
Abstract
Intensive treatments necessary to treat some childhood malignancies and other conditions, as well as certain anatomic variations, may lead to infertility in adulthood. Until recently, no fertility preservation options for prepubertal females were available. However, ovarian tissue cryopreservation has emerged as a safe and effective option for these children. In the next several years, it is likely that more pediatric patients, their families, and medical teams will pursue an ovarian cryopreservation protocol at their institutions. Patient selection, consenting, and laparoscopic oophorectomy can be done at many centers. Then, the ovarian tissue is initially processed and transported to a specialized center for processing for cryopreservation. The cryopreservation techniques are best performed at appropriately certified centers processing high volumes of reproductive cells/tissues with expert personnel and specialized equipment. This article aims to provide an overview for pediatric biobank professionals who may be called to participate in this or similar protocols.
Introduction
A
Unfortunately, there are conditions that either predispose to infertility, or require treatments that increase the chances of later infertility. These treatments include gonadal toxic chemotherapy agents, abdominal and pelvic radiation, bone marrow transplant, differences of sexual development, ovarian tumors, gender reassignment treatments or surgeries, and metabolic disorders. Therefore, a wide variety of pediatric specialists and their patients are increasingly interested in options to preserve fertility potential. In addition, childhood cancer survivors note significant psychological benefits from discussions of and participation in fertility preservation. 1
For postpubertal females, the current standard of care for fertility preservation is to cryopreserve oocytes or embryos, which can be used in the future to create a pregnancy. 2 However, this procedure is limited to postpubertal females and cannot be utilized in those patients who require urgent treatment for their condition. Therefore, interest in ovarian tissue cryopreservation (OTC) has been growing.
Ovarian cryopreservation consists of removing a portion of the ovary or the entire ovary during a laparoscopic or open abdominal surgery. This surgery is performed by either a pediatric/adolescent gynecologic surgeon or general pediatric surgeon. The tissue is then transported to a specialized facility that performs the cryopreservation process. The specialized facility must have the equipment needed, personnel with training, and a high enough volume to perform these procedures safely, and must be Clinical Laboratory Improvement Amendment (CLIA) and Federal Drug Administration (FDA) approved.
After the ovarian tissue is processed and frozen, it is stored in liquid nitrogen at a temperature of −195°C (−319°F), either at the fertility preservation institution or at a third-party commercial location. Storage of the tissue requires the facility to be accredited by the American Association of Tissue Banks (AATB). When the patient has completed the treatment, the ovary may be reimplanted into the abdomen, allowing for the reinstitution of endogenous hormonal secretion and the possibility of an assisted or unassisted pregnancy to occur. In the future, it is likely that the ovarian tissue may also be matured on an artificial matrix (an “artificial ovary”) outside of the body, 3 which decreases the possibility of reintroducing malignancy back into the body. In this context, it is important to exclude a BRCA gene mutation due to the higher risk of ovarian malignancy. 4
When OTC was initially utilized, national and international committees recommended that it be offered only as a part of an institutional review board (IRB)-approved protocol. However, the technology has matured and more than 130 babies have been born after transplantation of cryopreserved ovarian tissue. Based on this evidence, the American Society for Reproductive Medicine (ASRM) recently advised that the experimental label could be removed from OTC. 5
Lifting of the experimental label will likely increase the clinical demand for OTC, and insurance companies will hopefully soon start covering the costs. Therefore, more institutions may be interested in offering OTC, and will either process the tissue in-house, or contract with a third party for cryopreservation. In either case, some tissue handling and/or processing will always need to be done at the institution where the ovary is harvested. Therefore, pathologists and biobank personnel need to be aware of the techniques involved in the process (Fig. 1) to ensure quality care.
