
Abstract
To evaluate barriers and facilitators of pediatric biobank participation, we studied whether increased awareness of participants about pediatric biobanking changes their opinions on biobanking practices and their willingness to participate in biobanks. Adolescents (14–18 years) in public schools and their parents were invited to participate in a survey either with or without viewing educational material about biobanking before completing the survey. Questions included willingness to donate, consenting practices and use of specimens. Surveys were administered. Nonparametric statistical tests (Mann-Whitney U) were used to test the significance of differences in Likert scale responses between participant groups. A total of 545 participants (219 adolescent and 176 parents with prior awareness about biobanking vs. 106 adolescents and 44 parents without) completed the survey. Participants who had participated in an educational session were more willing to donate compared to participants without this session under three different conditions: a left-over sample, an extra sample at the time of a medical procedure, and an extra procedure. Adolescents without prior awareness were significantly more willing to donate compared to their parents. Parents perceived the need for reconsent more important than children, although it was less important to educated parents versus noneducated parents. Age of assent was lower in the groups with prior awareness and ongoing use of specimens without reconsent was more permissible to these participants. In conclusion, prior awareness of biobanks may facilitate pediatric biobank participation.
Introduction
Advances in biomedical research have greatly enhanced the therapeutic and diagnostic potential of the analysis of patient-derived biological specimens. Biological specimen banks (referred to as biobanks) play a key role in this growing field: they allow for the centralized collection, preservation, storage, and supply of both biological specimens and clinical information. 1 In a biobank, participants often give broad consent for their specimens and information to be used for yet undetermined future studies. This contrasts with a more traditional consent process, in which participants consent to the collection of their biological specimens for a specific study with a particular research question.
Consenting of pediatric biobank participants (younger than 19 years) has additional consenting practice challenges, as child assent must be obtained in addition to parental consent.2,3 Assent is the agreement of a child not able to give legal consent, and the age of assent and assessment of capacity to consent varies by jurisdiction. In addition, whether permission is needed for the continued use of a participant's specimens after they reach the age of majority is currently not well established. 4 It may be important to give these participants a chance to reconsider their biobank participation, given their capacity to consent, but recontacting these individuals can be logistically and financially challenging. 5 The lack of ethical clarity regarding these issues highlights the need for clear and effective communication with pediatric patients and their parents to facilitate their decision-making process.
Previously, Kong et al. studied some of these ethical questions through surveys given to parents and adolescents in hospital clinics and public schools. 6 The survey addressed willingness to donate specimens, appropriate ages for assent, and opinions on reconsent. Significant differences were found between clinic and school participants regarding willingness to donate specimens, with both adolescents and parents from clinics being more willing to donate specimens than those from public schools.
Various factors could have contributed to this difference: participants from the clinics may be more aware of or have experienced the importance of medical research, and may have previously been involved in or informed about biobanks. Through their experience with disease and medical procedures, clinic participants may have felt more inclined to give back through medical research.
Adult studies have found that with increased education, individuals are more willing to donate specimens. A quasi-interventional community-based study on willingness to donate to a Hepatitis B Virus specimen database found that participants were much more likely to donate if they received detailed information about specimen collection, how specimens would be used, and the benefits, risks, and importance of specimen research. 7 Another community-based study found that willingness to donate to a biobank increased following a presentation at a community health fair event. 8
While these latter studies presented the positive effects of education and awareness on willingness to donate specimens, none of them studied pediatric research participation. Therefore, it is unclear whether awareness or other factors affect the willingness to donate to pediatric biobanks in particular. The goal of this study was to investigate whether a brief educational program would increase willingness of adolescents and parents in the general public to donate to a biobank.
Methods
Participant recruitment
Adolescents aged 13–18 from seven Vancouver School Board secondary schools and their parents were invited to participate in this project. Teachers were contacted by the research team with approval from school administrators. In accordance with the Vancouver School Board, signed parental consent was required for students to be eligible for the study.
