
Abstract
Diseases that manifest themselves in the pediatric age group frequently have a more diverse spectrum of abnormalities and a greater rarity than diseases that are primarily seen in adults. The complexity and the relatively small populations with specific diseases are factors that have hindered progress in the treatment of pediatric disorders. Personalized medical therapies that are specifically tailored for individuals with unusual or unique problems have great potential to assist in overcoming these factors that have been a bottleneck to pediatric medical success. Personalization of therapies will necessarily be data driven and will require delineation of the proteomic, genomic, epigenomic, and immune characteristics of patients in comparison to the general population. It follows that there is a need to provide researchers with accessible high-quality pediatric tissue collections to facilitate the acquisition of the molecular information needed to support personalized medicine. Because of the unusual nature of many pediatric diseases, sample pools from individual institutions are often too small to adequately power definitive studies. Thus, etiological and translational research in this area are increasingly relying on biobanking networks to provide investigators with adequate numbers of tissue samples. Several pediatric biobanking networks have been formed, which are aimed at increasing the power of research studies and desired pools of high-quality samples. However, despite the concerted efforts, these multicenter networks and collaborations have met with mixed outcomes owing to increasing complexities and heterogeneity in the biobanking arena. While there have been challenges and roadblocks, there also have been some positive outcomes that have had paradigm impacts on diagnosis, study, and treatment of specific diseases. This article highlights the need for establishing pediatric biobanks, how current efforts in pediatric biobanking are influencing the pediatric research landscape, and attempts to identify practical impediments that continue to hamper advancements for the future.
Pediatric Disease and Development
During early life, the developmental pathways may become abnormal or remain incomplete, resulting in disruption of normal functional activities of all other organ systems. Overall morbidity and mortality have decreased substantially in pediatric diseases following advances in medical and surgical management for several devastating diseases. However, there has been little change in the incidence of developmental defects. Despite the heterogeneity in the etiology of pediatric diseases, there is a considerable overlap in the molecular and cellular pathways. Similar to cancer, several congenital pediatric disorders are known to arise through multifactorial inheritance such as cleft lip or palate, clubfoot, congenital dislocation of the hip, congenital heart disease, pyloric stenosis, and urinary tract malformations. Over the past decade, significant advances have been made in the understanding of the genetic regulation of pediatric cancer; however, due to the heterogeneity and rarity of many other developmental disorders, progress in this area is lagging behind.
With the success of human genome sequencing, researchers are now better able to comprehend the complex interplay of different transcription factors and genetic polymorphisms with one another as well as the influence of environmental factors, such as maternal viral infections, retinoic acid, lithium, maternal diabetes mellitus, gestational hypoxia and so on, that result in either normal or abnormal organ development. However, there is still a considerable gap in the knowledge about the basic understanding of disease mechanisms for the implementation of new therapeutic strategies and opportunities.
Children have a dynamic developmental physiology owing to which they are more susceptible to developmental and environmental hazards. Their physiology is undergoing constant and continuous changes. These physiological changes, that are somewhat intact in adults, are going through development differentiation and maturation phases making them vulnerable to various unique disease risks that can alter normal function and structure. The risk exposure pathways in children are also varied. They can be exposed in utero to chemical, physical, or biological toxicities via the mother's placenta or after birth to these pollutants via mother's milk for example, as evident in the effect of maternal folate and neural tube defects in infants. 1 These routes of exposure do not occur in adults or older children. The constantly changing developmental physiology of children involves multiple molecular and cellular pathways. With the possibility of an alteration in one pathway affecting multiple pathways, children are at increased risk to develop more complex syndromes as compared to adults. In parallel to deducing different genes that play a role in disease development, the understanding of gene–environment interactions in children is of utmost importance. 2
Gaps in Translational Research
The slow rate of progress in understanding congenital pediatric diseases is primarily not only due to the rarity of individual diseases but also due to the lack of public awareness and the consequent insufficient funding from federal agencies, pharmaceutical companies and medical institutions. As a result, few physicians and research scientists have the capacity to study pediatric diseases in depth.
Frequently and erroneously, findings from studies done on adults are applied to children even though there are distinct differences between the two groups. 3 Because the causes of the diseases remain unknown, developments in targeted and effective therapies continue to lag behind other adult diseases.
