
Abstract
Introduction:
In Italy, the transport of cryopreserved biological material is controlled by several Decrees (Legislative Decree No. 191/2007 and No. 16/2010 and Health Ministry's Decree of October 10, 2012). Given the nature of their applications, the transport of reproductive cells has peculiar quality and safety requirements that must be applied universally, minimizing the chance of error. To standardize the cross-border shipping procedure to meet the quality, traceability, and safety criteria for cells and tissues, it is appropriate to establish a unified process using the same tools, forms, and communication channels.
Methods:
A working group has been created by SIERR. This “FOCUS Group” was constituted by representatives from Italian-assisted reproductive technology centers and sperm banks who worked together to define joint procedural steps and create specific forms to support the movement of cryopreserved samples.
Results:
The FOCUS Group identified the critical steps in the communication procedures between Italian centers and created the related forms: patient authorization, request from the recipient center, critical checks carried out by both sending and recipient centers, start of samples transfer, collection, transport and taking responsibility of the biological material, acknowledgment of samples arrival, and acknowledgement of any adverse event that occurred.
Discussion:
Indications on shipping between tissue institutions and legal responsibilities are important points and a working protocol with shared transport forms has been defined. Standard Operating Procedures are necessary in light of the increasingly widespread movement of biological samples between the various countries, and represent a valid means of support for the patients who could have a higher awareness of safety and traceability during each stage of gamete transport.
Introduction
Treatment of an infertile couple frequently requires the use of assisted reproductive technology (ART) involving cryopreserved biological materials, gametes, and embryos. The cryopreservation of reproductive cells (gametes, embryos) and ovarian or testicular tissues is carried out in tissue establishments. These fall into two types: tissue banks dedicated to preserving the fertility of patients requiring potentially sterilizing treatments and facilities inside fertility centers, where the cryopreserved material may subsequently be used. Tissue establishments are thus able to preserve such biological products, ensuring high standards of long-term storage. The cryopreserved materials are of course precious for all patients who undergo ART, but are even more important for cancer patients, who have undergone potentially gonadotoxic surgical and/or pharmacological treatments and may have no other reproductive choice.
In clinical practice, couples often need to transfer cryopreserved biological samples from a sperm/egg bank to a fertility center. Such transfers may be within the same country or across borders, and demand particular attention, given the intrinsic value of these materials. Awareness of applicable regulations and of packaging and transport considerations is necessary. 1 The transport of these materials must also take into account that the samples are preserved in liquid nitrogen at −196°C, which can be extremely dangerous.
The cryopreservation of gametes and embryos is now an essential tool in the treatment of couple infertility. As in other fields of medicine, there is a need to develop a common set of rules for the cryobiology sector, with standardization not only of the technical aspects, which are now widely known, but also of the biological and regulatory aspects. The legislative provisions on transfers between tissue banks and fertility centers and the recognition of the responsibilities that such transfers entail are key points to be elaborated, elucidated, and agreed upon between the various establishments involved in cell and embryo management. Furthermore, given the nature of their applications, the distribution of reproductive cells entails particular safety and quality requirements that must be applied universally to reduce or, preferably, eliminate any possibility of error. Such distribution should be standardized through the establishment of a unified process using the same standard operating procedures, forms, and communication channels to achieve the required quality, traceability, and safety standards for cells and tissues. The aim of the SIERR Focus Group was to establish a safe Standard Operating Procedure for National use, given the increasing frequency of transfers of biological samples between different centers.
Methods
A working group has been created by SIERR. This “FOCUS Group” was constituted by representatives from Italian ART centers and sperm banks who worked together to define joint procedural steps and create specific forms to support movement of cryopreserved samples.