Study design
This study and all study materials, including educational materials, were reviewed and approved for clarity, objectivity, and accuracy by the Children's and Women's Research Ethics Board at the University of British Columbia. A two-group quasi-experimental study was conducted using surveys to compare attitudes toward biobanking between intervention and control groups. The intervention and control groups were from the same schools and same grades, but there was a year gap between the intervention and control surveys. The control group was done first as part of a previous study and the survey questions were identical to those used in the previous study. 6
Students were given a package to take home containing a letter about the study, a parental consent form, a parental survey, and an adolescent survey. Students were instructed to have their parents sign the consent form and complete the parental survey if interested. On a separate date, students returned with these documents and completed the surveys in-class. Surveys with illegible, irrelevant, or inappropriate responses as well as adolescent surveys without parental consent were excluded from analysis.
Intervention Group (prior awareness)
In class, adolescents in this group were shown a brief 2-minute video about the BC Children's Hospital Biobank (Supplementary Video S1), followed by a 5-minute PowerPoint presentation that went over the rationale, benefits, and ethical issues related to biobanking. Immediately following the video and presentation, adolescents were instructed to complete the survey. The parents in this group were instructed to watch the 2-minute video about biobanking before completing the survey independently of their child and to return their answers to the school in a sealed envelope. Parents did not receive the accompanying PowerPoint presentation.
Control group (no prior awareness)
Adolescents in this group completed the surveys before the 5-minute PowerPoint presentation about biobanking. Parents did not receive the PowerPoint presentation and neither the adolescents nor the parents in this group were shown the educational video.
Statistical tests
Statistical analyses were performed in consultation with a statistician. To test normality of response distributions, Kolmogorov-Smirnov tests were performed on responses to Likert scale questions. The results of this test revealed that the distributions were not normal (p < 0.001), therefore, nonparametric statistical tests (Mann-Whitney U) were used to test the significance of differences in Likert scale responses between participant groups. Responses to the 5-point Likert scale were assigned ranks (1 = Very unwilling, 2 = Unwilling, 3 = Neutral, 4 = Willing, and 5 = Very willing) and mean ranks were compared between groups. The Mann-Whitney U test was also used to analyze the suggested ages at which assent should be asked. Responses to questions involving “Yes”/“Willing,” “No”/“Unwilling,” and “Uncertain” options were compared using the Pearson chi-Square test without correction. A significant difference between groups was defined as p < 0.05 for all statistical tests.
Results
Survey demographics
A total of 389 adolescents and 279 parents completed the surveys (overall response rate was ∼30% among the four groups). Of the adolescents, 106 received educational materials about biobanking before completing the survey and 283 did not. Of the parents, 44 received prior educational materials and 235 did not. The ratio of males to females was ∼1:1 in adolescents with prior awareness (n = 106) versus 1:2 in adolescents without prior awareness (n = 279) (Table 1). The mean age was 15 for both adolescent groups (age range of 13–18). In the adolescent groups with and without prior awareness, 94% and 93%, respectively, identified as not having any chronic medical conditions.
Adolescent Participant Demographics in Groups With and Without Prior Education
Percentages do not add up to 100% due to rounding and partial nonresponse.
