
Abstract
Purpose:
The number of bone allograft transplantations required in low- and middle-income countries (LMICs) is growing very quickly. No previous study has investigated the challenges clinical banks face to sustain operations or meet this demand. The purpose of this study was to conduct a systematic review of the barriers to implementation and sustainability of clinical bone tissue banks in LMICs. Barriers identified in clinical bone banking can shed light on strategies for overcoming obstacles in other biobanking programs.
Methods:
A systematic review protocol was registered with PROSPERO under identification number CRD42019136045. LMIC was defined using World Bank criteria. A search strategy targeting PubMed, Cumulative Index of Nursing and Allied Health Literature (CINAHL), and the World Health Organization (WHO) Global Health Library was used. Studies from the inception of bone banking until June 4, 2019, that discussed an identifiable barrier to bone banking were included. Study quality was assessed using The Critical Appraisals Skills Programme (CASP) Qualitative Checklist.
Results:
Of studies identified, 33 studies were included in the final analysis. Based on the full-text review, the primary barriers identified were lack of regulation, low donor rates, and insufficient training and staffing. CASP analysis performed on the 24 qualitative articles showed an average of 3.6 qualitative measurements met.
Conclusions:
As international organizations such as the International Atomic Energy Agency (IAEA) restructure their participation in global bone banking regulation, these barriers such as lack of regulation, low donor rates, and insufficient training and staffing could pose a challenge to meeting the rising demand for bone transplantation in LMICs. Articles with higher quality evidence are needed to better define barriers and propose evidence-based solutions.
Introduction
There are many types of biobanking; these include research biobanks, which store biospecimens for testing, and clinical biobanks, which prepare specimens for therapeutic interventions and reconstruction. 1 Research and clinical biobanking can be further differentiated by their predominating challenges. While research biobanks must prioritize consent and privacy, clinical biobanks have the added responsibility of maintaining safety for future transplant or therapeutic use. This article will predominantly focus on clinical biobanking; however, these authors believe that all subtypes of biobanking can learn from the experiences of their sister organizations.
Bone banking is unique because it is one of the few types of tissues that can be used for research as well as transplantation. Because of this advantage, the development of bone banks across the world has opened new opportunities in reconstructive musculoskeletal surgery. Allografts consisting of the bony matrix of cortical and cancellous bone are recovered from living donors during routine orthopedic procedures, such as a hip replacement or from cadaveric donors. These grafts are processed to reduce risk of immunogenicity, sterilized to eliminate bacterial burden, and stored in anticipation of future therapeutic use, especially for the replacement of lost musculoskeletal tissue. Applications for these bone allografts include patients with bone loss due to high-energy traumas, osteolysis, or infection, or who underwent necessary bone resection due to malignancy. 2
While bone banks provide an essential service to patients requiring bone transplantation, these facilities face high costs and several complex barriers. In the last 30 years, there has been a significant increase in the number of bone banks in low- and middle-income countries (LMICs), largely due to the International Atomic Energy Agency's (IAEA) financial commitment and policies. According to the IAEA, “the growth and output of tissue banks have been exponential. Up to the year 2001, the program has helped to produce 222,580 tissue grafts with a value of $U.S. 51.8 million. 3 ” Despite this growth, a number of bone banks will be unable to meet the supply to support the projected number of allografts required in coming years. This study seeks to answer the following question: what are the barriers to implementing and sustaining bone banking programs across all LMICs?
Materials and Methods
Search strategy and selection criteria
A comprehensive search strategy using high-quality databases was used in this review. These databases included PubMed, Cumulative Index of Nursing and Allied Health Literature (CINAHL), and the World Health Organization (WHO) Global Health Library, and were chosen for their inclusion of international peer-reviewed research. The databases did not exclude gray literature. The systematic review organization software, Covidence, was used.
The search strategy is included in Appendix A1. The study's compliance with systematic review guidelines was published with The International Prospective Register of Systematic Reviews (PROSPERO) database under identification number CRD42019136045. The search dates were from database inception to June 4, 2019. Inclusion and exclusion criteria are listed below:
A. Inclusion criteria: All study types regarding the barriers to the implementation and sustainability of bone banking programs in LMICs were considered for inclusion. B. Exclusion criteria: A lack of sufficient information contained within the full text of the study regarding this topic; if the article was not an original, full-text, research study; if there was not an English translation of the article available; animal and nonhuman studies.