Several studies support the need for robust and rigorous research efforts in pediatric population. A National Cancer Institute (NCI)-funded study of nearly 1,000 children and young adults with acute myeloid leukemia (AML) was a part of the Therapeutically Applicable Research To Generate Effective Treatments (TARGET) initiative. TARGET was a collaborative effort between NCI and the Children's Oncology Group (COG) to better understand the biology of several high-risk or hard-to-treat pediatric cancers, which reported that at the genetic level, AML differs greatly between younger and older patients. They reported 142 driver genes in pediatric cancers, of which only 45% match those found in adult pan-cancer studies. These data emphasize the need for pediatric cancer-specific development of precision therapies and necessitate the need for shift in focus during therapeutic development when targeting pediatric diseases.4,5
This discrepancy in disease architecture has also been evident in major disease groups other than cancer, such as cardiomyopathy and pulmonary arterial hypertension (PAH), that eventually culminate into heart failure. 6 Compared with adult-onset, the pediatric-onset PAH disease is more heterogenous and often associated with a worse prognosis. 7 Similarly, cardiomyopathy in adults and children share causes of mutations in key structural genes; however, nearly 30% of children have an underlying metabolic, syndromic, or neuromuscular condition causing their cardiomyopathy, making the etiologies more diverse in children compared with adults. Genetic research in cardiac diseases in the pediatric population can enhance the understanding and will present many other advantages that include confirmation of the diagnosis in ambiguous cases, facilitating management of other cardiac and extracardiac diseases, prognosis, and establishing the genetic basis in the family. While some guidelines for approaches for genetic testing and family screening in patients with some forms of cardiomyopathy have been published, 8 use of genetic testing data for better management and prognosis of the disease requires larger cohorts and big data analysis.
Barriers in Pediatric Research
Working with pediatric subjects has been laden with many challenges. These encompass a wide array of areas ranging from ethical, regulatory, operational to economical, and are encountered in both the clinical and the research setting.
Recruitment and regulatory issues such as reconsent and data privacy have significantly hampered the growth of research in this population. These issues have been a topic of controversial debate for many years, and continue to remain barriers with little to no progress. 9 Small patient populations, characteristics of pediatric physiology and pathophysiology, practical, operational, and ethical difficulties have complicated the designing of successful preclinical trials. Due to these limitations, implementing suitable drug testing and safety protocols have also been difficult. Ultimately, the gaps and discrepancies between the number of clinical trials and pediatric disease have grown and are becoming more evident.10–13
The Convention on the Rights of the Child 14 stipulates that all children have a right to the highest attainable health care. However, most therapies are based on evidence generated through studies carried out in adults.15,16 This is counter effective as drug action and metabolic mechanisms differ in children and adults. There are disparities in their metabolic pathways with respect to receptor functions, chemical interactions, and homeostatic mechanisms. Moreover, age, growth, and development have varying effects on the severity and nature of the disease, thereby warranting drug dosage adjustments. 17 Owing to these differences, extrapolation of adult data leads to errors, 18 and it is ethically imperative that these discrepancies be eliminated.
The unavailability of appropriate normal sample controls has hampered pediatric research even further. The continuing development of children makes it imperative that normal controls are closely age matched. This is an enormous challenge in a population where any normal control sample is significantly more difficult to obtain compared to adult normal control samples. In addition, the lack of accessibility of fresh tissue makes autopsy tissue an important alternative. However, there are several limitations to its use and effective measures need to be in place to minimize the effect of agonal factors, postmortem intervals, and storage conditions that contribute to specimen degradation.19–22 Several studies have reported the value of autopsies in pediatric research. However, most of these studies have been conducted on discrete and specific patient populations.23–25
Further efforts should be aimed at increasing autopsy rates through education of clinicians, pathologists, patients and parents, improved funding for autopsies, a mechanism for quality assurance, as well as specimen sharing opportunities, so each precious specimen can be used to its fullest potential. Conducting well-planned experimental studies investigating the age-based differences in degradation of tissue quality to develop standards for storage, handling, and use of pediatric postmortem tissue in molecular research is crucial.
Current Efforts: Pediatric Networks
Currently, the majority of biobanks in the United States are adult focused with only 44% including any pediatric participants and 2% focused entirely on pediatric patients. 26 Solutions for all the outlined issues require collaboration between academia, industry, and government as well as creativity in designing pediatric studies. Developing disease markers specific to rare pediatric diseases, making genomic correlations, and developing new treatment and longitudinal monitoring strategies can only be attained by establishing pediatric biobank networks and assembling large pediatric study populations27–30 (Fig. 1).