Willingness to donate specimens
Participants were given three hypothetical scenarios to rate their willingness (adolescent survey) or willingness for their children (parental survey) to donate a specimen, based on a 5-point Likert scale (from 1 = Very unwilling to 5 = Very willing). Results were compared by mean rank. Scenarios included the following: providing a leftover specimen from a medical procedure (“leftover specimens”), giving an extra specimen while already having a medical procedure (“extra specimen”), and having an extra procedure to donate a specimen (“extra procedure”). In all groups, willingness to donate decreased as the invasiveness of the procedure increased (Fig. 1). Parents who watched the educational video were significantly more willing to allow their children to donate in all three conditions than parents who did not watch the video (leftover specimens: 4.15 vs. 3.63, p = 0.007; extra specimen: 3.90 vs. 3.35, p = 0.008; extra procedure: 3.26 vs. 2.70, p = 0.01, respectively). Adolescents with and without prior awareness did not have any significant differences in willingness to donate in these scenarios (leftover specimens: 4.00 vs. 3.94, p = 0.85; extra specimen: 3.58 vs. 3.55, p = 0.86; extra procedure: 3.26 vs. 3.05, p = 0.10, respectively). In groups without prior awareness, adolescents were significantly more willing than parents to give leftover specimens (3.95 vs. 3.63, respectively, p = 0.007) and have