Data extraction, analysis, and quality assessment
Covidence was used to organize, include, and exclude studies for final review. Each article underwent a systematic screening process as follows: two reviewers evaluated each abstract; to advance to full-text review, each article required both reviewers' approval. 4 If a discrepancy was present, a third reviewer assessed the abstract to resolve the conflict. After abstract screening, two independent reviewers examined the full-text articles, and conflicts were resolved via a third reviewer not involved in the initial screen. Articles included in the final review underwent data extraction and qualitative analysis.
Data extraction examined articles for inclusion of the following barriers: equipment and finance, governance and regulation, training and necessary staffing, donor availability, procurement, processing, sterilization, preservation, tracking and notification, and ethical/cultural considerations (Table 1). Major barriers within each category were compiled and analyzed. The Critical Appraisal Skills Programme (CASP) assessment tool was utilized to assess the quality of qualitative articles. A separate quantitative analysis was not performed for quantitative articles, as the results did not pertain to barriers to bone banking, only their qualitative commentary. Table 2 details the Qualitative Checklist, which was used to assess 24 articles. Qualitative synthesis was determined appropriate for these studies; as such, a meta-analysis was not utilized. Biases in data analysis include the removal of non-English language studies, an overrepresentation of articles with similar authors, and an underrepresentation of countries analyzed.
Barriers Identified Among Articles Included in Full-Text Review
, Barrier present.
Critical Appraisal Skills Programme Analysis of Qualitative Articles Included in Full-Text Review
Per CASP instructions: CT, can't tell; N, no; Y, yes.
CASP, Critical Appraisal Skills Programme.
Human and animal rights
No human or animal subjects were recruited for this research study.
Results
A total of 2913 studies were identified after the database search, 86 of which were duplicates and subsequently removed, leaving 2827 available abstracts. After abstract review by 4 independent researchers, 94 studies were selected for full-text review. Of the total studies identified, 33 studies were included in the final analysis. Figure 1 outlines this process of inclusion for final full-text review. The majority of excluded studies did not discuss specific barriers to bone banking. For the final analysis, nine studies were conducted in LMICs located in the Americas (North, South, and Central), nine in South Asia, eight in East Asia, two in both South and East Asia, three in the Middle East or North Africa, one in sub-Saharan Africa, and one in Europe. Based on the full-text review, the primary barriers identified were lack of regulation, low donor rates, and insufficient training and staffing.
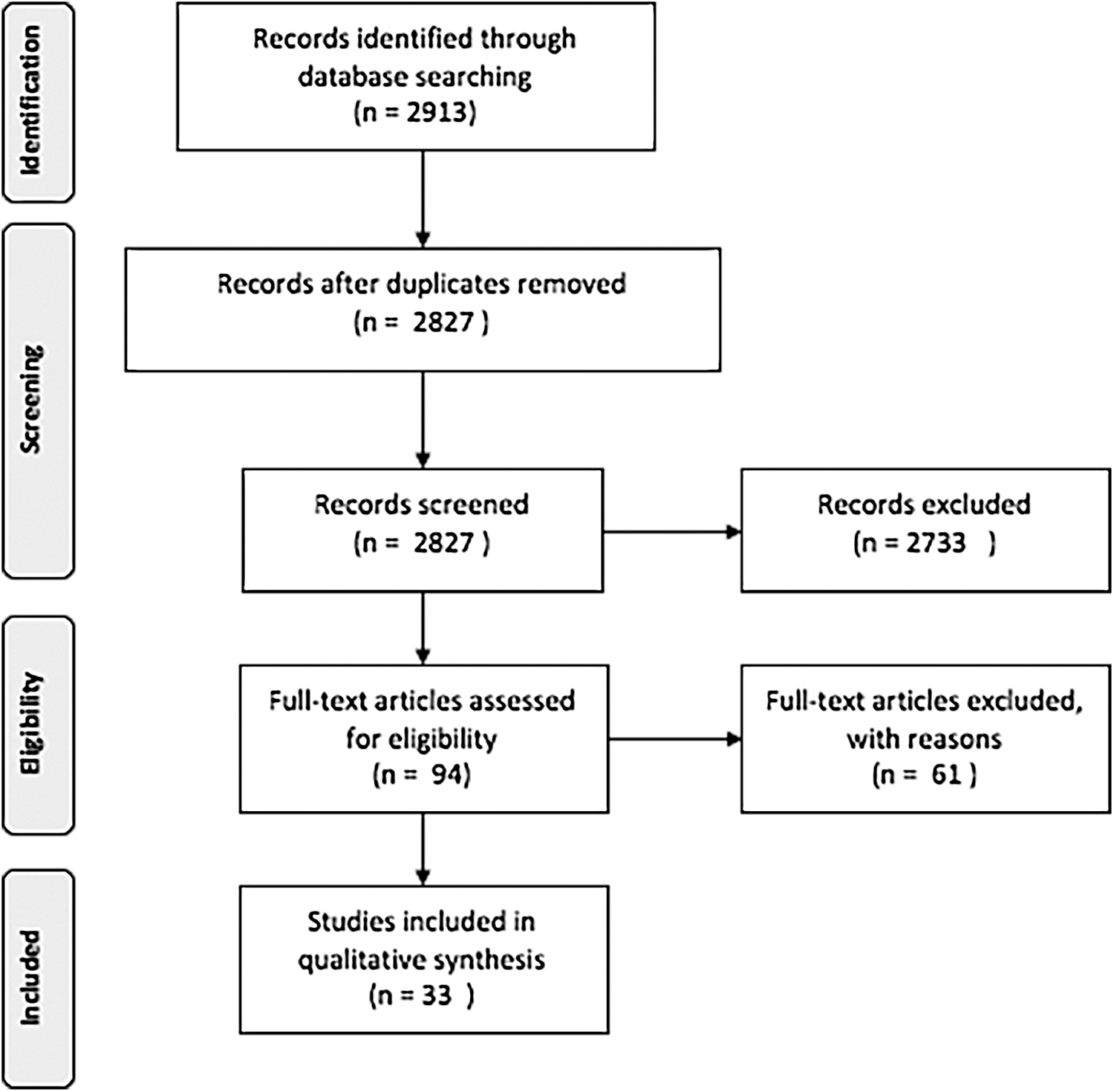
Process of inclusion for final full-text review.