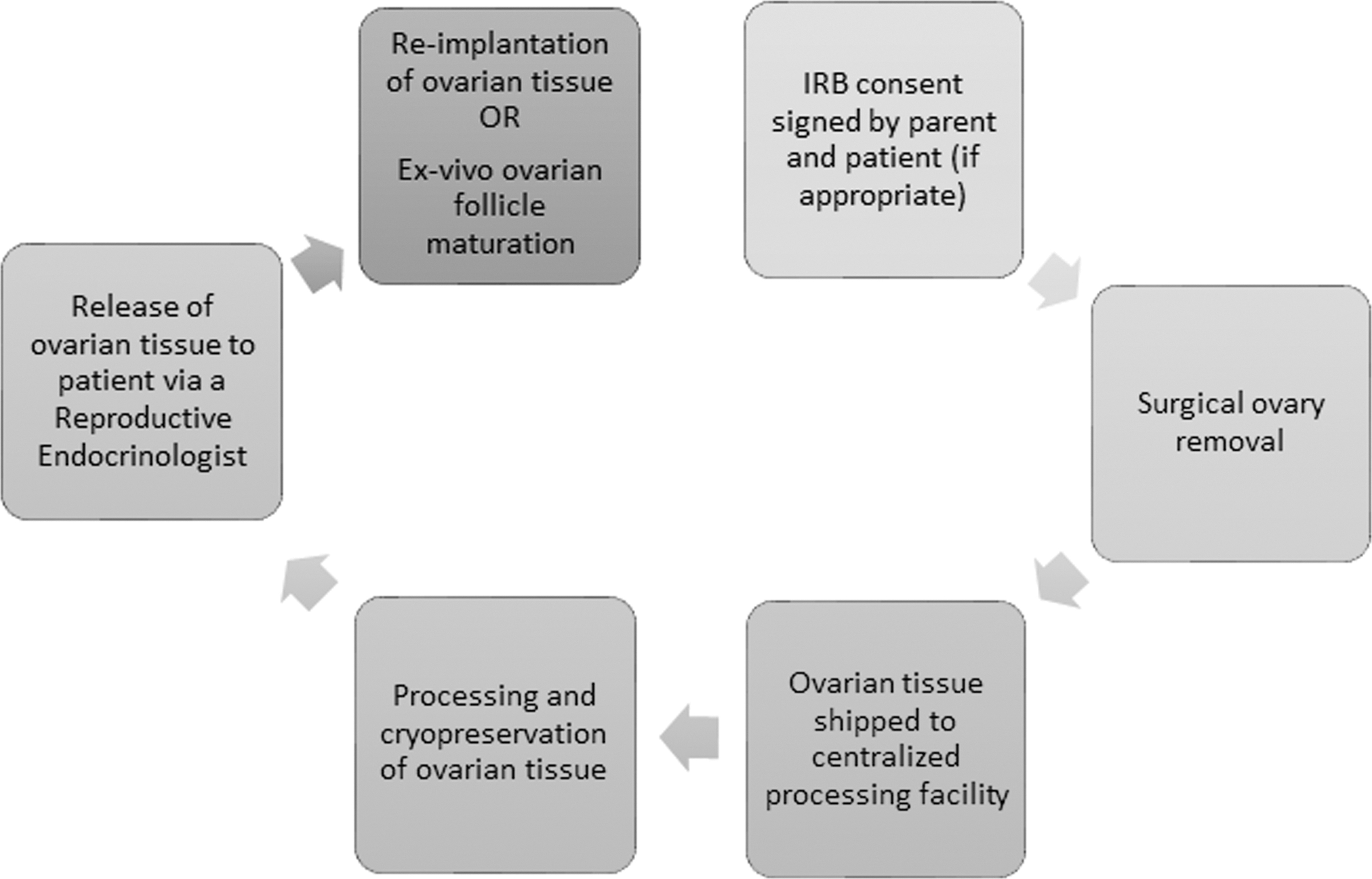
Flow diagram for the process of ovarian tissue fertility preservation.
Background
Genetically XX females are born with about 1 million primordial follicles that decline in number over time due to apoptosis and atresia. When a young person goes through puberty, hormonal levels increase, leading to secondary sexual characteristic development and, in the case of an XX female, maturation of the ovaries. During each menstrual cycle, a group of ovarian follicles mature and an average of 30–40 follicles develop. One dominant follicle then releases the matured oocyte during ovulation and the remaining maturing follicles die. 6
Treatments for malignancy and other conditions with gonadal-toxic therapies decrease the follicular reserve. As fertility is directly related to the number of primordial follicles, these treatments can significantly decrease patients' ability to have their own children. 7 Higher doses of alkylating chemotherapy agents (such as cyclophosphamide, procarbazine, and busulfan) and any dosage of radiation in the vicinity of the ovaries both have the potential to damage ovarian follicles. Higher doses of radiation to the brain (>35 Gy) also can affect future fertility. 8 Fertility preservation counseling is recommended for all patients who are at risk for the development of infertility due to cancer therapies. 9
Spermatogenesis, the process that produces sperm in the testes of men, is a stem cell-based process that maintains continuous sperm production throughout the postpubertal life of men. In contrast, women are born with a finite number of follicles in their ovaries. Once the majority of ovarian follicles have been matured, the female begins to go through menopause. Early menopause is associated with a decreased quality of life as well as the development of osteoporosis and cardiovascular disease. 9 Stem cell and testicular tissue transplantation technologies are under development,10,11 but there are no reported births from transplanted testicular cells or tissues in humans.