an extra procedure (3.05 vs. 2.70, respectively, p = 0.002), but equally willing to donate an extra specimen at the time of a medical procedure (3.55 vs. 3.35, respectively, p = 0.13). There were no significant differences between the opinions of adolescents and parents with awareness in these conditions (leftover specimens: 4.00 vs. 4.15: p = 0.21, extra specimen: 3.58 vs. 3.90, p = 0.06; and extra procedure: 3.26 vs. 3.26, p = 0.74, respectively).
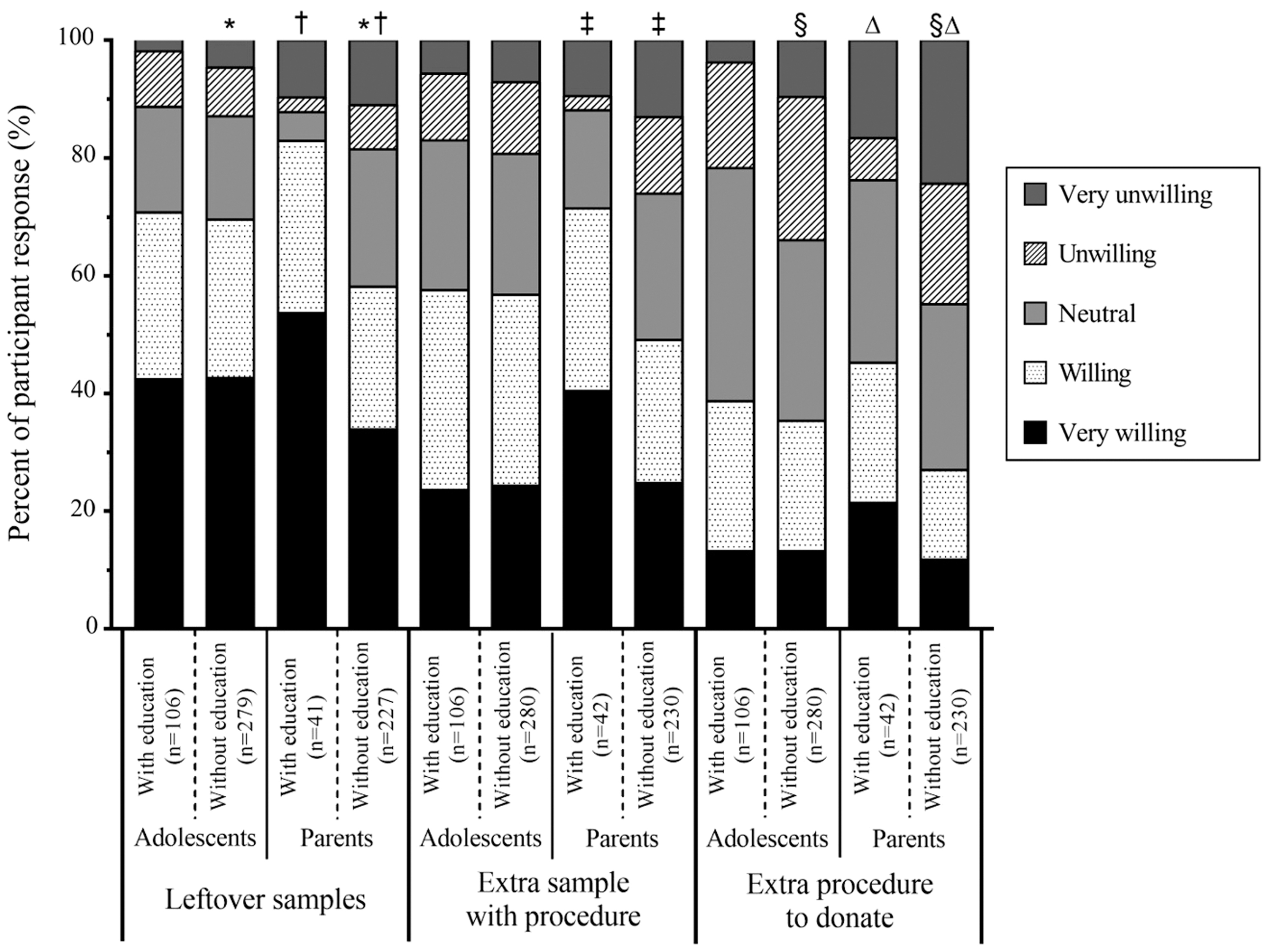
Willingness to donate specimens to a biobank. Bars represent percent of responses from participants with or without prior awareness about biobanking. Participants rated willingness to donate in three hypothetical conditions (leftover specimens, extra specimen during a medical procedure, or having an extra procedure to donate a specimen) using a five-point Likert Scale. Adolescents rated their own willingness to donate specimens under these conditions, while parents rated their willingness to allow their children to donate. Symbols represent significant differences in responses between groups detected using the Mann-Whitney U test. Significant differences were found between responses of adolescents and parents without prior awareness for donating leftover specimens (*p = 0.007) and having an extra procedure to donate (§p = 0.002), and between parents with and without prior awareness for all three conditions: leftover specimens (†p = 0.007), extra specimen (‡p = 0.008), and having an extra procedure (Δp = 0.01).