Years of publication ranged 20 years, from 1999 to 2019. The majority of studies, 58%, discussed bone banking in Southeast Asia, followed by 27% in the North, Central, and South Americas, and 15% discussed Africa, the Middle East, and Europe. The two types of research that were represented in these articles were qualitative and cohort studies. The majority were qualitative studies, most of which focused on documenting the evolution of bone banking within a particular country or group of countries, including current barriers. The other 27% of articles were structured as cohort studies. Over 50% of articles included the following barriers: regulation (70%), donor availability (64%), training/staffing (58%), and ethical/cultural considerations (52%). All other barriers were reported in fewer than half of the articles.
Bias within and among studies was reported via CASP assessment (Table 2).
Regulation
Regulation was defined as the governance, procedures, and legal processes involved in creating and operating a functional bone bank. Of the 33 articles included in the final analysis, 23 (70%) identified barriers to the regulation of bone banking activities, including a lack of regulatory oversight by a unified body, competing recommendations from international and national organizations, and varying quality measures between banks within the same country.
Donor availability
Donor availability was defined as donor recruitment, quantity of donations, and quality of donations. Of the 33 articles included in the final analysis, 21 (64%) discussed donor availability challenges in the establishment of a tissue bank, including lack of public information, donor screening difficulties, and high costs without adequate funding. Local governance and cultural context also represented important considerations in the development of successful bone banks. Seventeen of the 33 articles (52%) included in this review detailed the ways in which local issues, including variations in consent processes, language barriers, perceptions around donation, and differences in regulatory framework, contributed to operational efficiencies and developmental opportunities.
Training and staffing
Staffing was defined as the personnel required to operate a bone bank. Training was defined as the qualifications and/or skills that staff require to operate a bone bank. Nineteen of the final 33 articles (58%) discussed staffing and/or training. Barriers to staffing included limited finances for hiring bone bank personnel, a scarcity of secretarial support for tracking tissues, and the need for a new generation of leadership, as older personnel retired from their positions, particularly as demand continues to increase. Barriers to training of bone bank staff included a lack of standardization and the financial strains of enrolling in or creating training programs.
Ethical and cultural considerations
Ethical and cultural considerations were defined as country-specific customs, context, or religious concerns that influenced establishing and maintaining a bone bank. Seventeen of the final 33 articles (52%) discussed these topics. Country-specific ethical considerations included religious concerns and the public perception of the health care system.