In contrast, ovarian tissue transplantation (OTT) has already been utilized to produce healthy pregnancies. OTT was first performed in the 1980s, with the first successful reimplantation leading to ovarian function described in 2000. 12 The first successful live-birth to result from ovarian transplantation occurred in 2004 and a second in 2005. Since then, the number has risen exponentially, more than doubling between 2015 and 2017. 13 As of 2017, over 130 live-births have been reported worldwide, 14 with the actual number likely much higher due to underreporting (Fig. 2).

A significant logarithmic increase in ovarian tissue reimplantation in an orthotopic site since 2004 (note: with permission from Donnez et al. 14 ).
The ovarian tissue can either be transplanted back to the previous location (orthotopic reimplantation), or to an alternative site (heterotopic reimplantation). Overall pregnancy rates with orthotopic ovarian transplantation are not known precisely but are encouraging. In one center, in a study of 49 patients with follow-up of >1 year after orthotopic reimplantation, 67% had evidence of hormonal activity and 33% had become pregnant. 15 Other centers have reported lower rates of pregnancy (29%–33%) and live-births (23%–25%). 5 In all, about 100 centers worldwide are currently performing OTC.
The Oncofertility Consortium's National Physician's Cooperative (ON-NPC) was established in 2007, and now includes 38 member institutions in 20 states, with 16 institutions enrolling pediatric patients. 16 Participation in the study defrayed the cost of OTC. In 2018, the consortium published its experience with OTC in females <15 years of age. A total of 114 cases were performed in patients ages 1–14 at the time of OTC. 17 The patients undergoing OTC were found to be more likely to have soft tissue sarcoma or neuroblastoma (cancer types that are more likely to receive chemotherapy or radiation, which threatens fertility), than age-matched controls, suggesting that appropriate patient populations were undergoing OTC. 16
Since the ON-NPC is no longer actively enrolling patients, individual institutions have opened their own research protocols. In the United States, these live-birth outcomes from OTT have prompted a concerted effort to remove the experimental designation of the ovarian cryopreservation procedure, which would pave the way for increased insurance coverage.2,18,19 However, there is only one reported live-birth from tissues that were cryopreserved during childhood. 17 Therefore, most institutions will continue to offer OTC under IRB-approved research studies. As part of a research trial, as an added benefit, excess harvested ovarian tissue may also be utilized to develop improved technologies that will allow improved care for these patients in the future.
As an example, the inclusion criteria for participation in the research protocol at Phoenix Children's Hospital (PCH) are as follows:
Female age 1–25 years old Either: (a) Newly diagnosed or relapsed malignancy with proposed treatment regimen containing at least ONE (1) of the following: (i)Whole abdomen or pelvic irradiation (ii)Total body irradiation (TBI) (iii)Proposed treatment regimen to include any of the following: (1)Cyclophosphamide equivalent dose (CED
20
) ≥7.5 g/m2 (2)Any treatment regimen containing procarbazine (3)Bone marrow transplant conditioning regimen containing alkylators (b) OR: health condition or malignancy requiring removal of one or both ovaries Need for another surgical procedure (i.e., for line placement or mass biopsy) Health status adequate to undergo elective laparoscopic surgery (as per anesthesiologist assessment).