Participants were also asked about their willingness to donate DNA. Of the four groups, parents who watched the educational video were the most willing to donate DNA (Fig. 2). This group was significantly more willing for their children to donate DNA than the adolescents with prior awareness (3.95 vs. 3.72, respectively, p = 0.02) and parents without prior awareness (3.95 vs. 3.06, respectively, p < 0.001). Adolescents without prior awareness were significantly more willing to donate DNA than parents without prior awareness (3.58 vs. 3.06, respectively, p < 0.001). No significant difference was found between adolescents with and without prior awareness (3.72 vs. 3.58, respectively, p = 0.60).
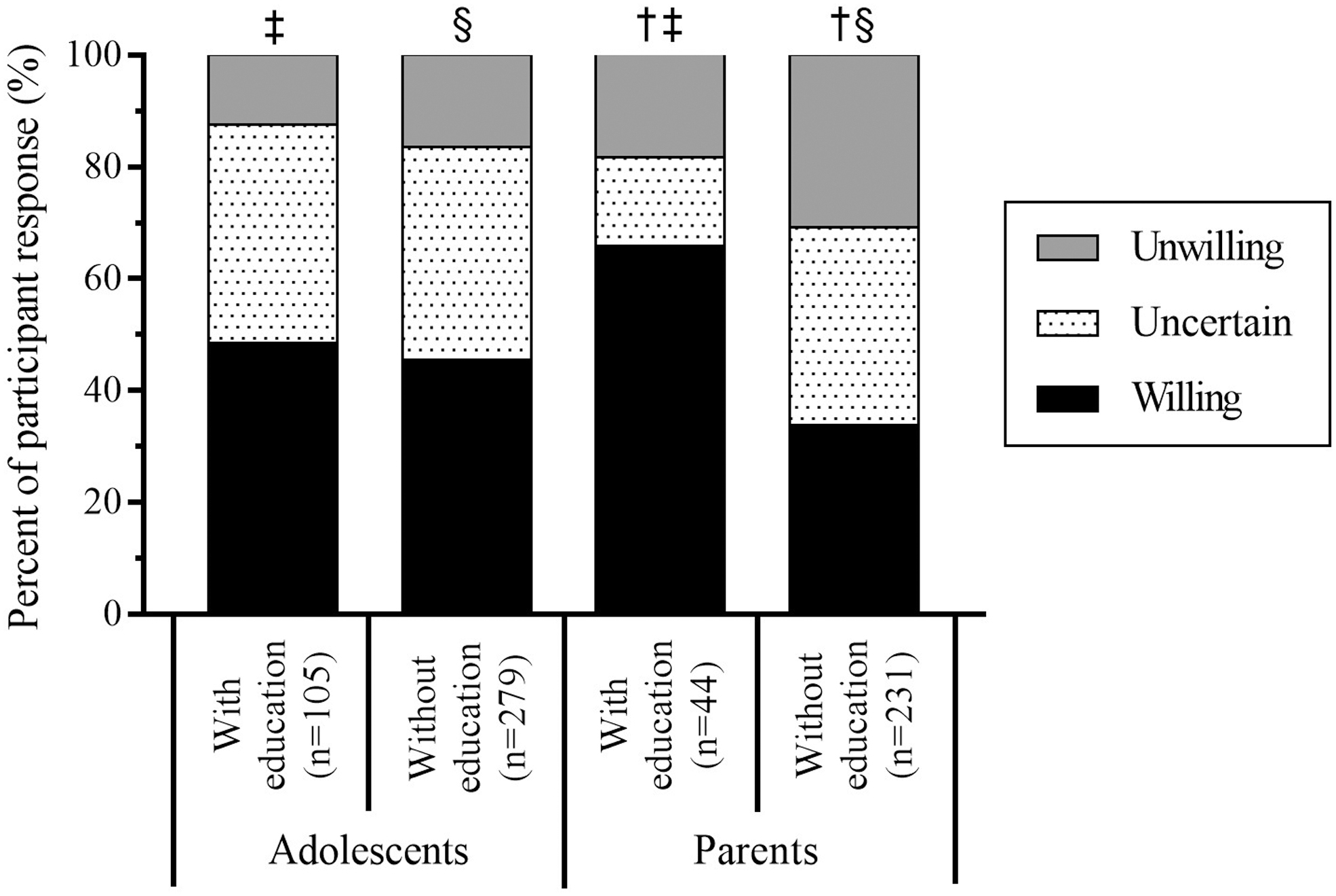
Willingness to donate DNA to a biobank. Bars represent percent of responses (unwilling, uncertain, and willing) from adolescents and parents with or without prior awareness about biobanking. Adolescents rated their own willingness to donate DNA, while parents rated their willingness to allow their children to donate. Symbols represent significant differences in responses between groups detected using the Pearson Chi-Square test. Significant differences were found between responses of adolescents and parents with prior awareness (‡p = 0.02), adolescents and parents without prior awareness (§p < 0.001), and between parents with and without prior awareness (†p < 0.001).
