
Abstract
Background:
Early treatment of neonatal biliary atresia (BA) and other end-stage liver diseases can delay or prevent the necessity of liver transplantation (LT). The establishment of a standardized clinical pediatric liver transplantation (PLT) biobank is the prerequisite for scientific research, which helps to provide a qualified sample resource platform for research.
Methods:
Following standardized procedures to establish biobanks, the operational processes and quality control system were formulated. Liver tissue, blood, and stool samples undergoing LT were regularly collected, managed, and stored. Systematic management was conducted in collected specimens and corresponding clinical information.
Results:
Since implementation in August 2018, we have enrolled 49 unique subjects (0–18 years of age); the biobank contains nearly 3000 biospecimen aliquots. The most common LT diagnosis is BA (61.23%).
Conclusion:
The establishment of this biobank is a valuable resource that incorporates detailed clinical and biological information. It will help accelerate the pace of PLT discovery research. ClinicalTrials.gov ID: NCT04477967.
Background
The clinical biobank is a specialized collection of human biological resources and biological information. The prime objective is to provide researchers with biological resources to advance understanding of human health and disease.
High-quality samples can be used to study the pathogenesis of biliary atresia (BA), which can effectively slow down or avoid the degree of cirrhosis in children, thus avoiding the need for liver transplantation (LT). However, these diseases are difficult to diagnose at an early stage, and infants may miss the best chance for treatment. 1 The American Academy of Pediatrics has recommended studies to develop strategies to help detect BA at an early stage. 2 LT has been recognized as the most effective method for the treatment of end-stage liver and bile diseases. Since Starzl carried out the first case of human LT in 1963, 3 after nearly 50 years of exploration and technological innovation, LT technology has become increasingly mature and achieved good therapeutic effects.
Although LT technology is becoming more and more mature, the pathogenesis of a pediatric end-stage liver disease is still not fully understood. As the most common pediatric liver transplantation (PLT) disease, the etiology of BA remains elusive. Hepatotropic viral exposure, either directly causing bile duct destruction or by eliciting an autoimmune reaction, has been proposed as a causative mechanism. 4 Furthermore, it mainly includes inflammation theory, virology, and genetics. 5 Kilgore and Mack pointed out the interplay of genetic predisposition, virus trigger, and progressive autoimmunity, culminating in bile duct injury, fibrosis, and biliary cirrhosis. 6 At the same time, the quality evaluation of LT, postoperative survival rate, prognosis, postoperative complications, postoperative risk factors, management, and experience of PLT is also vital to be studied. The lack of high-quality samples is one of the main factors limiting these studies. 7
There are many deficiencies in basic and clinical studies on pediatric end-stage liver disease, and mining statistical data in animal studies cannot truly transform the data into clinical care for patients. To fully understand the pathogenesis of pediatric liver diseases, a large number of systematic clinical samples must be available to support research. At the same time, to accelerate the progress of personalized medicine, we also need to develop new technologies to improve the diagnosis, prevention, treatment, and management of these diseases, which is also inseparable from the support of the clinical biobank. Therefore, with advances in clinical and basic research, access to a large, representative, and diverse range of clinical resources to increase awareness of PLT is becoming increasingly urgent. China has a large number of diverse population resources. For advanced research of liver diseases, it is relatively easy to obtain a large number of high-quality human biological samples.
In conclusion, as the unique children's hospital with liver transplant qualification in China, the Children's Hospital of Chongqing Medical University (CHCMU) has lost a large number of precious clinical samples of children's LT. During the last year, the CHCMU established a PLT biobank, aiming to collect clinical samples of pediatric end-stage liver disease systematically and expect to make contributions to the research and development of pediatric end-stage liver disease in China in the future. This study aims to guide the biobanker to establish an LT biobank.
Methods/Design
Construction and planning
Site and equipment
The first phase of the biobank center of CHCMU covers an area of about 300 m2, and the second phase is under construction, which covers an area of about 1600 m2. Both of them have seven major functional areas: sample receiving area, information management area, cryogenic storage area, liquid nitrogen storage area, quality control area, cell culture area, and an office area. The first phase can accommodate 20 freezers (−80°C) and 7 large gas-phase LN2 tanks. The total storage capacity of the first phase is about 4.5 million samples. The biobank is equipped with a cold chain temperature monitoring system, environmental monitoring system, and an emergency alarm system, all of which are under a 24-hour monitoring state. The biobank center has an automatic nucleic acid extraction instrument (KingFisher DUO; Thermo), Bioanalyzer and TapeStation Systems (Agilent 2100), fluorescence quantitative PCR instrument (LightCycler 480 II; Roche), and so on. The biobank center uses an advanced sample information management system, which can effectively and accurately track the entire process of samples from generation to end and realize the intelligent management of samples and information.
