will be an increased demand for high-quality biological specimens. During clinical studies, the specimen quality dictates the reliability of results. At present, the methods for clinically detecting cfDNA include capillary electrophoresis, droplet digital polymerase chain reaction (ddPCR), NGS, and the peripheral blood volume collected for cfDNA is 10 mL. The commonly used blood collection tube is an EDTA anticoagulation tube. The blood is processed within 4 hours for centrifugation, and the plasma extracted cfDNA construction library is collected. 15 According to Liu et al., 16 the proportion of cfDNA extracted from 10 mL of peripheral blood in patients with colorectal cancer is ∼80%. Similar to our findings, the amount of cfDNA extracted from 12 mL of peripheral blood in patients with advanced NSCLC was >20 ng, accounting for >90%. Streleckiene et al. 17 found that different cfDNA extraction kits and freeze–thaw cycles will affect the amount of cfDNA. The degree of hemolysis significantly affected the amount of genomic DNA (gDNA) extraction, but it had no obvious effect on the amount of cfDNA extraction. Compared with fresh plasma samples, the amount of cfDNA extracted by QIAamp Kit from plasma samples once frozen and thawed was significantly higher (2.46 ± 0.61 ng/mL vs. 3.15 ± 0.55 ng/mL, p = 0.016). Similarly, the amount of cfDNA in plasma subjected to two freeze–thaw cycles also increased significantly (2.46 ± 0.61 ng/mL vs. 3.11 ± 0.63 ng/mL, p = 0.031). Two other kits, MagMAX and dNextPrep-Mag, were not affected by the number of freeze–thaw cycles. In our study, plasma samples involved one freeze–thaw cycle, and since there was no comparison with fresh plasma samples, no data were available on the effect of freeze–thaw cycles on cfDNA extraction. However, our study retrospectively analyzed plasma samples obtained from 12 mL of peripheral venous blood stored at −80°C for 1–6 years, and 95.6% (318/332) of cfDNA >20 ng was obtained, which provided an important reference for long-term storage of plasma samples. Fernando analyzed human blood cell-free plasma, exosome, and apoptotic body DNA fragment sizes by chemistry-based ddPCR assays that demonstrated the existence of a unique fragment size distribution pattern for both cell-free plasma and exosome DNA fractions. 18
With the emergence of targeted therapies for NSCLC, real-time tumor genotyping is required for patients to guide clinical treatment. However, the patient's tumor tissue is often difficult to obtain, or the resulting tissue produces insufficient DNA for NGS sequencing, and it was rare to have a continuous biopsy. Aggarwal et al. used NGS to evaluate plasma genotyping in the treatment of metastatic NSCLC. 19 In the sample of only 101 plasma NGS analysis, 79 (78.2%) DNA yield or quality did not meet the sequencing criteria. From 207 tissue specimens tested for NGS, 79 specimens were insufficient for DNA quality and quality and did not meet sequencing requirements (38.2%). To assess whether disease staging affects the detection rate of mutant genes, Aggarwal et al. analyzed mutations in tissue and plasma samples from patients with metastatic nonsmall cell carcinoma, and 13 patients with M1a (intrathoracic) metastasis, 19 NGS detected mutations in the tissue specimens of seven patients with a detection rate of 53.8%, but no mutant gene was detected in the plasma specimens. In 42 patients with M1b (thoracic surgery), 8 cases of plasma NGS mutations were detected, and the detection rate was 19.0%. In another 13 patients with liver metastases, the detection rate of plasma NGS mutations was 100%. It is speculated that the detection rate of NGS mutation in peripheral blood cfDNA is related to the tumor metastasis site. However, only the concentration and amount of plasma cfDNA before NGS sequencing were presented. In this study, and there was no limitation in the presence of NGS sequencing results and the lack of mutation information in tumor samples had certain limitations.
At present, cfDNA is still facing many challenges in clinical application, such as sample collection time, collection process, storage conditions, cfDNA extraction, the analysis platform, and the interpretation of the results will have different degrees of impact on the test results. In summary, for the cfDNA extraction and detection of plasma specimens stored in −80°C for 1–6 years, the amount of cfDNA suitable for NGS sequencing was successfully extracted, indicating that plasma specimens with a storage time of 6 years at −80°C are feasible for NGS testing.
Footnotes
Author Disclosure Statement
No conflicting financial interests exist.
Funding Information
This research was funded by the Department of Science and Technology of Jilin Province (20170622005JC) and Scientific Research Funds of Jilin Province of Health and Family Planning Commission (2017J023 and 2018Q007).