Importance and suggested age of child assent
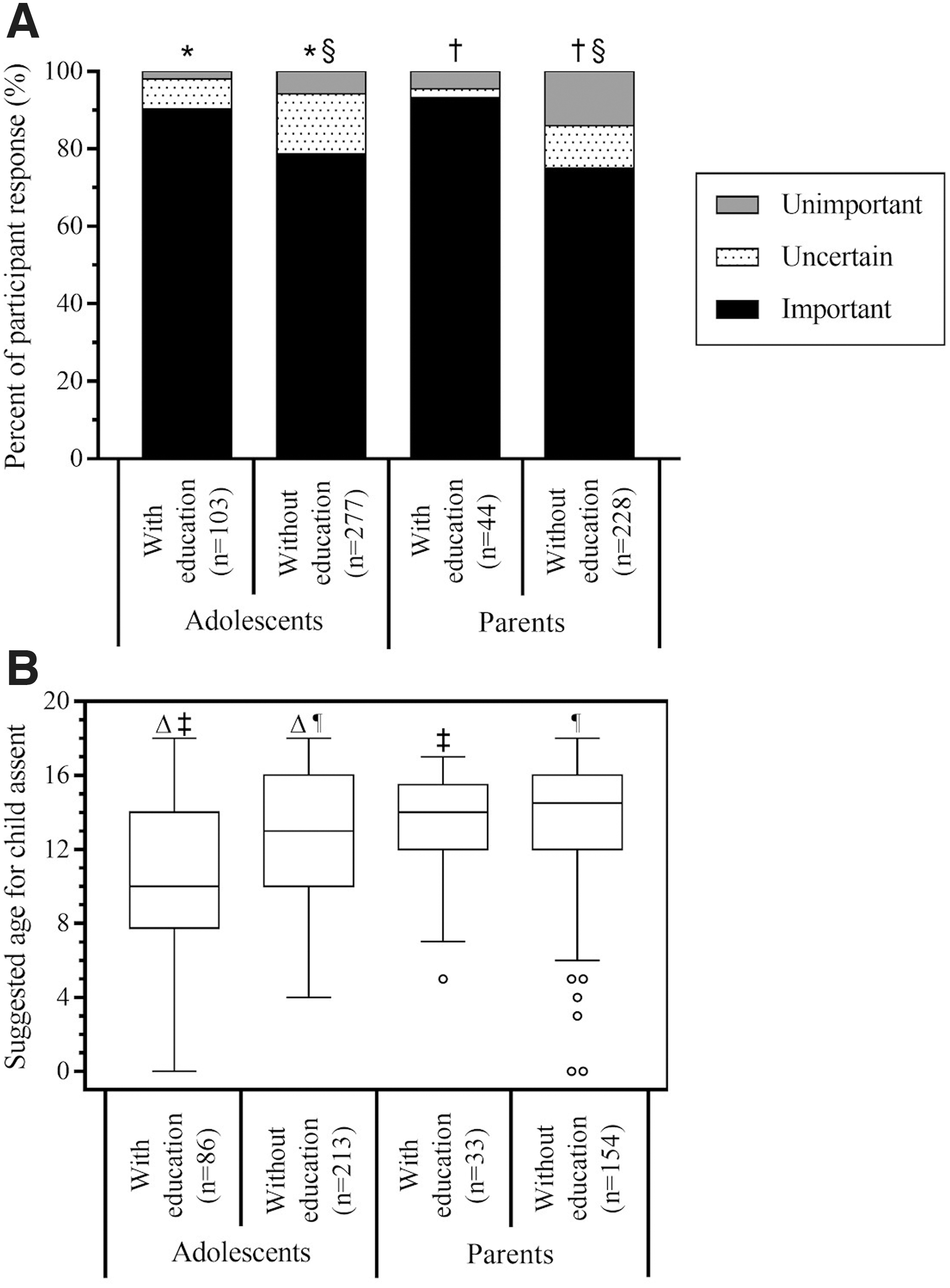
Participants also gave their opinion on the importance of child assent in the consenting process for donating pediatric specimens (important, uncertain, and unimportant). In both adolescent and parent groups, participants with prior awareness felt assent was significantly more important than those without prior awareness (adolescents: 4.77 with awareness vs. 4.46 without awareness, p = 0.031; parents: 4.77 with awareness vs. 4.22 without awareness, p = 0.03) (Fig. 3A). In the groups without prior awareness, adolescents felt that assent was significantly more important compared to their parents (4.46 of adolescents vs. 4.22 of parents, p = 0.004).
Importance
When asked about an appropriate age for child assent, parents in both groups suggested median ages that were significantly older than corresponding adolescent groups (groups with awareness: median 14 years [parents] vs. 10 years [adolescents], p = 0.002; groups without awareness: median 14.5 years [parents] vs. 13 years [adolescents], p = 0.005) (Fig. 3B). While no significant difference was found between parent groups with and without prior awareness (median 14 years vs. 14.5 years, respectively, p = 0.23), adolescents with prior awareness suggested a significantly younger age than without prior awareness (median 10 years vs. 13 years, respectively, p = 0.002).