Equipment and finance
Equipment was defined as the materials and machinery needed to operate a bone bank. Finance was defined as the monetary resources and funding for the development and maintenance of bone banks. Thirteen of the final 33 articles (39%) discussed barriers to acquiring the appropriate equipment and/or financing.
Procurement
Procurement of tissues was defined as recovering tissues from screened donors and transporting specimens to an appropriate processing center. Nine of the final 33 articles (27%) commented on barriers to procuring tissues.
Sterilization
Sterilization was defined as the reduction or elimination of bacteria, viruses, and fungi from bone allografts. Eight of the final 33 articles (24%) discussed barriers to achieving allograft sterility, including both the inability to achieve primary sterility and the inability to maintain sterility.
Processing
Processing was defined as macroscopic cleaning, laboratory testing, and initial packaging of tissues. Four of the final 33 articles (12%) discussed barriers to processing tissues.
Preservation
Preservation was defined as the long-term storage of tissues and their preparation for transplantation in the perioperative time period. Four of the final 33 articles (12%) discussed barriers to the preservation of bone allografts, with 3 commenting on the financial barriers versus sterility benefits to the various methods of preservation, including deep freezing, freeze drying, and ethylene oxide.
Tracking and notification
Tracking was defined as labeling allografts and internal record keeping. Notification was defined as external communication with physicians and patients utilizing the tissues. Three of the final 33 articles (9%) discussed specific barriers to tracking, and of those 3, only 1 mentioned notification specifically.
CASP analysis
Of the 33 articles included in this systematic review, 24 articles (73%) were qualitative in nature. To assess the overall quality of the evidence, a CASP analysis was performed (Table 2). All 24 articles were assessed against 10 quality measures. The average number of quality measures met was 3.6, ranging from 1 to 9 quality measures met.
Discussion
Key barriers: regulation, donor issues, training/staffing
Of the challenges reported in the results, barriers pertaining to regulation, donor availability, and training and staffing were most frequently discussed. All other barriers were reported in fewer than half of the articles.
Regarding regulation, the IAEA featured prominently in the majority of discussions surrounding governance and regulation in bone banking across the world. Outside of regulatory guidance, bone banks may also reference the IAEA's resources for governance templates and best practices before becoming accredited or certified as a member. Some countries that initially attempted local- or state-level oversight for bone banking later consulted the IAEA to provide feedback regarding the quality of services.
In India, for example, the Transplantation of Human Organs Act of 1994 serves as the technical national legal framework for bone bank operation. 17 The legislation, however, has not been implemented equally across Indian states, and only certain regions adhere to the guidelines. The IAEA stepped into an audit role to oversee bone banking quality, and provided quality scores to regional centers to increase standardization across bone banking centers in the country. Gajiwala identifies the primary barrier to oversight in India to be inadequate legislation and state support for tissue donation.16,18 Malaysia has similarly incorporated IAEA standards. 32
Argentina's regulatory body, the National Unique Coordinating Central Institute for Ablation and Implant (INCUCAI), on the contrary, independently regulates all organ donation activities, and provides accreditation for tissue banks. 7 No studies compared outcomes between IAEA-regulated bone banks versus those functioning independently. Several articles identified the need for standardization across countries. Aghayan et al. recommend standardization across tissue banks within and outside of Iran via a regulatory body, which would serve to develop policy, as well as tracking tissue samples via an electronic record. 33 While several articles also identified financial issues as a core barrier to successful tissue banking, many countries have folded their own regulatory body into the IAEA, and are drawing on their resources.