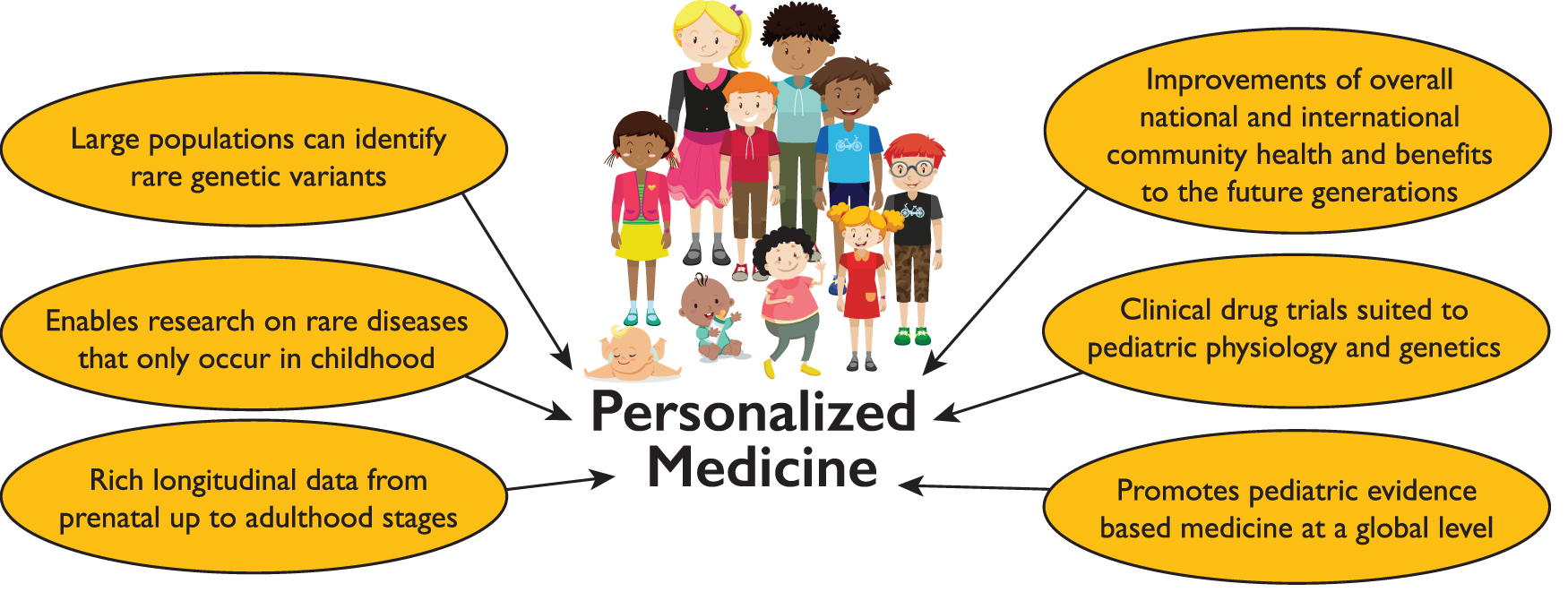
Benefits of pediatric biobanking. Color images are available online.
Regulatory barriers, limited resources in management, and infrastructure have so far prevented seamless linkage, interoperability, and scalability of biobanking networks. 31 Formation of networks is typically driven by the type of biobank and its goals. Although pediatric biobanks vary widely in size and type, ranging from small laboratory or single research team collections to larger networks of repositories, they generally fall into three main categories: (1) disease-specific (2) residual tissue repository that is a resource of remnants from the short term or the long term course of a treatment of patient, and (3) longitudinal or population biobanks that recruit and maintain large general populations from a small region to global cohorts with purpose of epidemiological and population health studies.32,33
Disease-specific biobanks are often the ones that come together to form networks. Disease-specific data hubs or registries such as The Rare Disease Hub (RD-HUB) a centralized database of biorepositories for rare biospecimens was established by the Office of Rare Diseases Research, National Center for Advancing Translational Sciences, National Institutes of Health (NIH), to aide researchers in locating RD biospecimens and facilitate the link between specimens and patient clinical data that resides in the Global Rare Disease Patient Registry Data Repository. 34 Many rare diseases primarily involve children and most are genetic in their etiology. Linking a genetic variant with a particular disease requires large number of unrelated individuals who have a genetic variant in common, as well as exhibiting a similar clinical phenotype. Therefore RD-HUB serves as a unique resource for storing and disseminating such useful pediatric data. 35
With rapid advances in next-generation sequencing and generation of big genomic data, large-scale genomic studies have been conducted by the eMERGE network. This network has two pediatric centers and is by far the largest multicenter platform that has developed pediatric cohorts for genome-wide studies by integrating genomics, medical records, and clinical data to effectively study and evaluate the outcomes, effects, and response of pharmaceutical treatments.36,37
Very few platforms have emerged that share pediatric biological specimens and the formation of pediatric networks or consortiums is far behind those established for adult diseases. One of very few successful pediatric initiatives is the Pediatric Cardiac Genomic Consortiums (PCGC). PCGC, funded by National Heart, Lung, and Blood Institute, is a successful enterprise directed toward the genetic signature of congenital heart defects (CHD) research. CHD and other pediatric disease research are limited by low recurrence, sample scarcity, and high phenotypic variability. The establishment of this consortium leveraged the genomic technology and multicenter participant recruitment to spearhead research for early diagnosis, treatment, and prevention of CHD. Joint studies through this network reported novel mutations in CHD cohorts that share genetic contributions to CHD and neurodevelopmental disorders and is a significant advancement in the field of CHD research.38,39
The similarly long-standing network of COG that represents the largest consortium in North America is banking specimens from children with cancer. The COG works in collaboration with the NIH-funded Cooperative Human Tissue Network and has made significant headways with pediatric cancer research. A recent example of the success of this program is the detection of RAS mutations in 14% of rhabdomyosarcoma samples. 40 In addition, The Gabriella Miller Kids First Data Resource Center is a new, collaborative, pediatric research effort with the goal of understanding the genetic causes and links between childhood cancer and structural birth defects. Many of these networks provide retrospective collections for research.