Importance of reconsent
Both with and without prior awareness, parents felt that it was more important for adolescents to reconsent for the use of their specimens when they reached the age of majority than adolescents themselves (with awareness: 4.11 for parents vs. 3.44 for adolescents: p = 0.001; without awareness: 3.81 for parents vs. 3.57 for adolescents: p = 0.006) (Fig. 4A).

Opinion on importance of re-consent upon adulthood (age 18) for use of pediatric specimens
In the absence of reconsent, parents with prior awareness and adolescents with and without prior awareness had similar levels of approval for the use of previously donated pediatric specimens, with 55%, 51%, and 51% responding with “Yes” for the use of these specimens, respectively (Fig. 4B). Contrastingly, parents without awareness approved significantly less of such use than parents with awareness (2.99 vs. 3.45, respectively, p = 0.03) and adolescents without awareness (2.9 9 vs. 3.58, respectively, p < 0.001).
Written comments
Additional written comments were welcomed from participants in the survey and they are tabulated in Table 2. Overall, written comments were positive in 59% of adolescents with prior awareness versus 46% without and 43% in parents with and 38% without prior awareness. Concerns about the procedure itself were a common theme among adolescents while parents had a wider breath of concerns, including privacy, not knowing the study, and mostly safety or hurting their child.
Comments from Adolescents and Parents With or Without Prior Awareness About Biobanking
Discussion
This study is a follow-up to a study published by our group. 6 This study explored whether prior awareness about pediatric biobanking in a healthy population increases willingness to donate and alter opinions on the consenting processes, as our previous study showed that adolescents visiting the hospital and their parents were more willing to participate in biobanking. We speculated that part of this willingness was the result of potential or perceived benefit this population may have from participating with no direct benefit to the healthy school population. However, we also hypothesized that adolescents and parents visiting the hospital are more familiar and aware of research, privacy, and confidentiality and procedures compared to the school population. This study explores this question by providing the school adolescents and their parents with some educational materials.
The educational materials consisted of a video from the BCCH BioBank as well as a short Powerpoint presentation. Note that the video was created for a target audience of 7–13-year-old children. Topics addressed in the video and presentation included what a biobank is, why samples and data are important for medical research, the assent and consent process, and a few specifics about our biobank.
As pediatric biobanking brings an additional set of challenges and complexities compared to adult biobanking, engagement and trust of participants are paramount. Our study team gathered opinions of parents and adolescents of the general public on pediatric biobanking, as a significant number of our potential biobank participants present to the hospital in acute situations and may have to make decisions about their health care and research participation in a short time frame without being familiar with health care and research. Knowing concerns and opinions from this population in addition to the opinions of patients will inform educational materials and changes to consent content and process. It also helps inform process with regard to reconsent and the use of samples in the absence of reconsent.
Opinions of parents and adolescents without prior awareness differed significantly from adolescents and parents who received educational materials with significant differences in willingness to donate, assent age, and importance of reconsent.
The main concern of adolescents was potential discomfort associated with specimen collection, which was not fully addressed in the presentation or the educational video. 6 Studies on teenagers, parents, and other family members also reported physical pain as one of the greatest concerns among patients considering donating specimens to research.9–12 Clearly, the issue of pain and discomfort with specimen collection needs to be further addressed in pediatric biobanking. While donation of saliva was briefly mentioned in the video, more information about noninvasive specimen collection could encourage donations from individuals with concerns about physical discomfort. This study highlights the need for information about pain and discomfort with specimen collection and the options for noninvasive collections in the consent process or educational materials. Our biobank is currently developing these materials.
In groups without prior awareness, adolescents were more willing to donate DNA than parents. However, when given an educational session about biobanking, the reverse was observed: parents were significantly more willing to donate DNA than adolescents. This variable was important to assess, since a previous study found that parents frequently did not consider the collection and storage of DNA when considering donation of their children's specimens. 13 Parents without prior awareness appear particularly concerned about privacy and potential misuse of such information by unintended parties, such as insurance companies and employers. 11 Parents who watched the video may feel more trustful of the research and biobanking process after learning about the protection of confidentiality and the anonymization process.