Other female patients who are at risk for decreased fertility include patients with rheumatologic conditions, gender dysphoria or reassignment, metabolic disorders, and those with genitourinary tract abnormalities. Patients requiring the removal of one or both ovaries for benign conditions may also benefit from OTC. Although the exact number of patients who could benefit from these procedures is difficult to accurately ascertain, there are ∼300,000 children with rheumatologic disorders in the United States 21 and estimates of gender dysphoria in pediatrics are 0.5%–1.3%. 22 Malignant ovarian tumors are rare in childhood, with an incidence of 0.71/100,000, 23 and metabolic disorders occur in about 1/784 live-births. 24
Among patients with disorders of sexual development, gonads may be removed before puberty for a variety of reasons. The diagnoses include androgen insensitivity syndromes, both complete and partial, as well as mixed gonadal dysgenesis and Turner's syndrome with Y material among others. So far, these patients have had limited access to gonadal tissue preservation. Similar to oncologic patients, shared decision-making and IRB approval are critical due to ethical issues regarding long-term use. Preliminary work has begun for this group and their care will continue to evolve. 25
Harvesting
The ovarian tissue is most often obtained by laparoscopic surgery. This procedure is generally well tolerated, but complications, such as intraoperative bleeding and postsurgical infections, are still higher than when performed in healthy controls at about 1:500. 26 The increased complication rate is thought to be due to underlying medical conditions. The laparoscopy is performed by either obstetricians/gynecologists (either pediatric gynecologists or reproductive endocrinologists), or by general pediatric surgeons. Ovarian size varies with age and pubertal development. Prepubertal ovaries are smaller, and thus, the entire ovary is removed. For older children or adults, a longitudinal strip of cortical tissue can be removed. In a single-institution report, 84% of 64 patients at high risk of future infertility enrolled in a harvesting protocol and had a successful laparoscopic unilateral oophorectomy. 27
Processing and shipment
The aseptically processed ovarian tissue is bivalved along its long axis, dropped into a sample container with Origio Handling media (Cooper Surgical, Trumbull, CT). This medium contains buffers to ensure appropriate pH levels, prevents drying, provides amino acids to support oocyte viability, and vitamins that act as antioxidants; see Figure 3. The specimen is then cooled and shipped to a central processing facility for further processing in a temperature-monitored shipping container at 2°C–8°C. For the Phoenix Children's Hospital IRB-approved protocol, tissue is shipped to the Center for Reproduction and Transplantation at Magee-Womens Research Institute at the University of Pittsburgh Medical Center, Pittsburgh, PA, for further processing.

Upon removal, the ovary is immediately transported to pathology on sterile saline-soaked gauze (top). The ovary is handled in an aseptic manner to obtain weight and measurements. Following this, the sample is bivalved (bottom) to expose the oocyte-containing cortex (outer) and medulla (inner portion) and subsequently submerged in a transport medium for shipment.
Cryopreservation
Once the ovarian tissue is received at the central processing facility, the cortex containing the immature follicles is dissected away from the stroma, cut into small strips (∼0.5 × 2 cm with a thickness of 1 mm) in a sterile class II laminar flow hood, and frozen either by slow-freezing techniques or by vitrification. See Figure 4 for details of the process. Recently, vitrification has become more popular because it is faster and requires less technical expertise. Vitrification involves the conversion of supercooled liquid into a glass-like amorphous solid. The addition of cryoprotectant agents 28 minimizes or eliminates the possibility of ice-crystal formation. Human and animal studies have shown no differences in the numbers of high-quality follicles processed by slow-freezing versus vitrification29–31 although the architecture of the ovarian stroma was better preserved in vitrification than slow-freezing, 31 with increased the numbers of ovarian stem cells obtained from the vitrified ovaries. 30
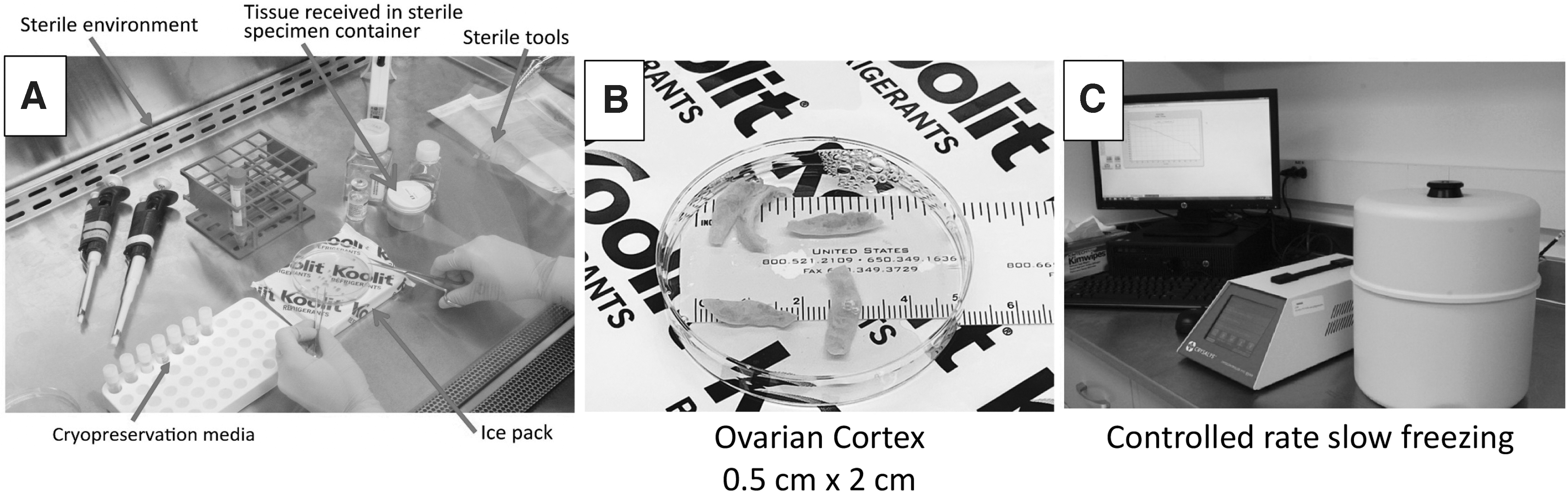