Results and Discussion
Sperm cryopreservation
Medical and surgical treatments, although essential for patients with neoplastic or autoimmune diseases, can lead to transient or permanent infertility. The main indications for sperm and testicular tissue cryopreservation are the following:
Patients with neoplastic or autoimmune diseases about to undergo gonadotoxic therapies that may impair future fertility Patients with urological diseases needing to undergo surgical treatments capable of damaging ejaculation mechanisms Patients affected by genetic diseases that may severely affect spermatogenesis (e.g., Klinefelter's Syndrome) Patients awaiting vasectomy Preventive cryopreservation in severe oligoasthenozoospermic and cryptozoospermic patients, to prevent the possible evolution in azoospermia Preventive cryopreservation in cryptozoospermic patients undergoing ART, including for psychological reasons Preventive cryopreservation for subjects in active duty in a dangerous occupation Male to female transgender adults and adolescents Sperm donors
Chemo- and radiotherapy protocols have different effects on spermatogenesis. The damage they cause depends on several factors, including pretreatment semen quality, tumor histotype, 2 and the pharmacological characteristics of the protocol itself. The patient's individual susceptibility to the treatment also seems to be important. 3
Antineoplastic agents selectively damage premeiotic cells, spermatogonia, and primary spermatocytes, in which nuclear alterations block replication, thus impairing all downstream spermatogenesis. 4 It is not possible to identify before the treatment which patients will suffer permanent impairment of spermatogenesis and which will recover. For this reason, sperm cryopreservation is the most effective tool to preserve the future fertility of boys and men of reproductive age who must undergo treatment for cancer. The latest antineoplastic therapies and the progressive improvement in the quality of ART have enabled even infertile men with serious iatrogenic damage to spermatogenesis to become fathers.
More than 50% of young cancer survivors state a desire for paternity after treatment, including 75% of those who did not have children at the time of diagnosis.5,6 Around 8% of such patients uses their cryopreserved semen samples, although the exact percentage varies between centers. Nearly half (45–49%) of these become fathers, that is, 3.9% of all patients cryopreserving their semen before treatment.3,7 However, this rate is probably underestimated, given the youth of these patients and the increasing length of their follow-up. 8 Sperm cryopreservation also enables women to use their partner's sperm when collecting oocytes, if the partner cannot be present or has psychological difficulties in collecting the ejaculation.
Urological surgery such as radical prostatectomy and transurethral resection of the prostate is associated with an increased risk of retrograde ejaculation, meaning that the semen ejaculates into the bladder rather than out through the penis. In such cases, sperm cryopreservation can overcome the possible consequent infertility.
Recently, an important role of cryopreservation has been proposed in the management of subjects with gender dysphoria. The hormonal and surgical treatments that transgender men and women undergo cause significant disruption of the individual's fertility. Thus, a fertility preservation strategy is increasingly discussed and offered by health care providers in this setting. 9
Finally, cryopreservation now enables infertile couples to use donated gametes. In vitro fertilization with donor oocytes or sperm is an increasingly common treatment strategy for men and women who cannot rely on their own gametes. 10
Oocyte cryopreservation
The last three decades, and especially the last 10 years, have seen the perfection of oocyte cryopreservation techniques, with the achievement of three main objectives: successful intracytoplasmic sperm injection, improved cryoprotectant quality, and the introduction of the vitrification procedure.11,12 Oocyte vitrification enables high postthaw survival rates and pregnancy and live birth rates similar to cycles with fresh oocytes. 13 Oocyte cryopreservation has thus become a cornerstone in preserving female fertility in many clinical conditions. The most important are the following:
Cancer patients who must undergo potentially gonadotoxic therapies
Patients with ovarian hyperstimulation syndrome
Patients previously classified as “poor responders”
Women with an increased risk of premature ovarian failure and infertility due to genetic alterations (BRCA mutations, Turner syndrome, X chromosome deletions)
Couples who do not want to cryopreserve an excessive number of embryos for ethical, legal, or religious reasons 14
Literature reports of the outcomes of oocyte cryopreservation are highly variable, and the different protocols used, the age of the patients, and the number of frozen-thawed oocytes and transferred embryos mean that they cannot be compared. The main differences in outcome seem to depend on the oocyte freezing method. The fertilization rate, embryo development, and pregnancy rate for vitrified oocytes are comparable to those of fresh oocytes, while oocytes treated with slow freezing have significantly lower rates of success. Since 2006, the embryo implantation success rate has increased from 2% to 14% and live birth rates from 2% to 27% when slow freezing was used, in comparison with increases from 13% to 20% and from 23% to 35%, respectively, 7 when vitrified oocytes were used.15–17 In recent years, an increasing overall post-thaw oocyte survival rate has been reported, with recent studies reporting a rate of about 90%.18–19
Legal aspects of biological material distribution
In Italy, Law 40/2004 on ART regulates the distribution of cryopreserved material in fertility centers, under the section reporting guidelines for medically assisted reproduction procedures and techniques (Article 7, Law 40/2004; Health Minister's Decree of July 1, 2015). Transport of stored biological material is also regulated more exhaustively by Legislative Decree 191/2007 and Legislative Decree 16/2010. 20 These implement the European directive (23/2004) and establish quality and safety standards for the donation, procurement, testing, processing, preservation, storage, and distribution of human tissues and cells in tissue establishments; distribution is also regulated by the Health Ministry's Decree of October 10, 2012 concerning the “importation and exportation of human tissues, cells, and reproductive cells.”