Overall, adolescents were found to be more willing to donate to biobanks regardless of whether they had any prior knowledge compared to parents without prior knowledge. These findings may reflect that parents are inherently protective of their children, and therefore prioritize the immediate comfort and safety of their child over possible benefits of research. 12 Adolescents also tend to be more carefree and may not consider biobanking risks as seriously as parents.
Cultural and socioeconomic factors such as religion, collectivism, and education may also play a role in the willingness of parents to allow their children to donate. In a study conducted in China, Qiu et al. found that low education, strong religious beliefs, and having a child with a severe disease were factors that played the greatest roles in parent's willingness to donate. 9 In contrast, communities that hold more collectivist values were more willing to donate to help benefit future generations, as indicated in a study involving Chinese Americans. 14 Religious permission to donate is a strong positive influence in willingness to donate. 15 Future educational programs about biobanking may have greater success if conducted in a culturally and religiously appropriate manner.
The majority of participants felt that child assent was important, although prior awareness only altered adolescent opinions on the importance of child assent (increased with awareness) and the suggested age for assent (decreased with awareness). Perhaps a greater understanding of biobanking encouraged an active role of adolescents in biobank participation and the consenting process. Alternatively, adolescents may have overestimated their ability to comprehend biobanking in a form of the retroactive Dunning-Kruger effect, in which individuals mistakenly overestimate their own competence based on the unawareness of deficits in their own knowledge. 16 The educational video was brief and simple, but did not cover the ethical intricacies and difficulties associated with consent and assent.
Prior awareness among parents also increased their perceived importance of child assent compared to parents without awareness. However, the median suggested ages of child assent between parents with and without prior awareness were not significantly different, indicating that their perceptions of their children's overall ability to understand and make decisions regarding biobanking remained the same. A parent's external view of their child's maturity may be less susceptible to overestimation by the Dunning-Kruger effect, resulting in a more consistent view of their child's maturity at a given age. 16 The inherent protective nature of parents may also contribute to higher suggested assent ages than adolescents.
Adolescents both with and without prior awareness considered the need for reconsent upon adulthood to be significantly less important than corresponding parent groups did. Adolescents may have felt more confident that their willingness to donate would not change upon adulthood, while parents were less certain of their child's future opinion. Parents may also view adulthood as a relinquishment of responsibility over their child, who should then be making decisions for themselves. Note that prior awareness increased the approval rate among parents for use of specimens without reconsent. As the reconsent process remains a resource intensive process and not always feasible, the knowledge that most adolescents would like the continued use of their specimens without reconsent is encouraging. Note that the authors do not suggest that reconsent should not be attempted first.
One of the limitations of this study is that parents who received awareness training by choosing to watch the educational video may have a more positive attitude toward biomedical research and greater willingness to donate. The sample size of this group was also smaller than other survey groups due to nonresponse. These factors may have resulted in bias toward increased willingness to donate and more positive opinions of biobanking within this group.
The total number of surveys distributed was not accurately recorded and so the nonresponse rate could not be quantified. Nonetheless, participation bias may have skewed the results, since participants who feel strongly about biobanking, whether positively or negatively, are more likely to respond to the survey.
Another limitation of this study is that we cannot be sure that parents who received educational materials actually looked at them and parents who were in the control group did not voluntarily looked for information about biobanking before completing the survey.
In summary, this study highlights that awareness of the public about (pediatric) biobanks can increase understanding of medical research, while reducing concerns regarding handling of specimens. For pediatric biobanks specifically, age-appropriate educational materials should be created, addressing issues specific to children such as discomfort during specimen collection. In addition, the inclusion of children in the consenting process is important to them and allows them to understand the importance of research and use of specimens. Increased awareness may lead to improved engagement of the public in pediatric biobanking.
Footnotes
Acknowledgments
We thank the Vancouver School Board and adolescents and parents who participated in this project. We thank Boris Kuzeljevic for his assistance with the statistical analysis.
Author Disclosure Statement
No conflicting financial interests exist.
Funding Information
No funding was received for this article.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.