Personnel
The biobank center has a management committee responsible for overall planning, an academic committee responsible for professional review of resource collection projects, including project design, content, and resource use, and ethics committees, which rely on CHCMU ethics committees.
The center sets up a management office, including the quality controller, sample manager, and sample processor. All staff need to attend the preservice training organized by the Biobank Branch of China Medical Biotech Association (BBCMBA), pass the examination, and obtain the biobank job certificate. At the same time, the staff must participate in the standardized training in our biobank and pass the examination before they can be formally on duty.
Qualification
According to the national regulations, the biobank center has obtained the administrative license for the preservation of human genetic resources and the approval from the ethics committee of CHCMU for preservation activities. At the same time, the liver surgery department of CHCMU has obtained the national LT qualification.
Participants
Ethics and informed consent
The trial has been approved by the Institutional Review Board of CHCMU and registered at No.120/2018.
Liver transplant samples are collected from both donor and recipient populations, so both groups should sign an informed consent. All the recipients are infants or children. A parent/primary guardian represent their infant/child to sign the informed consent to participate in the study. A written or verbal agreement should be provided from children older than 7 years if their parents think they are able to understand the study requirements. There are two major types of donors: parental donors and donation of citizen's death (DCD) donors (Table 1).
Donor and Recipient Grouping and the Requirements for Informed Consent
The numbered conditions need to be met in full.
DCD, donation of citizen's death.
Sample collection and processing
Sample type