Incorrect handling of cryopreserved biological material can damage cell viability through exposure to a drastic temperature change. This can trigger the ice recrystallization process and other chemical reactions affecting the integrity of the biological material. The distribution of cryopreserved materials thus involves three main determining factors: the means used to store and transport the sample, the components used to keep it cold, and the total transport duration. 21 The latter should be as short as possible if carried out at −80°C, as the fertility of motile sperm progressively decreases due to functional deterioration of the spermatozoa themselves.22,23 Longer times can be tolerated for samples transported in nitrogen vapors (−130°C) and in liquid nitrogen (−196°C).
The accurate sharing of technical information on the material's “freezing history,” traceability and compliance is also required to ensure future cell viability. This information is necessary for both patient and laboratory safety.
The transfer process comprises several steps (Figs. 1–3).

Steps transfer process.

Steps transfer process.
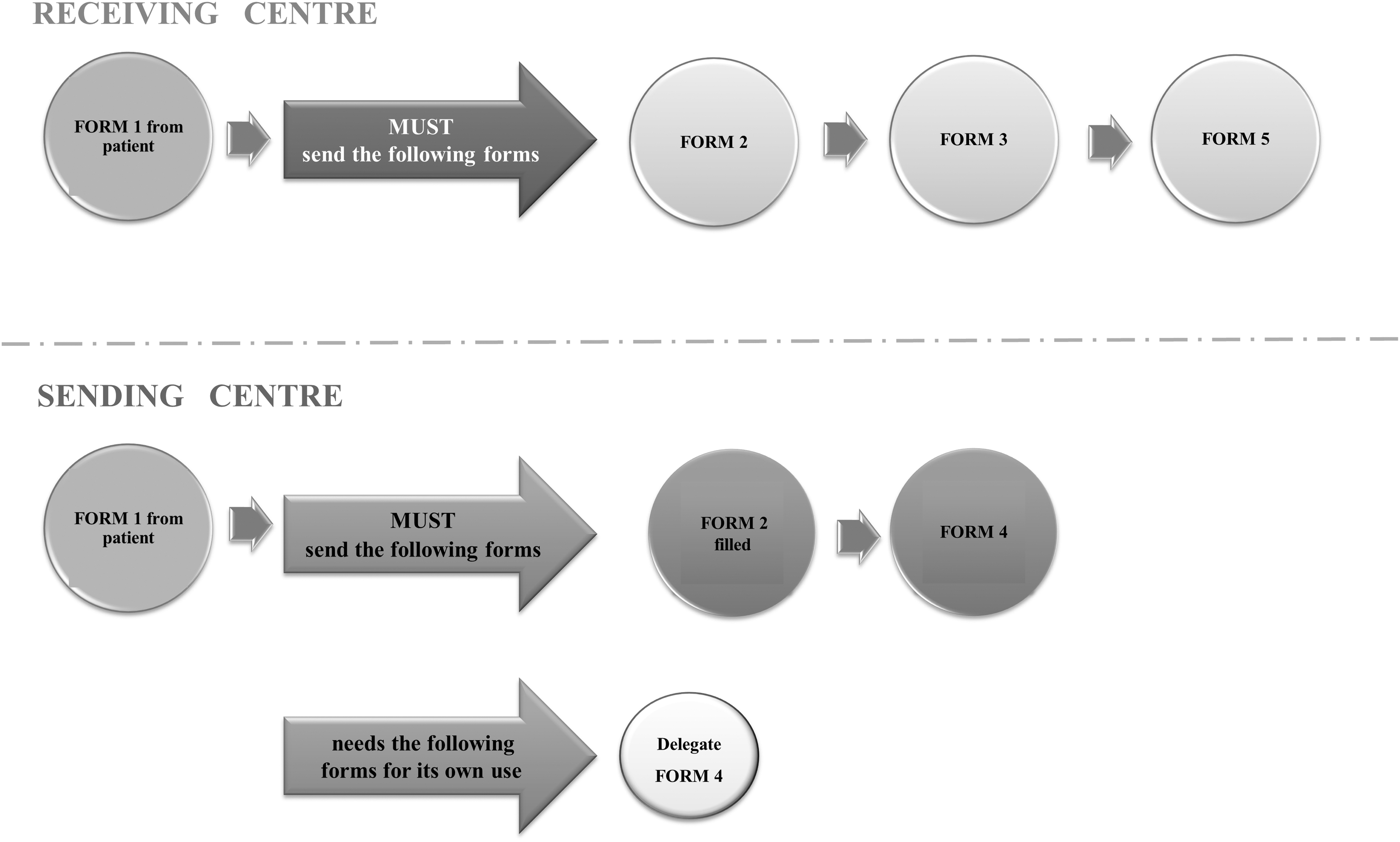
Forms exchanged between the receiving and sending centers.