Understanding organ pathology requires deeper investigation of normal developmental processes and causes and contributions of genetics, gene–environment influences, physical, social, and maternal environment on pediatric health and disease. Inclusion of healthy children in the United States' Precision Medicine Initiative in the All of Us cohort and the local Healthy Brain Network initiative of recruiting 10,000 children and adolescents (ages 5–21) are great steps forward that would provide opportunities to investigate mechanisms of pediatric disorders and boundaries between normative and clinically significant presentations. 41 However, it should be noted that the availability of controls for children <5 years of age, a period during which the largest growth and development occurs, remains virtually absent. Most single center biobanks are unlikely to be able to prospectively collect sufficient cases for most pediatric rare diseases in a reasonable period of time. Functional networks of biobanks are necessary to leverage the strength of larger collections in short time periods and to address important research questions. Biobanking networks offer an advantage in being able to generate retrospective cohorts from their existing stocks or create a prospectively collected cohort size by optimal enrollment.
Future Directions
Accelerating pediatric research requires addressing challenges on multiple fronts. More technology developments such as dry plasma cards 42 and chip assays 43 need to be made to accommodate small sample volumes, that can be shared with several research studies to allow maximal use of these precious samples. Repurposing of remnant clinical samples should be encouraged for improved access and availability of rare specimens. Hospital practices aimed at unifying pediatric biobanks, pathology units, and clinical laboratories for optimal management of the patients' biomaterials for diagnostic and research projects should be streamlined and implemented.
Advances in bioinformatics and laboratory information systems to facilitate pediatric specific data and sample storage, management, and sharing are warranted. Harmonizing data elements and linking together of longitudinal biobanks for generating outcomes based on genetic makeup and health determinants of pediatric population.
Regulatory restrictions will need to be reformed to provide participative conditions for pediatric subjects that entail minimal risks. 44 Processes where biobanking is embedded into the health care system and utilization of treatment and outcomes data for leveraging the biobank potential should be encouraged. 45 Complexities of pediatric disease requires building large, longitudinal, and comprehensively annotated cohorts that can potentially enable better understanding and investigation into the development, treatment, and prevention of pediatric diseases.
Summary
It is imperative to do research on the pediatric population as they have a major social and economic contribution to the world. Children are ethically a vulnerable population where assenting and reconsenting of the child at age of maturity are often required and perception of on risks/benefits to participate in biobanks between adults and children may vary. Most children have rare and complex syndromes and comparison of children's samples and outcomes is hampered due to the marked biological variation between age groups in children as well as disease heterogeneity. Therefore, collecting specimens across all ages is critical to allow a useful collection to be built. To achieve this, biobanking should be integrated into children's clinical care. Normal controls as well sufficient amounts of samples are very difficult to obtain in the pediatric population especially from newborns, infants, and toddlers, requiring technical modifications in processing and new method development for processing small samples. Due to all of these limitations, virtual networks and collaboration between pediatric networking with good governance and sustainable models is critical to ensure sufficient sample sizes. These biological, physiological, and ethical distinctions between adults and children highlight the need for focused and dedicated pediatric biobanking efforts and will hopefully influence our current biobanking practices.
Footnotes
Author Disclosure Statement
No conflicting financial interests exist.
Funding Information
No funding was received for this publication.