To ensure the comprehensiveness of the samples, it is necessary to collect the samples of the donor and recipient. We recommend collecting the tissue and blood from both donors and recipients, and the recipient's stool sample. The specific sample type and volume are shown in Figure 1 and Table 2.
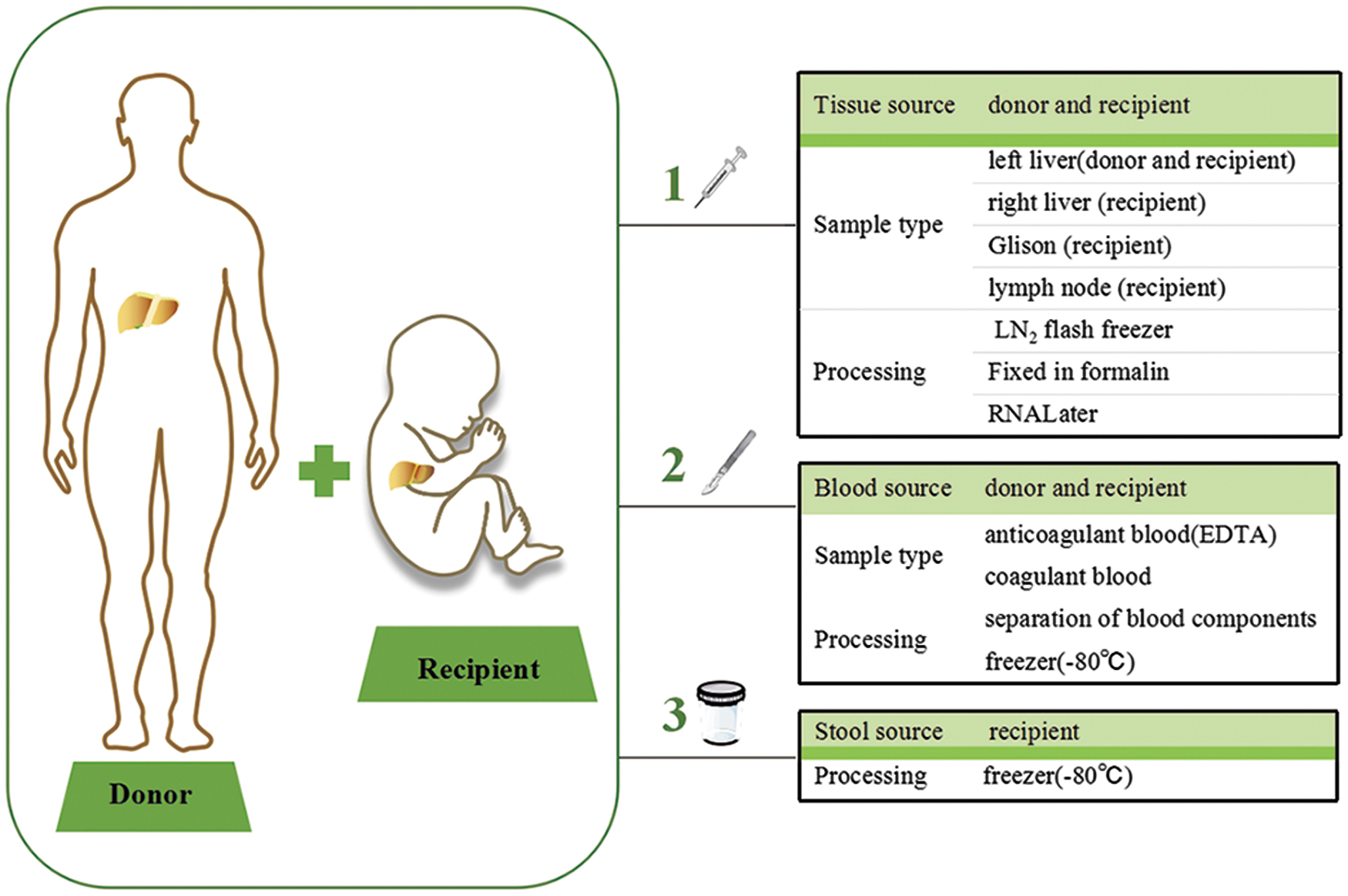
The mode pattern of sample collection.
The Sample Type and Volume
Ethylene diamine tetraacetic acid.
SST.
D, donor; F, formalin; R, recipient.
Tissue sample collection and processing
Before the operation, the biobank will prepare sterile cryopreservation tubes. To avoid cross-contamination during operation, the inner and outer walls of the cryopreservation tubes should be disinfected. For fresh tissue, a pathologist will examine the surgical specimen, and tissue that is not required for the diagnosis will be made available for the biobank. The tissue is generally divided into LN2 fresh-frozen, formalin-fixed sections, and RNALater fixed in the liver biobank. We mainly collected the liver lobes of the donor's graft as left hepatic lobe, right hepatic lobe, Grinson system, and lymph nodes, which will be resected during surgery. The specific sample type and volume are shown in Table 2. The biobanker should take photos immediately after the liver is removed, and then collect the tissue within a cold ischemia time (CIT) of 30 minutes. The specific collection protocol is summarized in Figure 2A.
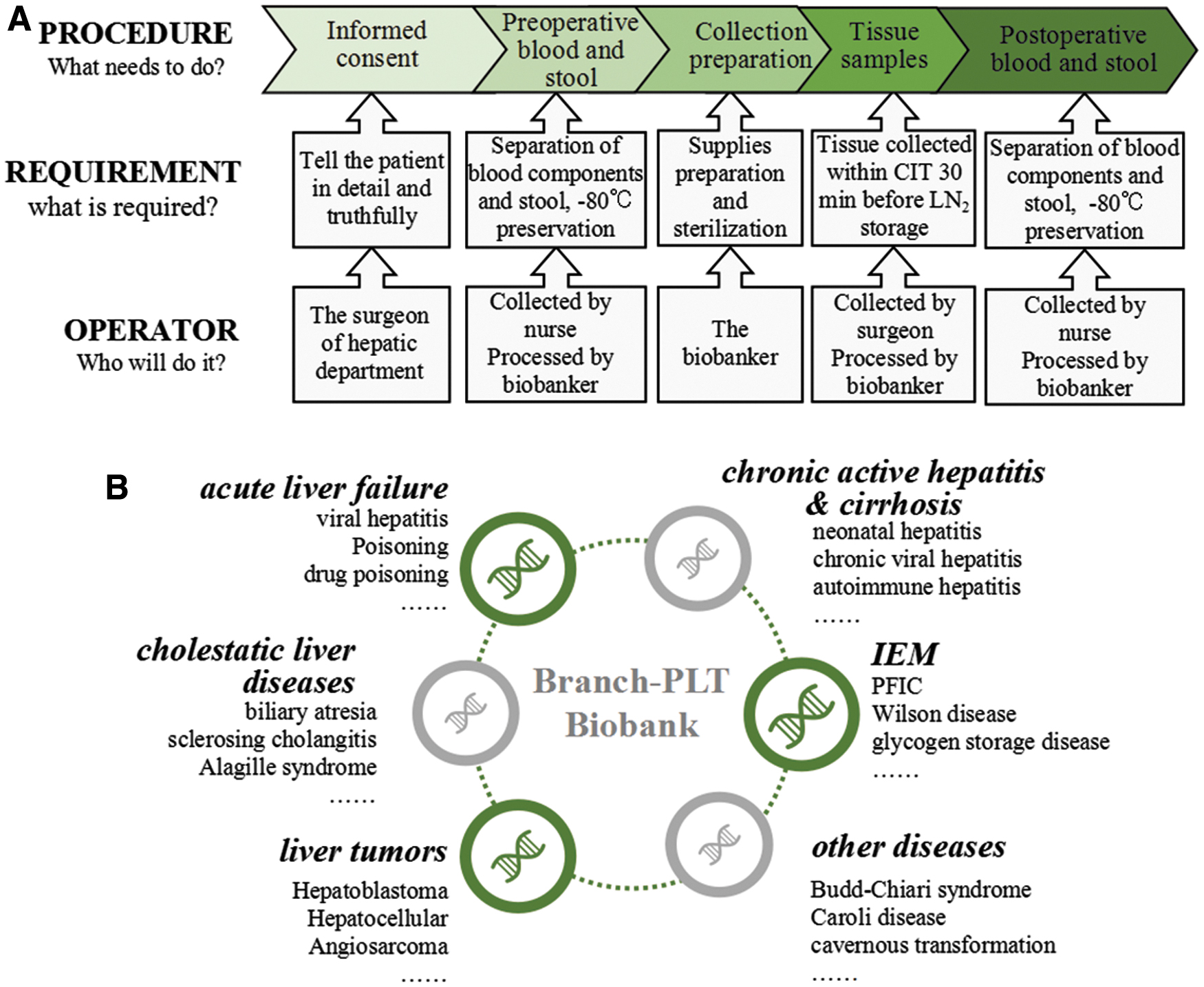
The procedure of sample collection and Branch-PLT biobank setting.
Blood sample collection and processing
Since children undergoing LT are generally younger, blood samples should be collected as little as possible. Two milliliters of anticoagulant and non-anticoagulant blood are, respectively, extracted. The donor was generally an adult, and 5 mL of anticoagulant and non-anticoagulant blood was, respectively, extracted. We collected blood samples from the recipients at admission, before surgery, during postoperative hospitalization, and each follow-up after discharge. At the same time, we collected blood samples from donors before surgery. The specific sample type and volume are shown in Table 2. And the specimen collection protocol is summarized in Figure 2A. It is important to note that we can only take tissue samples from DCD.