Activation of the procedure by the Italian center receiving the patient's request
Sending center: tissue establishment storing the biological material
Receiving center: tissue establishment that will receive the material on the patient's request
Patient authorization and consent to the processing of personal data
The patient/couple undergoing ART and requiring the transfer of cryopreserved material to another center presents their official request to the two centers and consent to the processing of their personal data pursuant to GDPR 679/16 and Legislative Decree No. 196/2003, allowing the centers to exchange “sensitive” data and information about their cryopreserved sample and state of health (Supplementary Form 1).
Request by the receiving center
In compliance with Italian law, the receiving center, having been authorized by the patient/couple, forwards to the sending center the applicable information request form in relationship to the type of cryobanked material (sperm, oocytes, embryos) and its suitability, attaching a valid patient's identity document. The receiving center must check that the sending center is authorized by the Italian National Transplant Center (CNT) as a Tissue Establishment (TE) by verifying the sending center's TE code (Supplementary Form 2).
Checks by the sending center
The sending center must verify the patient's request and check that the receiving center is authorized by the National Authorities for ART activities by verifying its presence in the list of TE.
The sending center must also check that
the material has the necessary documentation;
the documentation corresponds with the personal data of the patient/couple;
the material is physically present in the center's storage containers;
all identification codes are present for traceability;
the number of specimens correspond and that they are undamaged.
A copy of all the documents required in relationship to the type of material is then sent with the following completed forms (Supplementary Form 2) to the receiving center:
informed consent;
cryopreserved material report;
required infectious disease tests;
patient/couple ID;
number and type of storage holders/straws and their identification codes;
material lot number.
Checks by the receiving center
The receiving center assesses the conformity of the cryopreserved sample, the feasibility of the assisted reproduction attempt, and the type of cryopreserved material. The receiving center decides the amount of material to be transferred with the couple/patient through appropriate counseling and indicates the type and quantity of material to be transferred (Supplementary Form 3).
Once the receiving center has declared the material and the documentation to be “suitable,” it sends confirmation of its acceptance of the transfer to the sending center via fax or e-mail (Supplementary Form 3).
The two centers then agree a date for the transfer.
Initiation of transfer process and collection of biological material from the sending center
On the agreed material collection date, the specialist courier comes to the sending center with a suitable transport container, and the center does the following.
Verifies the identity of the patient/couple and specialist courier through their identity document
Inspects the transport container to assure conformity
Transfers the material to the transport container (to be carried out by two members of the sending center's staff)
Closes the container with a tamper-proof seal
Labels the container appropriately (including prohibition of irradiation, if applicable), without including any “sensitive” data
Makes a copy of all documents
Completes (Supplementary Form 4) and gets it signed by the courier
Releases the container containing the cryopreserved material
Transport and acceptance of the material by the receiving center
The courier should deliver the frozen material directly to the receiving center as soon as possible, and mandated to be within the guaranteed lifetime of the container. During transport, the container must not be turned upside down or opened for any reason and must be placed in a secure upright position.
Before final acceptation of the material, the receiving center does the following.
Verifies the identity of the courier through their identity document
Checks the completeness of the paper documentation
Checks the conformity and integrity of the transport container
Checks that the material corresponds with the paper documentation and that the samples are undamaged
Once these checks have been successfully completed, the receiving center accepts the material and assumes responsibility for its handling and traceability. It then completes the material receipt form and sends it by fax or e-mail to the sending center. The transport procedure is closed upon receipt by the sending center of the correctly completed form (Supplementary Form 5).
In the event of any nonconformity, the receiving center will contact the sending center immediately and open an adverse event report.
Footnotes
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.