Overview of the cryopreservation technique. The received bivalved ovary is carefully separated into the cortex and medulla in a sterile environment
Controlled slow rate freezing is the method used by the Center for Reproduction and Transplantation in Pittsburgh. Briefly, ovarian cortical strips are deposited in cryovials containing the OFC Cryopreservation Medium (Cooper Surgical, catalog no. ART-8050). Components of the freezing medium are proprietary and not known. Cryovials are then loaded into a programmable freezer at 5°C; cooled at a rate of −2.0°C/minute from 5.0°C to −7.0°C; and held at that temperature for 10 minutes. Each tube is then manually seeded; held at −7.0°C for an additional 10 minutes; and then cooled at a rate of −0.3°C/minute until −30°C before plunging in liquid nitrogen for long-term storage.
In general, cancer patients must wait several years after their final treatment before ovarian tissue reimplantation can occur. This waiting period is often longer for pediatric patients, making long-term viability a crucial issue. In an early study published in 2006, 10 ovaries were evaluated immediately before and then again after freezing and thawing. Results showed that the viability parameters between the fresh and the slowly cryopreserved ovaries were very similar, while the tissue that was frozen quickly had less viability. 32
A study in ewes published in 2009 evaluated the function of cryopreserved versus native ovaries and found restoration of vascularization, follicular, and oocyte development. 33 In one study spanning 18 years, three cryopreserved human ovaries were evaluated for tissue quality, maintenance of ovarian potential, and markers of viability. The markers were similar in tissue samples that were analyzed immediately after slow cryopreservation, after 120 days, and after 18 years, 34 suggesting that long-term storage did not adversely affect function.
Discussion
Improvement to the OTC processes is an area of active research efforts. One significant concern with orthotopic reimplantation is the reintroduction of malignant cells back into the patient. Hematologic malignancies such as leukemia and lymphoma are often present in ovarian tissue. One group has successfully described elimination of leukemia cells by isolating and washing individual follicles. 35 Researchers are currently studying the feasibility of creating an “artificial ovary” with manufactured scaffolding. 3 Resumption of hormonal function and pregnancy has been achieved in murine models 36 using this technique, offering hope for patients who have undergone OTC secondary to malignancy.
The Practice Committee of the ASRM recommends that OTC be offered only by centers with the necessary laboratory and surgical expertise. 5 Individual centers that do not have the necessary expertise or infrastructure, however, may be able to collaborate with other institutions to be able to offer this procedure successfully to patients. While smaller and/or less experienced institutions may not have the resources to develop a specialized fertility laboratory with the experienced personnel to perform the technically challenging vitrification techniques, there is the option to send the ovarian tissue to more experienced facilities for centralized processing, making OTC more readily available to patients everywhere.
This partnership has the advantage of also increasing the volumes at the central institutions, thus continuing to grow their expertise. It also allows for knowledge sharing among institutions, which accelerates the pace of technology development. As suggested previously, organizations involved in this biobank protocol (cryopreservation and long-term storage) often require that their personnel obtain a Certification of Tissue Bank Specialist (CTBS) through the AATB. 37
As suggested, OTC is now expanding to a wider variety of pediatric conditions to preserve fertility and the demand will likely grow as a standard of care. In this scenario, biobank professionals will face an increasing demand for these procedures, and will be a critical part of the team to ensure that OTC is successful for children who may benefit.
Footnotes
Acknowledgments
Thanks to all of the patients and their families in the survivorship and fertility preservation programs at Phoenix Children's Hospital for being our source of continuous inspiration.
Author Disclosure Statement
No conflicting financial interests exist.
Funding Information
No funding was received for this article.