Blood samples should be stored temporarily at 2°C–8°C after collection, and processed and stored as soon as possible (<24 hours). Serum or plasma separated from whole blood is dispensed into several (about 2–3 tubes) cryopreservation tubes (500 μL/tube) and stored below −80°C. The brown-yellow layer is stored below −196°C after adding cryoprotectant. Anticoagulation can extract whole blood, plasma, buffy coat (including white blood cells), and red blood cells, which can be used for nucleic acid detection and live-cell extraction. Different types of anticoagulants also have an impact on subsequent studies.8–10 Ethylene diamine tetraacetic acid anticoagulation tubes are commonly used for blood collection. Non-anticoagulated serum and blood clots are available for DNA genotyping and other metabolite studies.
Stool sample collection and processing
We mainly collected stool samples of the recipients at admission, before surgery, daily after surgery, and at each follow-up. These samples can be used for research such as intestinal flora. Specific sample type and volume are shown in Table 2
Clinical information collection
As the core of biobank management, we use a data management system for tracking the collection, processing, and distribution of material. The system is also used for the management of clinical information about the samples, storage of identifiable, and patient personal information. Biobank-IT connects with clinical information are summarized in Figure 3. Login ID and password need to be provided when logging into the system, which is located on the CHCMU encrypted server and is accessible only to study personnel. A unique biospecimen ID will be given to each sample. The biobank identifies each specimen by the ID and stores the specimen securely in the locked facility. Identifying information of all password-protected databases is only available to authorize liver surgery department personnel. Information such as user login, data entry, and editing are recorded and available for future review.