Donor availability was another key barrier reported in the literature. A lack of knowledge about bone banking among the public was viewed as a reason for low donation rates. As such, countries proposed creative solutions for spreading information to the public and among clinicians. Bangladesh developed a web page that offered information about the country's tissue bank, arranged 20 seminars across districts, and coordinated meetings between physicians to increase professional awareness. These efforts correlated with an increase in the collection of discarded surgical tissue. The professional awareness campaign led the Tissue Banking and Biomaterial Research Unit to expand bone tissue collection. 22
In Mexico, a 2002 advertising campaign led by a government agency shared messages on television about the number of patients on the waiting list to receive an organ or tissue transplant, and the high-quality medical professionals who participate in this process. 5 Another challenge discussed in 5 of the 21 articles citing donor issues was difficulty with uniform donor screening. Hovanyecz et al. pointed to challenges in initial screening. The Biotar Tissue Bank screening was described as being both “not as rigorous as it is for blood donation” and that “the patient is not as aware that full information on their health status should be provided. 8 ” The financial resources needed were discussed as a hurdle. Herson et al. explained “pricing and reimbursement through the public health system is lacking in efficiency. 7 ”
In systems where the public health system has inadequate resources, there is concern about the private sector taking over. If an unregulated private sector became the primary distributor, experts worry about a fair distribution of tissues, as well as appropriate quality. Kairiyama and Morales Pedraza particularly pointed to the cost of imported sterilized grafts from the United States, which may cost three to four times the amount than those from Argentina. 9
Of the 20 articles relating to training and staffing included in the final analysis, 1 article described that training was not standardized. 33 Another article explained that approval for an MSc in tissue banking was obtained, but no student completed this course due to its length of study; this program was modified to be an Advanced Training course. 30 Recommendations for improved training included quality assurance, additional professional education to better promote the utilization of bone grafts and avoid complications, and general training of medical personnel and tissue bank operators.
Ethical and cultural considerations to bone bank operation
Various studies reported ethical and cultural influences on bone bank operation. Religious views worked to encourage or discourage donation, depending on the cultural context. In Iran and Morocco, for instance, where Islam is the dominant religion, religious guidance “encourages and authorizes organ donation and regards it as a gesture of benevolence and solidarity. 35 ”
In Bangladesh and India, on the contrary, people do not donate portions of their deceased loved ones due to religious beliefs. 22 Overcoming a pervasive distrust of the health care system in many communities is a barrier to building successful tissue banks. Gajiwala described that “some are afraid that the hospital will sell the tissues for a profit. 15 ” Another article pointed to the “fear of legal repercussions of unknowingly participating in illegal organ selling. 16 ” An analysis of Mexico's tissue banking described a “distrust [of] the health system related to good use of donated organs and tissues. 5 ”
One pitfall of the IAEA and other standardization bodies may be the heterogeneous ethical and cultural landscape in various LMICs, and associated donor issues. Such issues emphasize the importance of decentralized standardization, so that those operating bone banks within those contexts do so in a culturally appropriate manner, while maintaining quality and efficiency.
Logistical barriers to bone bank operation
The first logistical barrier we focus on is the equipment and financing required for bone banks. With regard to equipment, these articles suggest that when bone banking is stripped down to its necessities, it can be accomplished using simple technology, such as freezers11,35 or a basic refrigerator.11,19 Chemicals, such as HCl and ethanol, 19 and irradiation technology 15 have been made more accessible and affordable over the last 50 years, and no longer represent the chief obstacles to biobanking in LMICs. Regarding financial support for bone banking, while finance will always be an underlying challenge for any clinical biobank, the articles indicate that this barrier is now greatly reduced due to the international funding efforts of large biobanking support organizations.6,11,15,32
In terms of procurement, a majority of the barriers discussed had implications for sterility; therefore, these two categories will be discussed in tandem. Incomplete screening of donors for disease, 34 location of procurement (operating room versus elsewhere), 5 timing of procurement after donor death, 25 and a variety of technical aspects of procurement13,37 all have implications for the level of tissue sterility. Articles discussing procurement commented on physician requirements to function as tissue procurers rather than surgical technicians, 18 the threat of foreign allograft imports reducing resource allocation to home procurement programs, 23 and the presence of restrictive policies guiding procurement.17,30
Both irradiation and chemical sterilization have been used in these articles. While both methods are accessible, irradiation is preferred over chemical sterilization. This technique is favored as it reduces bacterial burden while maintaining the health of the bone, 19 compared with using chemical agents during processing, which can detract from the mechanical strength and osteoinductive properties of the bone allografts.14,20 Despite irradiation being by far the most common effective and financially prudent way to sterilize bone, it does not ensure adequate sterilization in the setting of viral contamination. 10 Therefore, many efforts have been made to screen out donors with viral infections before procurement begins.