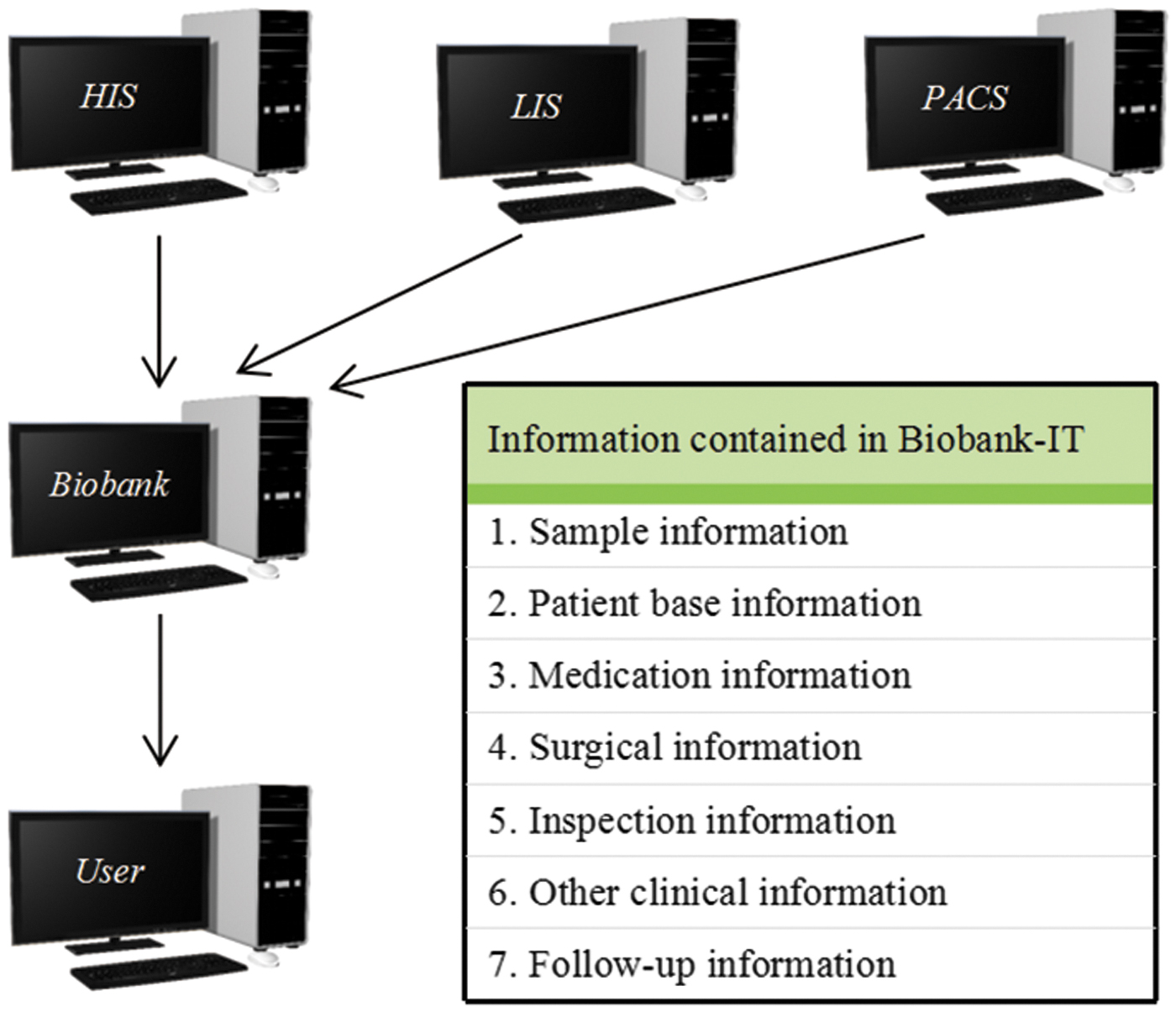
Biobank-IT concept to connect with clinical information.
Branch-PLT biobank setting
According to different disease types and causes of disease classification, we set up a sub-biobank (Fig. 2B), currently divided into six major categories: (1) cholestatic liver disease, including BA, sclerosing cholangitis, and Alagille syndrome; (2) inborn errors of metabolism, including progressive familial intrahepatic cholestasis, hepatolenticular degeneration (Wilson's disease), glycogen storage disease, and citrin deficiency; (3) acute liver failure, including viral hepatitis, poisoning, and drug poisoning; (4) chronic active hepatitis & cirrhosis, including neonatal hepatitis, chronic viral hepatitis, and autoimmune hepatitis; (5) liver tumors, including hepatoblastoma, hepatocellular carcinoma, and angiosarcoma; and (6) other diseases, including Budd-Chiari syndrome, Caroli disease, and cavernous transformation, and gradually enrich the branch-PLT biobank according to the situation of patients admitted.
Quality control
We maintain the quality of biospecimens and associated data collections as per the guidelines published by ISBER and ISO20387. Biospecimen collection, transportation, warehousing, storage, and sharing are carried out within a quality management system (Fig. 4): (1) in the collection session, we mainly record the type of anticoagulant, duration of resting, and temperature, the cold ischemic time of the tissue, and the resting time and temperature of the stool sample. These factors will affect the quality of the sample. (2) In the transportation session, the shipping temperature needs to be appropriate and the shipping time needs to be as short as possible. (3) At the time of warehousing, we ask that all information about the sample be carefully checked. (4) During storage, samples are evaluated every 6 months. We randomly take different kinds of samples according to a certain ratio. DNA and RNA are extracted and their quality will be checked. We present a quality control result of blood samples (Supplementary Table S1). Each storage equipment was equipped with a temperature monitoring system. Provision was to be made for the central alarm system (24 hours/7 days) and technical services will be available for emergencies. (5) During sharing, we ask that all information about the sample be carefully checked. We need to ensure that the sample quality is compliant throughout its life cycle.

Quality control of samples throughout their life cycle.
Sharing and interest
Our biobank stipulates to share our resources and informatics. We aim to promote biomedical research in the field of LT in China.
The staff of the hepatic department can directly select the sample after being examined by their project leader. Third-party researchers can search specimens by disease name and sample type through our database website, which is under construction. In the online system, researchers can directly find what samples are in our biobank. All the requests are subjected to ethical clearance, and researchers will also be required to submit a release plan and research program to the review committee. Review committee review of the projects regarding to the scientific nature and importance. Biobank will assist the hepatic department in signing the Sample Use Cooperation Agreement with the third-party units on the premise of protecting their interest such as article signature and patent sharing. The patient identity is classified, and the biobank stipulates specimens that will be used only for purposes cited in the application.
Results
Since 2018, a total of 49 PLTs have been registered. The mean ages of recipients and donors were, respectively, 13.1 ± 19.7 months and 29.1 ± 6.2 years. Males was more represented among the recipients (61.23%; 30/49), while women were more prevalent among parent donors (65.12%; 28/43), which is shown in Table 3. And the most common LT diagnosis is BA (61.23%).
The Basic Information of Pediatric Liver Transplantation Recipient and Donor
Except DCD.
From Aug 2018 to now, we collected 2780 samples as shown in Table 4. There are more blood samples than tissue samples. Among blood samples, postoperative blood samples are the most, the plasma of the follow-up period in the least. Among tissue samples, recipients' samples are more than donors. And the lymph node samples are the least of all tissues.
The Number of Samples Collected
Discussion
As far as we know, this is the first PLT biobank in China, which effectively provides the shortage of resources in scientific research on PLT. This article illustrates the design and implementation of a biobank for clinical information and biospecimens in children with end-stage liver and bile disease. Several adult LT biobanks have been established in China, such as the Armed Police General Hospital LT biobank, Qidong liver cancer biobank, and liver cancer biobank of Zhongshan Hospital. 11 In 2018, India's National Liver Disease Biobank also clarified the importance of building a national liver transplant sample bank. 7 It can be seen that the trend of establishment of a Chinese child LT biobank is upcoming.
The ultimate goal of biobank construction is to transform the advantage of biological sample resources into clinical and scientific research. There is a lot of research in the field of LT in children, and significant progress has been made into the therapy method. However, the complex genetic, biological, and interacting environmental mechanisms contributing to an end-stage liver and bile disease are not clear. Several successful international biobanks have supported many scientific discoveries in this area to date, but have collected limited amounts of clinical information, restricted sample collection to adult samples.11–13 At the same time, there is a lot of research in the field of LT in children, and there is great demand for high-quality biological sample resources. No standardized PLT biobank has been established before ours, and no standardized methods and procedures of specimen collection, treatment, and preservation have been formed.