Of note, the handling of samples is particularly challenging in the COVID-19 era, as identified by the International Society for Biological and Environmental Repositories (ISBER) COVID-19 Response Task Force. 38 The screening process itself, however, can be very costly, 21 especially in the face of a rise in donor disease burden in some countries. 31 In addition to financial strains, live donors may not adequately participate in disease screening. For example, not all donors may return to the donation center for a second human immunodeficiency virus (HIV) test to account for the window period. 16 Finally, tissues may be contaminated at the time of procurement, which has been found to be increased with inexperienced procurement teams and donor status.25,34 Only one article discussed the inability to maintain sterility, due to the timing of thawing the allograft and the level of experience of the surgical team. 13
The primary barrier for processing bone allograft donations is verifying the health status of donors. This barrier is best exemplified by HIV. Testing for HIV requires two separate donor blood tests. If living donors do not follow-up for a second HIV test, the tissues must then be discarded. 16 Another article commented on the timing of donor blood tests, increasing the risk for hemolysis, false negatives, and increased risk of transmitting disease. 30 Other barriers included not enough processing centers to meet the demand for tissues. 17
With regard to preservation, the articles describe similar methods as those used for sterilization: chemical agents, deep frozen bone storage, and freeze drying. These methods present identical issues for bone integrity as those described for sterilization, which remains a controversial topic among bone preservation experts. It is important to note that while some of these articles compared the finances needed to support these methods, there was no analysis comparing the costs of these three tools against each other. After our review of these articles, we have drawn the conclusion that irradiation or investing in a deep freezer represents a larger upfront cost to bone banks, but these methods preserve the quality of bone allografts and reduce long-term costs. Additional research is needed to compare the costs of these methods.
Tracking and notification were the least mentioned barriers. The three articles discussing these issues noted that using a manual system to track allografts was prone to human error.26,29,33 Those authors suggested that moving from a manual system to an electronic system would eliminate a large portion of errors within the tracking system and allow for improved international communication regarding shared allografts.26,29,33
Quality assessment
Of the studies included in this review, few used a quantitative approach with a research question and hypothesis intended to determine the barriers to bone banking. Therefore, the above discussion resulted from qualitative commentary from authors' firsthand experience. Studies that were the highest quality evidence addressed training and staffing, and equipment and finance, were cohort studies, and included a mix of quantitative and qualitative data. Studies with lower quality evidence focused on single bone banks and reported quantitative and qualitative analysis without details regarding data collection, the role of researchers, and the primary research question.
The overall quality of evidence is a limitation of this study; the average number of quality measures met by each article was just 3.6 out of 9. While there is no numeric threshold to designate a “high-quality” study according to CASP, having a majority of the nine quality measures is considered favorable in qualitative research. 39 In addition, while CASP provides guidance for scoring, use of this tool can be subjective with great interoperator variability.
Future directions
This systematic review is relevant to all bone banking programs and their stakeholders across the globe. Without the definition and description of barriers, it is difficult to craft an appropriate solution. While most countries included in this analysis were influenced by the IAEA and many articles were dedicated to listing the various impacts of the organization, no comparative analysis exists between countries with a history of IAEA influence and countries without IAEA influence. In addition, while it was beyond the scope of this study to investigate the similarities or differences in barriers among high-income countries, investigating the standardization of tissue procurement and safe biobanking in high-income countries, and what tools LMICs may derive from that process, may be of value in future studies.
Important outcomes to study would relate to regulation, donor rates, training and staffing, and financial efficacy. Other opportunities for future study include a comparison of the barriers to clinical bone banking versus those experienced in other types of clinical biobanking, such as skin, stem cells, and corneas. Finally, a juxtaposition between the barriers faced in both clinical and research biobanking can encourage an exchange of dialogue that would benefit both fields.
The practice of tissue banking in LMICs has shown the capacity for both resilience and adaptability, surmounting barriers over time, such as legally defining donor consent, expanding beyond serving single hospitals, decreasing disease transmission, and beginning to institute nationally standardized quality measures. This study found that the three-most common issues faced by bone banks in LMICs were a lack of regulation, low rates of donation, and inadequate training and staffing. Gaining a more thorough understanding of these barriers to success will be vital as international bone banking attempts to meet the growing need for allografts.
Footnotes
Authors' Contributions
All authors contributed to the study conception and design. Material preparation, and data collection and analysis were performed by C.W., S.M., N.R., and H.M. The first draft of the article was written by C.W., S.M., N.R., and H.M., and all authors commented on the previous versions of the article. All authors read and approved the final article.
Acknowledgments
This study required no primary funding source; therefore, no acknowledgment of funding exists for this study. All parties who contributed significantly to this article are authors.
Author Disclosure Statement
No conflicting financial interests exist.
Funding Information
No funding was received for this article.