The authors collected more than 2000 tissue, blood, and stool samples from liver transplant donors and recipients since August 2018. The establishment of the clinical biobank requires the review and evaluation of the ethics committee to collect the patient's specimens legally. 14 On this basis, after the patient signs the informed consent, the specimen of the transplant patient will be collected by professional personnel. The collection and preservation of blood and tissue specimens is collected and preserved by full-time technicians under the same conditions, to avoid artificial deviation caused by improper operation without professional training. Also, the biobank of CHCMU has established a system, which connects to the clinical information system and is used for the management of clinical information about the samples. So it has relatively complete information about long-term postoperative follow-up of patients.
There are specific ethical issues involved in the inclusion of children's samples in biobanks. One of the main issues is how to appropriately involve children in the consent process. Referring to the Guidelines for Ethical Review of Drug Clinical Trials in China, special attention should be paid to the following points: (1) in principle, it is prohibited for children who are incapable of giving consent to participate in clinical research. However, if the child has an end-stage disease, the ethics committee will determine whether the child will benefit from the research. The child may participate in the research with the consent of the child's parents/legal guardians and the special approval of the ethics committee. (2) Considering the knowledge level of the participants, easy-to-understand expressions and appropriate reading lengths should be used. At the same time, we can also design different versions of informed consent for children, such as videos, animations, and other forms of expressing informed consent. (3) The risks of the study and special risks that cannot be foreseen now should be described in detail. (4) Investigators should prohibit the use of inducements such as free of charge and exaggerated efficacy to participants. Verbal promises of noninformed consent should also be prohibited. (5) Informed consent should be conducted in a quiet, private place, allowing sufficient time for the child and parents/legal guardians to make decisions. Repeatedly inform and re-explain questions or problems until they are fully understood. (6) Researchers should integrate informed consent throughout the research process. Children and their parents/legal guardians are promptly informed of new information that may affect their willingness to continue participating in the study. At the same time, the researcher should dynamically assess the children's cognitive abilities and seek the children's consent to the extent permitted by the children's developmental and intellectual level. (7) The children's admitting or bedside physician should be prohibited from participating as an investigator in the process of obtaining informed consent. This is because it may result in the children's parents/legal guardians being forced to participate in the study for fear of subsequent treatment.
Specimen quality control is the key to the establishment of a standardized biobank. Our established quality control system includes complete hardware facilities, standardized operation processes, scientific clinical information-sample information management systems, and professional technical personnel. Tissue specimens were collected in strict accordance with the requirements of the ISBER and standardized operation process. Organization's CIT within 30 minutes after in vitro will be put into LN2 frozen. The CIT is vital for the quality of preservation. Most scholars recommend specimens should be processed within 30 minutes after removal of materials, to avoid the degradation of genome DNA, RNA, and protein. 15
Given the small total number of liver transplant samples in children and the complexity of the sample acquisition process, the value and rarity of high-quality biological samples are highlighted. The use of LT samples in children should be carried out on the premise of ethics, and the applicant should provide a sound application plan and expected results, which can only be used in related research after the scientific demonstration. The application process should be monitored throughout, and if biological samples do not meet expectations, the procedure should be terminated immediately to avoid a waste of resources.
High-quality clinical specimens are a prerequisite for scientific research. The standardized PLT biobank that provides valuable clinical sample resources can not only fully protect the rare children's LT specimen resources but also can ensure the accuracy of the scientific research. Therefore, a standardized PLT biobank can promote the development of children's end-stage liver disease research, which has especially important medical significance.
Footnotes
Authors' Contributions
Y.Z. conceived the study and is the principal investigator. Y.Z. initially designed the study protocol. M.Z. coordinated the doctors and nurses. At the same time, M.Z. mainly provided clinical support and lead surgery. Z.X. and R.W. contributed to subsequent amendments to the study protocol. Z.X. and R.W. wrote the first draft of this article. Y.Z. and Z.X. revised this article. All authors are responsible for the coordination of sample collection and data management. All authors contributed to subsequent drafts and approved the final article.
Acknowledgments
The authors would like to thank all families who generously accept to participate in this study. The authors would like to thank the doctors and nurses of CHCMU for their facilitation of patients for the study. The authors also gratefully thank Yuhan Xiong for his outstanding work in language editing.
Ethical Statement
A parent/primary caregiver for each child provided written informed consent for their child and themselves to participate in the study. Children older than 7 years could provide written or verbal assent if their parent deemed them cognitively able to understand the study requirements.
Author Disclosure Statement
No conflicting financial interests exist.
Funding Information
This study has not received any funding.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.